Explain me 10 common heart disease with ecg changes and ecg images of those disease
Reading File
Finding Sources
Finding Sources
Searching the Web
10 common heart diseases ECG changes with ECG images explained
Reading File
Reading File
Searching the Web
ECG images atrial fibrillation ventricular fibrillation heart block LBBB site:litfl.com OR site:ecgwaves.com
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG strips STEMI atrial fibrillation heart block hypertrophy Brugada WPW site:ecgwaves.com OR site:litfl.com
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
Finding Sources
Searching the Web
pericarditis ECG saddle shaped ST elevation complete heart block third degree AV block ECG images
Loading Image
Loading Image
Loading Image
I now have all the textbook images retrieved successfully. Let me compose the comprehensive answer using everything gathered.
10 Common Heart Diseases: ECG Changes and Images
Below is a clinical guide to the 10 most common cardiac conditions, each with their characteristic ECG findings and images sourced from authoritative medical textbooks (Harrison's, Ganong's, Guyton & Hall, Braunwald's).
1. ST-Elevation Myocardial Infarction (STEMI)
What it is: Complete occlusion of a coronary artery leading to transmural (full-thickness) myocardial necrosis.
ECG Changes:
- Hyperacute T waves - tall, peaked T waves (first minutes)
- ST-segment elevation - convex (tombstone) shape in leads overlying the infarct zone (≥1 mm in limb leads, ≥2 mm in precordial leads)
- Reciprocal ST depression in leads opposite the infarct
- Pathological Q waves - develop over hours to days (>40 ms wide and/or >25% of R-wave height), indicating necrosis
- T-wave inversion - follows the ST elevation as the infarct evolves
- Loss of R-wave progression ("failure of R wave progression") in anterior STEMI
Localization by leads:
| Territory | Artery | Leads |
|---|---|---|
| Anterior | LAD | V1-V4 |
| Inferior | RCA | II, III, aVF |
| Lateral | LCx | I, aVL, V5-V6 |
| Posterior | RCA/LCx | Tall R in V1-V2 (reciprocal) |
Mechanism: Three ECG defects in infarcted cells: abnormally rapid repolarization (K⁺ channels open) → ST elevation; decreased resting membrane potential from K⁺ loss → TQ depression (manifests as ST elevation); delayed depolarization → ST elevation. As the Harrison's textbook explains, with subendocardial ischemia the ST vector points inward (ST depression in overlying leads); with epicardial/transmural injury the ST vector points outward (ST elevation in overlying leads).


2. NSTEMI / Unstable Angina (Non-ST-Elevation ACS)
What it is: Partial occlusion of a coronary artery causing subendocardial ischemia without transmural necrosis (NSTEMI) or reversible ischemia (unstable angina). Troponin elevation distinguishes NSTEMI from unstable angina.
ECG Changes:
- ST depression (horizontal or downsloping, ≥0.5-1 mm) in leads overlying ischemic zone
- T-wave flattening or inversion - particularly prominent (deep symmetric T inversions in V1-V4 = Wellens sign, suggesting high-grade LAD stenosis)
- No ST elevation (by definition)
- ECG may be entirely normal in up to 30% of NSTEMI cases - serial ECGs and troponins are required
- Transient ST elevation may occur with Prinzmetal (vasospastic) angina, resolving completely
Key distinction from STEMI: No persistent ST elevation and no Q-wave formation. Per Harrison's: "The diagnosis of NSTEMI depends on abnormal elevation of cardiac biomarkers but may include ECG changes not meeting criteria for STEMI."
3. Atrial Fibrillation (AF)
What it is: Chaotic, disorganized atrial electrical activity with multiple simultaneous re-entrant wavelets - the most common sustained cardiac arrhythmia. Common causes include mitral valve disease, hypertension, heart failure, and hyperthyroidism.
ECG Changes:
- Absent P waves - replaced by irregular fibrillatory (f) waves, fine undulations at 350-600/min
- Irregularly irregular RR intervals (the hallmark - no two RR intervals are the same)
- Variable ventricular rate - typically 100-160 bpm if uncontrolled
- Normal QRS morphology (unless aberrant conduction or bundle branch block is present)
- The fibrillatory waves may be coarse (recent onset) or fine (longstanding AF)
Mechanism (Guyton & Hall): Numerous depolarization waves spread in all directions through the atria simultaneously; because they are opposite in polarity at any given time they electrically neutralize each other, producing no discernible P wave. AV node acts as a gatekeeper, passing impulses irregularly at rate ≥0.35 s apart.

