Anterior abdominal wall anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have excellent content and images. Let me compile the comprehensive answer.
Anterior Abdominal Wall Anatomy
Layers (Superficial to Deep)
The anterior abdominal wall has the following layers, encountered in order during surgical incision:
- Skin
- Superficial fascia - two sublayers:
- Camper's fascia - the outer fatty layer (panniculus adiposus), continuous with the dartos of the scrotum; contains the superficial epigastric and superficial circumflex iliac vessels
- Scarpa's fascia - the deeper fibrous/membranous layer; forms the fundiform (suspensory) ligament of the penis; fuses inferiorly with fascia lata of thigh
- Deep (investing) fascia - fascia innominata, covers the external oblique
- Musculoaponeurotic layer (see below - three flat muscles laterally, rectus medially)
- Transversalis fascia - the endoabdominal fascia lining the wall internally
- Extraperitoneal fat (preperitoneal fat)
- Peritoneum
Muscles
Lateral (Flat) Muscles - Three Layers
These three muscles arise posteriorly, their fibers running in different directions, and converge medially into broad aponeuroses that interdigitate at the linea alba.
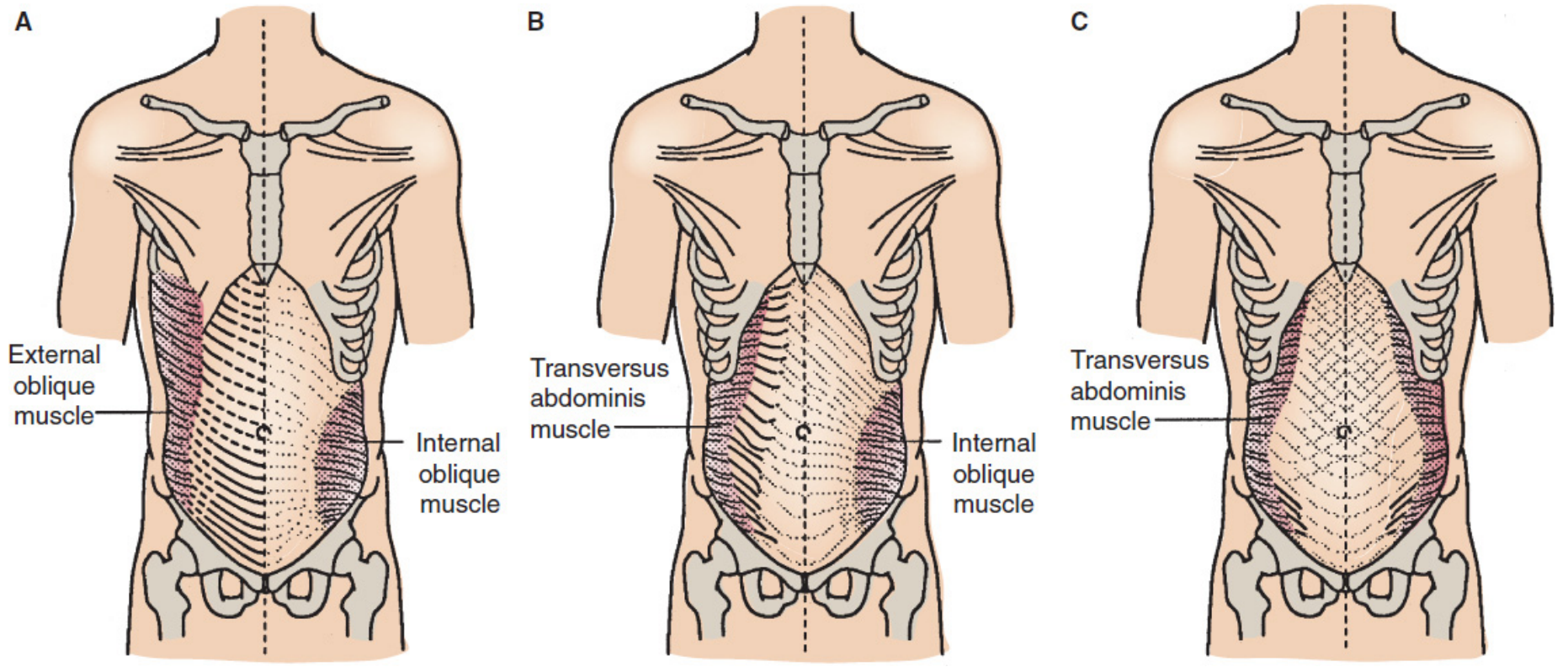
A - External Abdominal Oblique (most superficial)
- Origin: posterior aspects of lower 8 ribs; interdigitates with serratus anterior and latissimus dorsi
- Fibers: run inferomedially ("hands-in-pockets" direction)
- Aponeurosis: forms the anterior rectus sheath; its inferior free edge rolls inward to form the inguinal ligament (ASIS to pubic tubercle)
- The aponeurosis splits at the pubic tubercle to form the superficial (external) inguinal ring
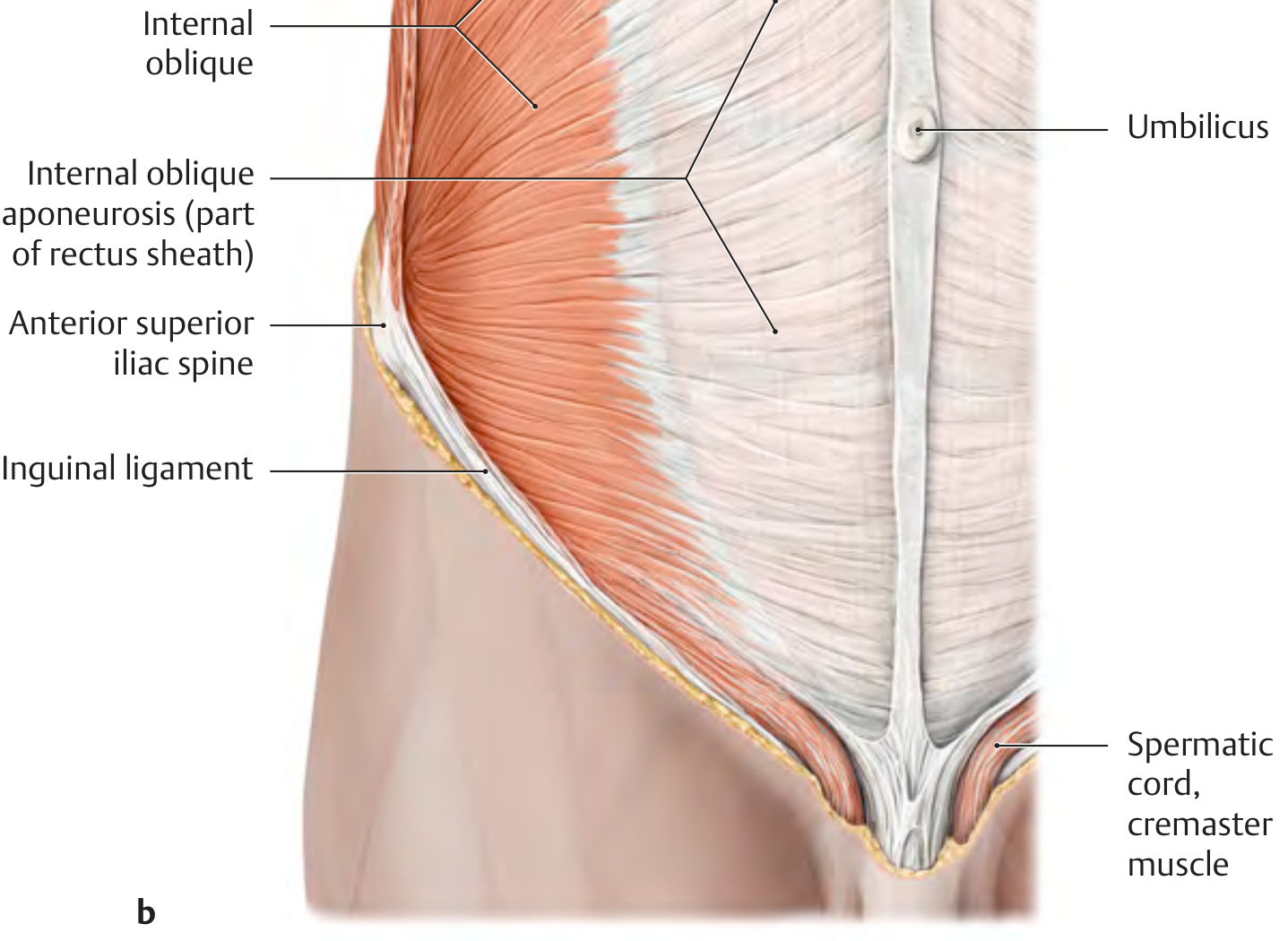
B - Internal Abdominal Oblique (middle layer)
- Origin: thoracolumbar fascia, ASIS, inguinal ligament
- Fibers: run superomedially (perpendicular to external oblique)
