Edema.physiolgy for ahs students according to shambulingam physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content to compile a thorough, AHS-level edema physiology guide aligned with Sembulingam's approach. Let me compose the full answer:
Edema — Physiology for AHS Students
Based on Guyton & Hall Textbook of Medical Physiology (standard reference aligned with Sembulingam's coverage)
Definition
Edema is the presence of excess fluid in the body tissues. It occurs mainly in the extracellular fluid compartment but can also involve intracellular fluid accumulation.
Types of Edema
1. Intracellular Edema
Swelling within cells. Three main conditions cause it:
| Cause | Mechanism |
|---|---|
| Hyponatremia | Low plasma Na⁺ → osmosis of water into cells |
| Metabolic depression | Cell membrane Na⁺/K⁺ pumps fail → Na⁺ accumulates inside → water follows |
| Ischemia/Inadequate nutrition | ↓ O₂ and nutrients → pump failure → intracellular Na⁺ ↑ → osmotic water entry |
| Inflammation | ↑ cell membrane permeability → ions diffuse in → osmotic swelling |
In severe ischemia, intracellular volume can increase 2–3× normal — often a prelude to tissue death.
2. Extracellular Edema
Excess fluid in the interstitial spaces. Two general mechanisms:
- Abnormal leakage of fluid from plasma → interstitium (across capillaries)
- Lymphatic failure — lymphatics cannot return fluid and protein to blood (lymphedema)
The most common cause is excessive capillary filtration.
Starling Forces — The Physics of Capillary Filtration
Filtration is governed by:
Filtration = K_f × (P_c − P_if − π_c + π_if)
| Symbol | Meaning | Normal Effect |
|---|---|---|
| K_f | Filtration coefficient (permeability × surface area) | ↑ K_f → more filtration |
| P_c | Capillary hydrostatic pressure | ↑ P_c → pushes fluid out |
| P_if | Interstitial fluid hydrostatic pressure | ↑ P_if → opposes filtration |
| π_c | Plasma colloid osmotic pressure (oncotic) | ↑ π_c → draws fluid back in |
| π_if | Interstitial fluid colloid osmotic pressure | ↑ π_if → draws fluid out |
Any of the following increases filtration → edema:
- ↑ capillary hydrostatic pressure
- ↓ plasma colloid osmotic pressure
- ↑ capillary permeability (↑ K_f)
Summary of Causes of Extracellular Edema
I. Increased Capillary Hydrostatic Pressure
A. Excessive renal retention of salt and water
- Acute/chronic kidney failure
- Mineralocorticoid excess
B. High venous pressure
- Heart failure
- Venous obstruction
- Failure of venous pumps (paralysis, immobilization, valve failure)
C. Decreased arteriolar resistance
- Excessive body heat
- Sympathetic insufficiency
- Vasodilator drugs
II. Decreased Plasma Proteins (↓ π_c)
- Nephrotic syndrome — loss of proteins in urine
- Burns/wounds — protein loss from skin
- Liver disease (cirrhosis) — failure to synthesize albumin
- Malnutrition — inadequate protein intake
III. Increased Capillary Permeability (↑ K_f)
- Immune/allergic reactions (histamine release)
- Toxins, bacterial infections
- Vitamin C deficiency
- Prolonged ischemia, burns
IV. Lymphatic Blockage (Lymphedema)
- Cancer, surgery, infections (e.g., filariasis)
- Congenital absence of lymphatics
- Key point: Proteins that leak out cannot be removed → ↑ π_if → more fluid drawn out → worsening cycle
Edema in Heart Failure
| Phase | Mechanism |
|---|---|
| Acute | Aortic pressure ↓, RA pressure ↑ → capillary pressure falls to ~13 mmHg → no immediate peripheral edema (pulmonary edema may occur) |
| Chronic | ↓ renal blood flow → renin ↑ → angiotensin II + aldosterone ↑ → salt & water retention → venous pressure ↑ → capillary pressure ↑ → peripheral edema |
| Advanced | ↑ ADH → water reabsorption → hyponatremia → both intracellular and extracellular edema |
In left-sided failure, raised pulmonary capillary pressure causes pulmonary edema.
In right-sided failure (or combined), raised systemic venous pressure causes peripheral edema.