Clinical risk: Blood stasis in left atrial appendage → thrombus formation → embolic stroke. Anticoagulation (warfarin or DOACs) is the primary stroke-prevention strategy.
4. Left Bundle Branch Block (LBBB)
What it is: Conduction delay or block in the left bundle branch, forcing ventricular activation to spread from right to left in an abnormal, slow fashion. It is a marker of significant heart disease: coronary artery disease, hypertensive heart disease, aortic valve disease, or cardiomyopathy.
ECG Changes (complete LBBB, QRS ≥120 ms):
- Broad, notched or slurred R wave in lateral leads (I, aVL, V5-V6) - often "M-shaped" or plateau-topped
- Wide, deep QS complex in V1 (no r wave, or very small r)
- Absence of normal septal Q waves in I, V5-V6 (septal depolarization reversed, now R→L)
- Discordant ST-T changes - ST depression and T inversion in leads with dominant R; ST elevation and upright T in V1-V3
- Left axis deviation common
- New LBBB in the setting of chest pain is treated as STEMI equivalent (Sgarbossa criteria apply)
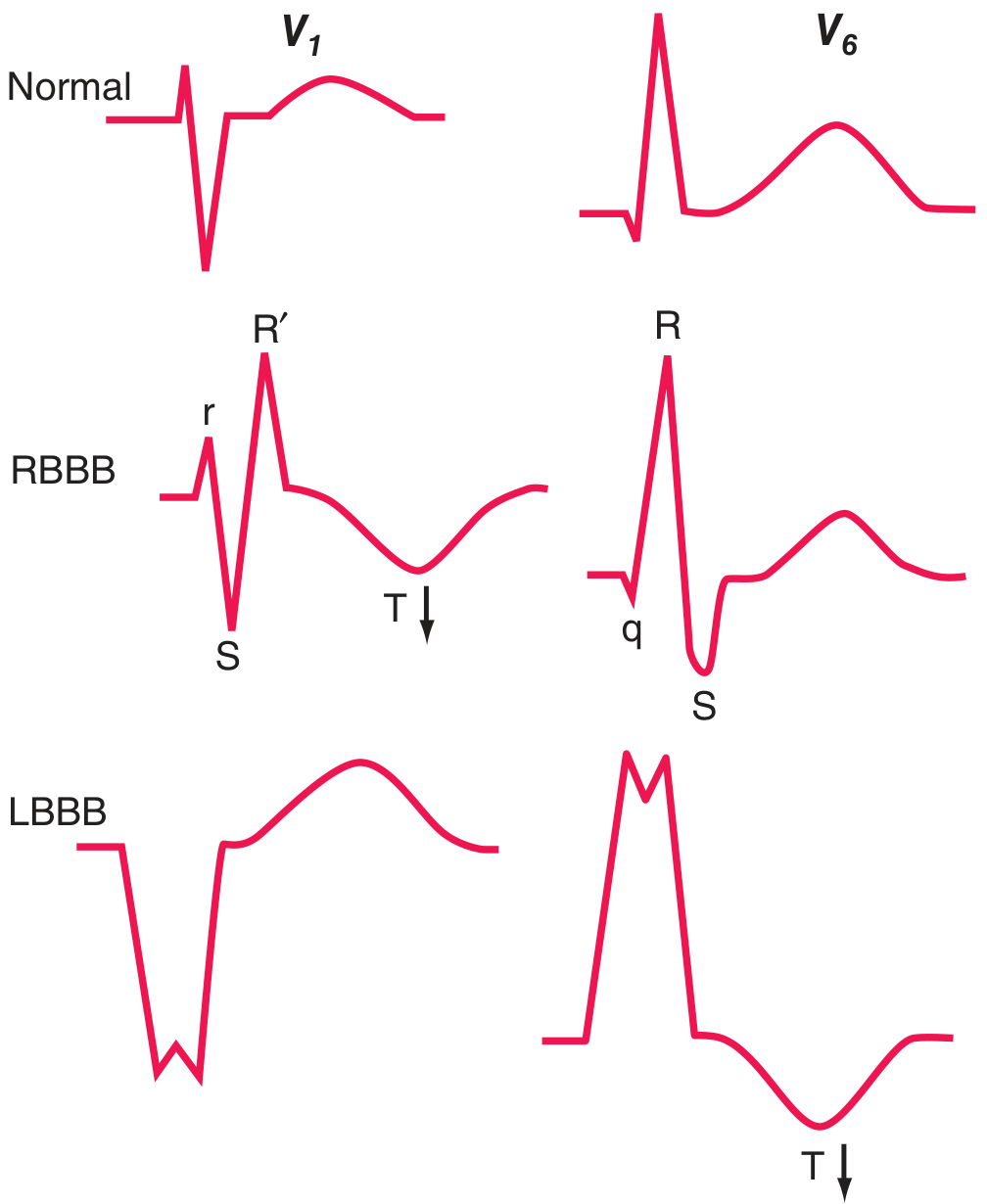
Right Bundle Branch Block (RBBB):
- rSR' (RSR') pattern in V1 ("rabbit ears")
- Wide S wave in I, V5-V6
- T-wave inversion in V1-V2 (secondary repolarization change)
- More commonly a benign finding than LBBB; also seen with atrial septal defect and pulmonary embolism
5. Left Ventricular Hypertrophy (LVH)
What it is: Thickening of the left ventricular wall, typically from chronic pressure overload (hypertension, aortic stenosis) or volume overload (aortic/mitral regurgitation).