- Aponeurosis: splits at the lateral border of rectus to contribute to both anterior and posterior rectus sheath (above arcuate line)
- Its inferior free border arches over the inguinal canal, forming the roof of the canal; continues onto the spermatic cord as the cremaster muscle and cremasteric fascia
C - Transversus Abdominis (deepest flat muscle)
- Origin: lower 6 costal cartilages, thoracolumbar fascia, ASIS, inguinal ligament
- Fibers: run transversely (horizontally)
- Aponeurosis: contributes to posterior rectus sheath above arcuate line; passes entirely anterior below arcuate line
- The lower free border forms the conjoint tendon (falx inguinalis) with internal oblique, inserting onto pubic crest

Vertical (Strap) Muscles - Midline
Rectus Abdominis
- Runs vertically from pubic symphysis and pubic crest to costal cartilages 5-7 and xiphoid process
- Divided by 3 fibrous tendinous intersections (at xiphoid, umbilicus, and halfway between) - these are adherent anteriorly to the rectus sheath but not posteriorly
- Enclosed in the rectus sheath formed by the aponeuroses of the three flat muscles
- Function: flexes trunk, compresses abdomen, depresses ribs
Pyramidalis
- Small triangular muscle at the pubic symphysis, within the rectus sheath
- Tenses the linea alba; absent in ~20% of individuals
Rectus Sheath
The sheath is formed by the decussating aponeuroses of the three flat muscles. Its composition changes at the arcuate line (of Douglas), located at the midpoint between umbilicus and pubis:
| Region | Anterior Sheath | Posterior Sheath |
|---|---|---|
| Above arcuate line | External oblique aponeurosis + anterior lamella of internal oblique | Posterior lamella of internal oblique + transversus aponeurosis |
| Below arcuate line | All three aponeuroses (external oblique + both lamellae of internal oblique + transversus) | Absent - only transversalis fascia + peritoneum |
The semilunar line (of Spieghel) marks the lateral border of the rectus sheath, where the flat muscle aponeuroses begin.