Lymphedema — Special Consideration
When lymphatics are blocked:
- Proteins accumulate in interstitium
- ↑ π_if draws more fluid from capillaries
- Fluid → protein → more fluid = self-perpetuating cycle
- Tissue becomes chronically swollen and fibrotic (elephantiasis in filariasis)
Safety Factors That Normally Prevent Edema
Three major protective mechanisms act against edema:
1. Low Compliance of the Interstitium (−3 mmHg range)
- Normal interstitial fluid pressure = −3 mmHg (slightly subatmospheric)
- In this negative pressure range, small volume changes cause large pressure increases → opposes further filtration
- Safety factor = ~3 mmHg
- Proteoglycan gel in tissues binds fluid → restricts free fluid movement
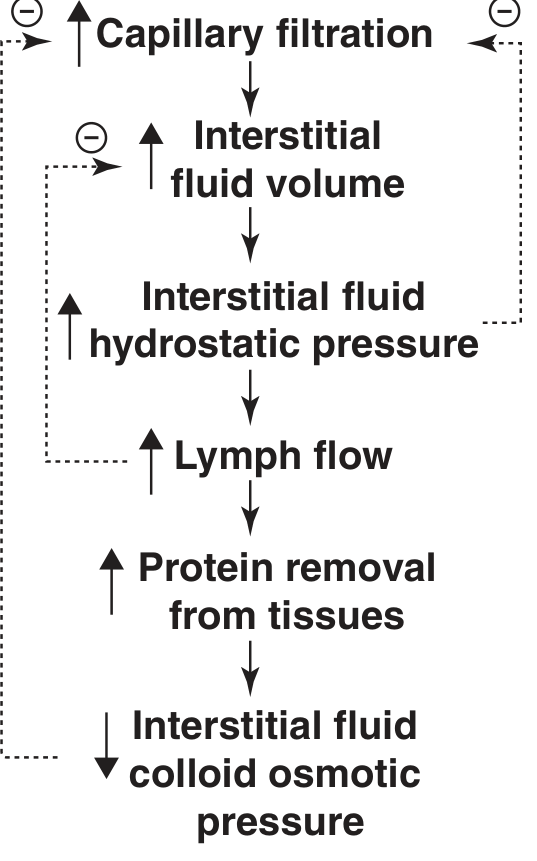
2. Increased Lymph Flow (10–50× normal)
- When capillary filtration increases, lymph flow rises dramatically
- More fluid returned to blood, preventing accumulation
- Safety factor = ~7 mmHg
3. Wash-Down of Interstitial Proteins
- As filtration ↑ → interstitial proteins get diluted
- ↓ π_if → less force drawing fluid out of capillaries
- Safety factor = ~7 mmHg
Total Safety Factor = ~17 mmHg
Capillary pressure would have to approximately double before marked edema occurs.
Edema in Potential Spaces (Effusion)
| Space | Clinical Term |
|---|---|
| Peritoneal cavity | Ascites (up to 20 L in cirrhosis) |
| Pleural cavity | Pleural effusion |
| Pericardial cavity | Pericardial effusion |
| Joint spaces | Synovial effusion |
Effusion occurs when edema forces fluid into these spaces via the same mechanisms (excess capillary filtration or lymphatic blockage). Proteins drain through lymphatics arising directly from cavity surfaces.
Key Clinical Correlations (AHS Exam Points)
| Condition | Primary Mechanism | Type |
|---|---|---|
| Heart failure | ↑ venous/capillary hydrostatic pressure | Pitting edema (legs) |
| Nephrotic syndrome | ↓ plasma proteins (albuminuria) | Generalized/facial |
| Liver cirrhosis | ↓ albumin synthesis + portal hypertension | Ascites + peripheral |
| Malnutrition (Kwashiorkor) | ↓ plasma oncotic pressure | Generalized |
| Filariasis | Lymphatic blockage | Non-pitting (elephantiasis) |
| Inflammation/allergy | ↑ capillary permeability | Local edema |
| Renal failure | Salt & water retention → ↑ hydrostatic pressure | Generalized |
Quick Revision Summary
Edema = ↑ Capillary Filtration OR Lymphatic Failure
↑ Filtration caused by:
→ ↑ Capillary hydrostatic pressure (heart failure, venous obstruction, renal retention)
→ ↓ Plasma oncotic pressure (nephrotic, cirrhosis, malnutrition)
→ ↑ Capillary permeability (inflammation, burns, toxins)
Safety factors (total = 17 mmHg):
→ Low interstitium compliance = 3 mmHg
→ Increased lymph flow = 7 mmHg
→ Protein washdown from interstitium = 7 mmHg
Sources: Guyton and Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology, 26th Ed. Content aligned with Sembulingam's Essentials of Medical Physiology AHS syllabus topics.
This is a shared conversation. Sign in to Orris to start your own chat.