ECG Changes:
- High-voltage QRS complexes - the most characteristic finding:
- SV1 + RV5 or RV6 > 35 mm (Sokolow-Lyon criterion)
- R in aVL > 20 mm (women) or > 28 mm (men)
- Left axis deviation (-30° to -90°)
- ST depression and T-wave inversion in lateral leads (I, aVL, V4-V6) - "strain pattern"
- Left atrial enlargement - broad, notched P wave (P mitrale) in II; biphasic P in V1
- LVH may progress to LBBB
Right Ventricular Hypertrophy (RVH):
- Tall R wave in V1 (R > S in V1)
- Right axis deviation (>+90°)
- ST depression and T-wave inversion in right precordial leads (V1-V3)
- Dominant S waves in V5-V6

6. Complete (Third-Degree) AV Block
What it is: No electrical impulses are conducted from the atria to the ventricles. Atria and ventricles beat completely independently. The ventricles are sustained by a slow escape rhythm from below the block.
ECG Changes:
- P waves and QRS complexes are completely dissociated - Ps and QRSs march through independently at different rates (AV dissociation)
- Regular P-P intervals (sinus rate, typically 60-100/min)
- Regular but slow RR intervals from the escape pacemaker (junctional escape: 40-60/min with narrow QRS; ventricular escape: 20-40/min with wide QRS)
- More P waves than QRS complexes
- No fixed relationship between P waves and QRS complexes
Causes: Acute inferior MI (usually transient, from AV nodal ischemia via RCA), Lyme disease, hyperkalemia, digoxin toxicity, congenital heart block, infiltrative disease (sarcoidosis, amyloidosis).
Clinical significance: Often requires temporary or permanent pacemaker implantation.
7. Pericarditis (Acute)
What it is: Inflammation of the pericardium, typically from viral infection (Coxsackievirus, echovirus), autoimmune disease, or post-MI (Dressler syndrome). Causes diffuse myocardial surface irritation.
ECG Changes (diffuse, involving multiple lead groups - unlike focal STEMI):
- Diffuse concave ("saddle-shaped") ST elevation in most leads (I, II, III, aVF, V2-V6) - the ST is scooped upward, not convex
- PR segment depression in leads II, V4-V6 (highly specific, from atrial inflammation)
- PR elevation in aVR (reciprocal to PR depression elsewhere)
- No reciprocal ST depression (except in aVR and V1)
- No pathological Q waves (distinguishes from STEMI)
- T-wave inversion develops after ST elevation normalizes (stage III)
- Four classic stages: Stage I (ST elevation + PR depression) → Stage II (ST normalizes) → Stage III (T inversion) → Stage IV (normalization)
Key distinction from STEMI: Saddle-shaped (concave up) vs. convex ST elevation; diffuse multi-lead distribution; PR depression; no Q waves; no reciprocal changes except in aVR.
8. Hypertrophic Cardiomyopathy (HCM)
What it is: Genetic (autosomal dominant, most commonly myosin heavy chain mutations) disorder causing asymmetric ventricular hypertrophy, particularly of the interventricular septum. A leading cause of sudden cardiac death in young athletes.