Linea Alba
A tendinous raphe running in the midline from xiphoid to pubic symphysis, formed by the decussation and interdigitation of the aponeurotic fibers of all three flat muscles from both sides. It is wider above the umbilicus (up to 1-2 cm) and narrower below. This is a surgical approach site (midline laparotomy).
Blood Supply
Arterial:
- Superior epigastric artery - terminal branch of the internal thoracic (internal mammary) artery; enters the rectus sheath superiorly
- Inferior epigastric artery - branch of the external iliac artery; enters the rectus sheath inferiorly and anastomoses with the superior epigastric within the muscle
- Together they form the epigastric arcade within the rectus muscle
- Lateral muscles are supplied by the lower 3-4 intercostal arteries, deep circumflex iliac artery, and lumbar arteries
- Superficial fascia is supplied by the superficial epigastric and superficial circumflex iliac arteries (branches of the femoral artery)
Venous: Corresponding veins drain to the internal thoracic (superiorly) and external iliac/femoral veins (inferiorly)
Nerve Supply
The anterior abdominal wall is segmentally innervated in a dermatome pattern:
- T7-T12 (lower intercostal nerves) - innervate skin and muscles in a band from xiphoid to just below umbilicus
- T10 - corresponds to the umbilicus (important clinical landmark)
- L1 - divides into the iliohypogastric and ilioinguinal nerves
- Iliohypogastric nerve: pierces external oblique above superficial inguinal ring, innervates skin above pubis
- Ilioinguinal nerve: passes through inguinal canal and superficial ring, innervates upper medial thigh and scrotum/labia majora
- L1-L2 (genitofemoral nerve): innervates cremaster muscle
- Nerves pass anteriorly in a plane between internal oblique and transversus abdominis, then pierce the lateral rectus sheath
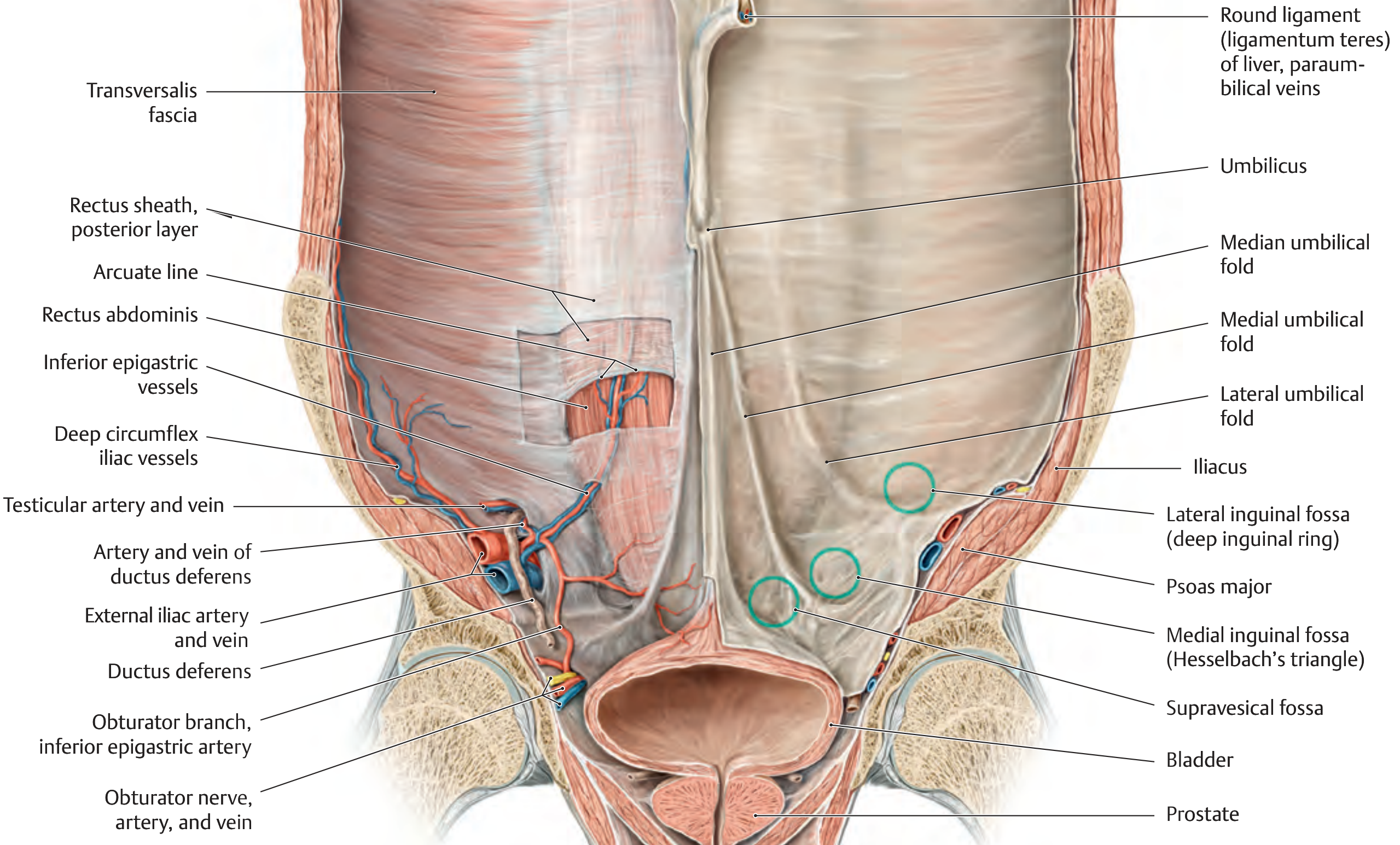
Internal Surface of the Anterior Abdominal Wall
Viewed from inside (as in laparoscopy), the lower abdominal wall shows five peritoneal folds radiating toward the umbilicus:
| Fold | Content | Paired/Unpaired |
|---|---|---|
| Median umbilical fold | Obliterated urachus | Unpaired (midline) |
| Medial umbilical folds (x2) | Obliterated umbilical arteries | Paired |
| Lateral umbilical folds (x2) | Inferior epigastric vessels (active) | Paired |
These folds define three important fossae on each side, which are potential hernia sites:
| Fossa | Location | Hernia |
|---|---|---|
| Supravesical fossa | Between median and medial umbilical folds | Supravesical hernia |
| Medial inguinal fossa (Hesselbach's triangle) | Between medial and lateral umbilical folds | Direct inguinal hernia |
| Lateral inguinal fossa | Lateral to lateral umbilical fold | Indirect inguinal hernia (site of deep inguinal ring) |
Hesselbach's triangle boundaries:
- Medially: lateral border of rectus abdominis
- Laterally: inferior epigastric vessels
- Inferiorly: inguinal ligament
The Inguinal Canal
A 4 cm oblique passage through the lower abdominal wall:
| Feature | Contents |
|---|---|
| Deep (internal) inguinal ring | Lateral inguinal fossa, in transversalis fascia, lateral to inferior epigastric vessels |
| Superficial (external) inguinal ring | Opening in external oblique aponeurosis, superior to pubic tubercle |
| Anterior wall | External oblique aponeurosis (+ internal oblique laterally) |
| Posterior wall | Transversalis fascia (+ conjoint tendon medially) |
| Roof | Arched fibers of internal oblique and transversus |
| Floor | Inguinal ligament (+ lacunar ligament medially) |
| Contents (male) | Spermatic cord: vas deferens, testicular/cremasteric/artery to vas deferens, ilioinguinal nerve, lymphatics |
| Contents (female) | Round ligament of uterus, ilioinguinal nerve |
Clinical Relevance
- Midline laparotomy incises the avascular linea alba - minimal bleeding, no muscle damage
- Pfannenstiel incision transects the anterior rectus sheath transversely, then separates the rectus muscles in the midline - used for pelvic surgery
- Kocher incision (subcostal) is used for cholecystectomy/hepatic surgery
- Inferior epigastric vessel injury during laparoscopy: trocars placed lateral to the lateral umbilical folds risk injuring these vessels
- Arcuate line significance: below this line, the posterior rectus sheath is absent - rectus sheath hematoma extending below the arcuate line is not self-limiting and can spread freely into the extraperitoneal space
- Nerve preservation in flap surgery: the rectus abdominis is supplied by segmental nerves T7-T12 entering laterally; a TRAM flap requires preservation of these neurovascular pedicles
Sources: General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy; Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7th ed.