ECG Changes:
- LVH voltage criteria - often extreme
- Deeply inverted T waves in lateral leads (V4-V6, I, aVL) - among the deepest T inversions seen in any condition
- Abnormal Q waves in inferior and lateral leads (from septal hypertrophy causing abnormal septal depolarization vectors) - can mimic infarction
- Left axis deviation
- Left atrial enlargement
- Short PR interval may be present
- In apical HCM (Yamaguchi variant): giant T-wave inversions (>10 mm) in V4-V6
9. Wolff-Parkinson-White (WPW) Syndrome
What it is: An accessory conduction pathway (Bundle of Kent) connects the atria and ventricles, bypassing the AV node. This allows ventricular pre-excitation - part of the ventricle depolarizes early via the accessory pathway before normal AV node conduction arrives.
ECG Changes (classic triad):
- Short PR interval (<120 ms) - accessory pathway conducts without AV nodal delay
- Delta wave - initial slurring/notching at the onset of the QRS from early ventricular activation via the accessory pathway
- Wide QRS complex (>120 ms) - from the fusion of pre-excitation and normal conduction
- Secondary ST-T changes - discordant T waves (opposite to delta/QRS direction)
- Pseudo-infarction pattern - delta waves in inferior leads can mimic Q waves
Clinical risk: If AF develops in WPW, impulses can travel to the ventricles at extremely rapid rates via the accessory pathway (bypassing AV nodal protection) → pre-excited AF → ventricular fibrillation → sudden death. AV nodal blocking drugs (verapamil, adenosine, digoxin) are contraindicated in WPW with AF.
10. Brugada Syndrome
What it is: A genetic ion channelopathy (most commonly SCN5A mutation, affecting cardiac Na⁺ channels) causing characteristic ECG changes and risk of ventricular fibrillation and sudden cardiac death, typically in young males, at rest or during sleep.
ECG Changes:
- Type 1 (diagnostic - "coved" pattern): ST elevation ≥2 mm with a coved (downward convex) shape followed by a negative T wave in ≥1 right precordial lead (V1 or V2)
- Type 2 ("saddle-back" pattern): ST elevation ≥2 mm with a saddle-back shape and positive/biphasic T wave - considered suspicious but not diagnostic alone
- Changes are most pronounced in V1-V2 (right precordial leads)
- Pattern may be intermittent or unmasked by fever, drugs (Na⁺ channel blockers, cocaine), vagal stimulation
- No structural heart disease is present (ECG is the only abnormality at rest)
Key distinction from STEMI/pericarditis: Restricted to right precordial leads V1-V2; characteristic coved morphology; no reciprocal changes; history of syncope or family history of sudden death.
Quick-Reference Summary Table
| # | Condition | Key ECG Feature | Leads Affected |
|---|---|---|---|
| 1 | STEMI | Convex ST elevation + Q waves | Territory-specific |
| 2 | NSTEMI/UA | ST depression, T inversion | Ischemic zone leads |
| 3 | Atrial Fibrillation | No P waves, irregularly irregular | All leads |
| 4 | LBBB | QS in V1, broad R in V6 (QRS ≥120 ms) | V1, V5-V6, I, aVL |
| 5 | LVH | High voltage + strain pattern | V1, V5-V6, aVL |
| 6 | Complete AV Block | P-QRS dissociation, slow escape | All leads |
| 7 | Pericarditis | Diffuse concave ST↑ + PR depression | Widespread, all except aVR |
| 8 | HCM | Deep T inversions + septal Q waves | V4-V6, inferior leads |
| 9 | WPW | Short PR + delta wave + wide QRS | All leads (V1-V6) |
| 10 | Brugada Syndrome | Coved ST elevation V1-V2 | V1-V2 only |
Sources:
- Guyton and Hall Textbook of Medical Physiology - Atrial fibrillation, conduction system
- Harrison's Principles of Internal Medicine 22E - Ischemia/infarction ECG, bundle branch blocks, hypertrophy
- Ganong's Review of Medical Physiology 26E - ECG mechanisms in MI, ionic changes
- Braunwald's Heart Disease - Brugada syndrome
- Fuster and Hurst's The Heart, 15th Edition - WPW, Brugada patterns
- GOLDMAN-CECIL Medicine - Intraventricular blocks, complete heart block
This is a shared conversation. Sign in to Orris to start your own chat.