Deep dive into the inguinal canal anatomy and hernia sites
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive, well-illustrated content from multiple authoritative sources. Here is the full deep-dive:
Inguinal Canal Anatomy and Hernia Sites
Overview
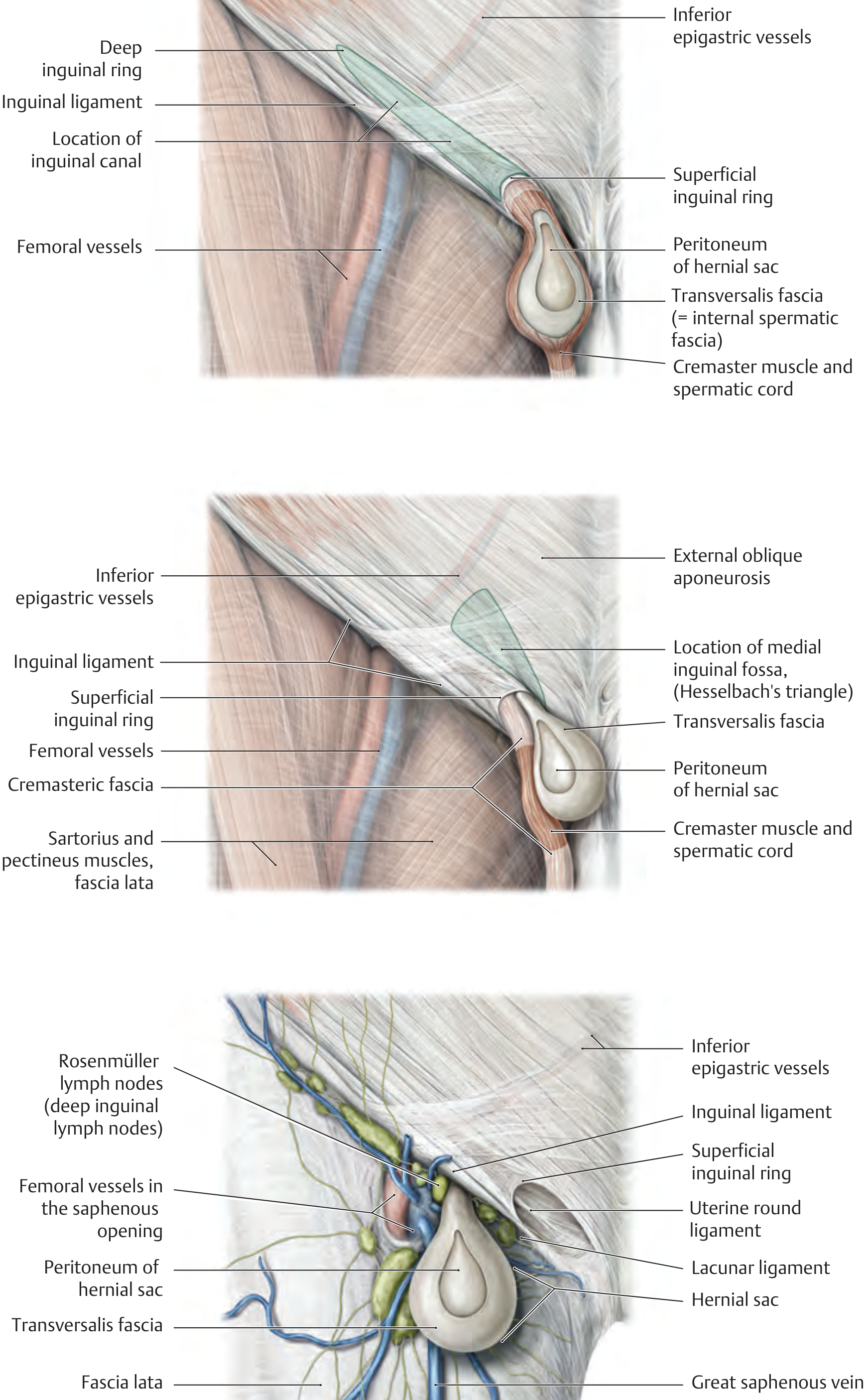
The inguinal canal is an oblique passage through the lower anterior abdominal wall, approximately 4-6 cm long in the adult. It runs parallel to and just above the inguinal ligament, directed obliquely downward, forward, and medially - from the deep inguinal ring to the superficial inguinal ring. It was created embryologically by the descent of the testis (or round ligament in females), and it remains patent for life, forming a permanent potential path for herniation.
The Two Openings
Deep (Internal) Inguinal Ring
- A U-shaped defect in the transversalis fascia, located in the lateral inguinal fossa
- Position: midpoint of the inguinal ligament, approximately 2-3 cm above and lateral to the femoral artery pulse
- The inferior epigastric vessels lie just medial to this ring - this is the key anatomical landmark distinguishing indirect from direct hernias
- Bounded by: the interfoveolar ligament (medially), inguinal ligament (inferiorly), and the lateral umbilical fold
- The transversalis fascia is evaginated through this ring as the internal spermatic fascia around the spermatic cord
Superficial (External) Inguinal Ring
- A triangular/inverted-V defect in the external oblique aponeurosis, just lateral and superior to the pubic tubercle
- Bounded by: the medial crus (superomedially), lateral crus (inferolaterally), intercrural fibers (superolaterally), and the reflected (reflex) inguinal ligament (inferiorly)
- Transmits: the spermatic cord in males, the round ligament in females, and the ilioinguinal nerve in both
Walls of the Inguinal Canal
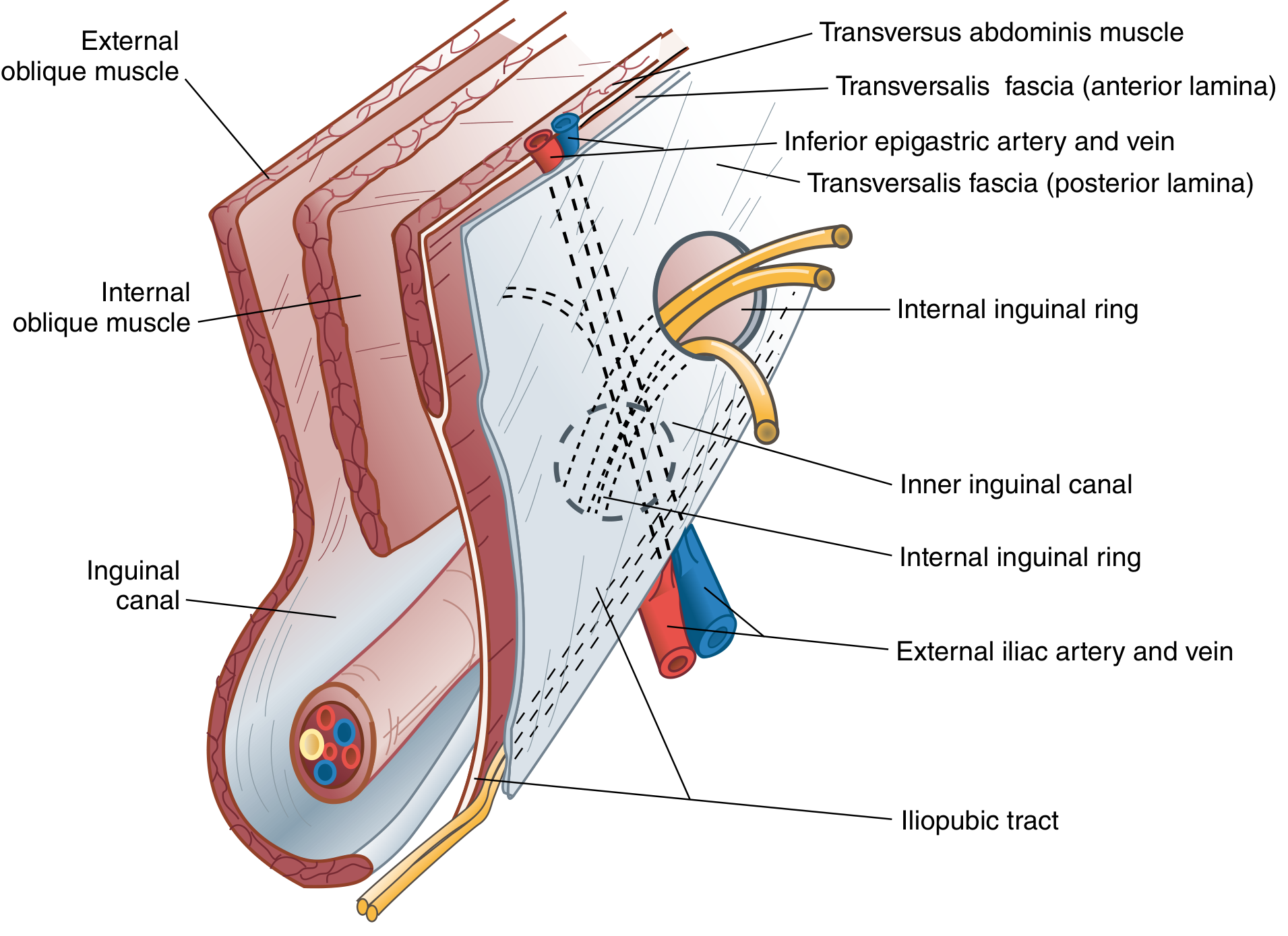
| Wall | Structure(s) |
|---|---|
| Anterior wall | External oblique aponeurosis (full length) + internal oblique muscle (lateral third only) |
| Posterior wall | Transversalis fascia (full length) + conjoint tendon medially |
| Roof (superior) | Arched fibers of internal oblique and transversus abdominis (they arch over the canal and descend to form the conjoint tendon) |
| Floor (inferior) | Inguinal ligament (rolled-inward lower edge of external oblique aponeurosis) + lacunar ligament medially |
Key point: the posterior wall is weakest medially - between the conjoint tendon laterally and the rectus sheath. This is Hesselbach's triangle, the site of direct hernias.
Contents of the Inguinal Canal
In males - the spermatic cord:
- Vas deferens (ductus deferens)
- Testicular artery (from aorta)
- Pampiniform venous plexus (drains to testicular vein)
- Artery to the vas deferens (from inferior vesical artery)
- Cremasteric artery (from inferior epigastric artery)
- Lymphatics
- Autonomic nerves
- Processus vaginalis remnant
- Three fascial coverings: internal spermatic fascia (from transversalis fascia), cremasteric fascia + cremaster muscle (from internal oblique), external spermatic fascia (from external oblique)
In females:
- Round ligament of the uterus (ends in labia majora)
- Artery to the round ligament
In both sexes:
- Ilioinguinal nerve (L1) - runs anterior to the cord inside the canal, exits superficial ring to supply medial thigh, root of penis/labia majora, upper scrotum
- Lymphatics
Related Ligaments
| Ligament | Description | Relevance |
|---|---|---|
| Inguinal ligament (Poupart's) | Infolded lower border of external oblique aponeurosis; ASIS to pubic tubercle | Floor of canal; superior border of femoral triangle |
| Lacunar ligament (Gimbernat's) | Medial extension of inguinal ligament folding horizontally onto pectineal line | Medial border of femoral ring; cuts in to release strangulated femoral hernia |
| Pectineal ligament (Cooper's) | Periosteum of superior pubic ramus from pubic tubercle to iliopectineal eminence | Used in hernia repair (McVay repair); posterior border of femoral ring |
| Iliopubic tract | Thickened band of transversalis fascia running parallel to inguinal ligament | Deep to inguinal ligament; important landmark in laparoscopic hernia repair |
| Conjoint tendon (falx inguinalis) | Fused aponeuroses of internal oblique and transversus abdominis, inserting on pubic crest | Forms medial part of posterior wall; reinforces Hesselbach's triangle |
| Interfoveolar ligament (Hesselbach's ligament) | Thickened transversalis fascia medial to deep ring | Medial boundary of deep inguinal ring |
Hesselbach's Triangle
The key weak zone of the posterior wall, bounded by:
- Laterally: inferior epigastric vessels (lateral umbilical fold)
- Medially: lateral border of rectus abdominis (semilunar line)
- Inferiorly: inguinal ligament (iliopubic tract/pectineal ligament)
At this site, the abdominal wall consists of only transversalis fascia + external oblique aponeurosis - no muscle protection. This is where direct inguinal hernias bulge through.
The Myopectineal Orifice (Fruchaud's Orifice)
Described by the French surgeon Henri René Fruchaud in 1956, this is a single large musculoaponeurotic gap in the lower abdominal wall through which all groin hernias (inguinal and femoral) pass. The inguinal ligament divides it into:
- Superior (inguinal) portion - site of direct and indirect inguinal hernias
- Inferior (femoral) portion - site of femoral hernias
Modern laparoscopic hernia repair (TAPP/TEP) is designed to cover this entire orifice with a wide mesh, addressing all three hernia types in one repair.
Groin Hernia Sites

1. Indirect (Lateral) Inguinal Hernia
- Internal opening: deep inguinal ring - lateral to the inferior epigastric vessels
- Course: passes obliquely through the entire inguinal canal, anterolateral to the spermatic cord
- External opening: superficial inguinal ring
- Can descend into the scrotum (scrotal hernia) - follows the path of the processus vaginalis
- Congenital type: due to a patent processus vaginalis (always the cause in infants and children)
- Acquired type: gradual widening of the deep ring from raised intra-abdominal pressure
- Coverings (medial to lateral): peritoneum, extraperitoneal fat, internal spermatic fascia, cremasteric fascia, external spermatic fascia
- Strangulation risk: high - the narrow deep ring can constrict the neck of the sac
2. Direct (Medial) Inguinal Hernia
- Internal opening: medial inguinal fossa (Hesselbach's triangle) - medial to the inferior epigastric vessels
- Course: protrudes directly and perpendicularly through the posterior wall; does NOT traverse the full inguinal canal
- External opening: superficial inguinal ring (the sac appears medial to the spermatic cord)
- Always acquired - due to weakness/attenuation of the transversalis fascia and conjoint tendon
- More common in elderly males with chronic raised intra-abdominal pressure
- Broad-necked - strangulation is rare; the bladder may be pulled into the sac (sliding component)
- Does not descend into the scrotum (no processus vaginalis involvement)
Key clinical test: reduce the hernia, place a finger over the deep ring (midpoint of inguinal ligament), ask patient to cough:
- Hernia controlled → indirect (exits lateral to finger)
- Hernia not controlled, bulges medially → direct
3. Femoral Hernia
- Internal opening: femoral ring - below the inguinal ligament, medial to the femoral vein
- Course: passes through the femoral canal (within the femoral sheath) downward toward the thigh
- External opening: saphenous opening (hiatus in fascia lata), approximately 2 cm below the inguinal ligament
- Always acquired
- More common in women (wider pelvis, larger femoral ring)
- Femoral ring boundaries: inguinal ligament (anteriorly), lacunar ligament (medially), femoral vein (laterally), pectineal ligament/Cooper's ligament (posteriorly)
- High strangulation risk: the lacunar ligament forms a sharp, rigid medial border that constricts the neck of the sac - emergency surgery is often required
- The sac initially points downward, then turns forward and superiorly (due to fascia lata resistance), which is why the swelling appears below and lateral to the pubic tubercle (vs. inguinal hernias which appear above and medial to the pubic tubercle)
Laparoscopic View of the Inguinal Region
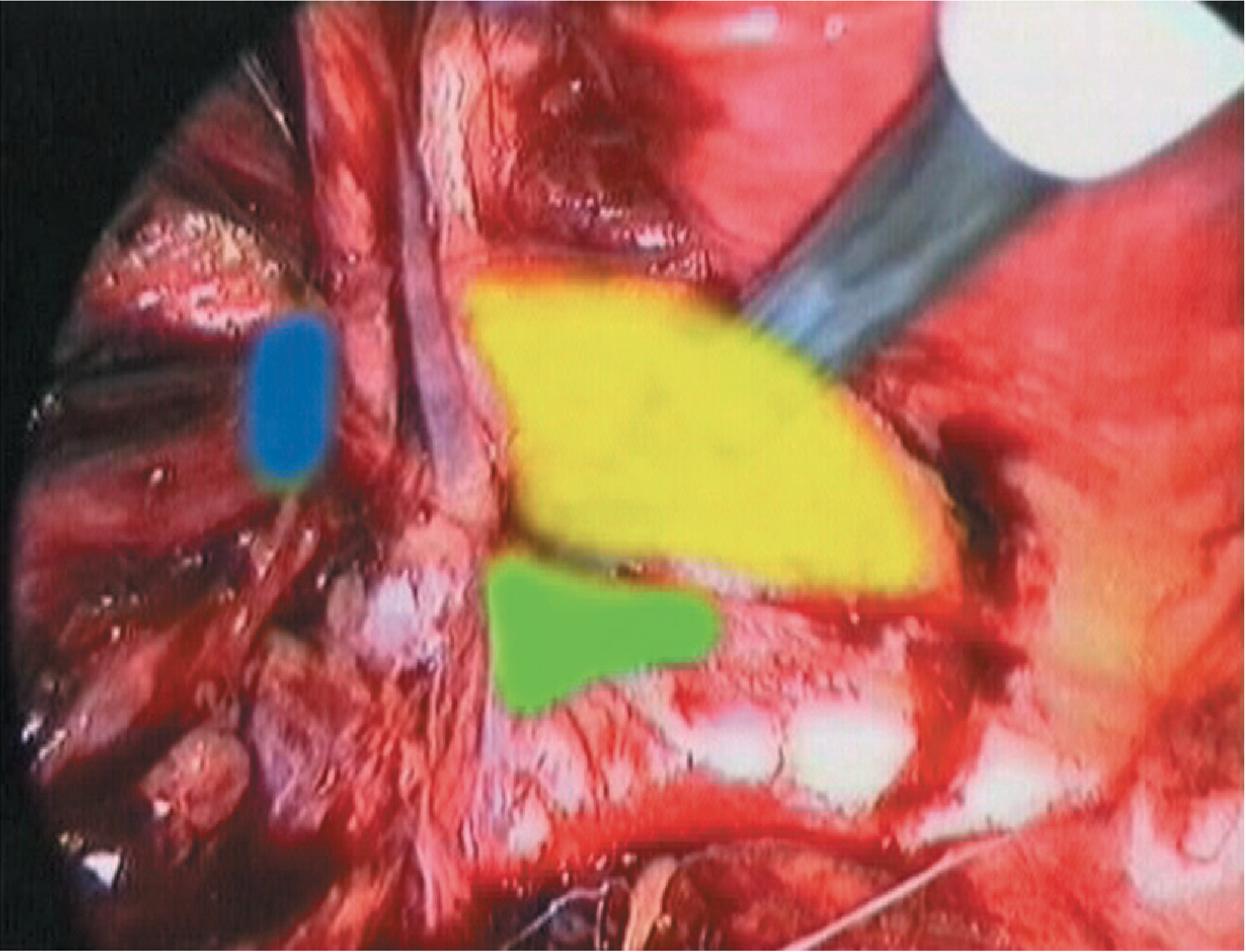
From the laparoscopic perspective (looking at the posterior surface of the anterior abdominal wall):
- Yellow area = Hesselbach's triangle (direct hernia site)
- Blue area = lateral inguinal fossa, site of deep inguinal ring (indirect hernia site)
- Green area = femoral ring (femoral hernia site)
Comparative Summary Table
| Feature | Indirect Inguinal | Direct Inguinal | Femoral |
|---|---|---|---|
| Relation to inf. epigastric vessels | Lateral | Medial | Below inguinal ligament |
| Relation to pubic tubercle | Above and medial | Above and medial | Below and lateral |
| Neck of sac | Narrow (deep ring) | Wide (Hesselbach's) | Very narrow (femoral ring) |
| Strangulation risk | High | Low | Very high |
| Aetiology | Congenital or acquired | Always acquired | Always acquired |
| Descends to scrotum? | Yes | No | No (thigh) |
| Common sex | Male >> Female | Male | Female > Male |
| Coverings | 3 layers of spermatic cord | Pushes through transversalis only | Femoral sheath + fascia lata |
| Age | Any age | Older adults | Middle-aged / older women |
Special Hernia Types
Pantaloon (Saddle) Hernia: both a direct and indirect hernia coexist on the same side, straddling the inferior epigastric vessels like trouser legs.
Sliding Hernia: a retroperitoneal viscus (usually sigmoid colon on the left, caecum/bladder on the right) forms part of the wall of the hernia sac. The sac forms secondarily. Caution: bowel can be damaged during sac dissection.
Littre's Hernia: a Meckel's diverticulum is the sole content of the sac.
Amyand's Hernia: the appendix is within the hernia sac (most often inguinal).
Maydl's Hernia ("hernia-in-W"): two loops of bowel are within the sac, with the connecting loop (which can strangulate) still inside the abdomen.
Nerve Injury Risk in Hernia Repair
| Nerve | Course | Injury consequence |
|---|---|---|
| Ilioinguinal (L1) | Runs anterior to cord in canal; exits superficial ring | Loss of sensation: medial thigh, scrotum/labia |
| Iliohypogastric (L1) | Pierces external oblique above superficial ring | Loss of sensation: suprapubic skin |
| Genitofemoral - genital branch (L1/2) | Enters canal at deep ring with cremaster vessels | Loss of cremasteric reflex; scrotal/labial numbness |
| Femoral nerve (L2-L4) | Deep to inguinal ligament, lateral to femoral artery | Rare in open repair; risk in laparoscopic stapling below iliopubic tract |
| Lateral femoral cutaneous nerve (L2-L3) | Crosses iliac fossa under inguinal ligament near ASIS | Meralgia paraesthetica (lateral thigh numbness) |
The "triangle of doom" (in laparoscopy) is the space between the vas deferens medially and testicular vessels laterally - it contains the external iliac vessels and must never be stapled.
Sources: Bailey and Love's Short Practice of Surgery, 28th ed.; General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy; Sabiston Textbook of Surgery, current ed.; Mulholland and Greenfield's Surgery, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.