Pain full lipoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
painful lipoma treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Here is a thorough, textbook-backed overview of painful lipoma:
Painful Lipoma
What Is a Lipoma?
A lipoma is the most common benign mesenchymal neoplasm in adults. It is a well-encapsulated, slow-growing nodule of mature fat cells (adipocytes) with absent mitotic activity. Most lipomas are painless, soft, mobile, and doughy in consistency. However, pain can and does occur in specific circumstances. - Fitzpatrick's Dermatology, p. 2202
Why Does a Lipoma Become Painful?
There are several distinct reasons:
1. Neurolipoma (Nerve Tissue Within the Lipoma)
When a lipoma contains nerve tissue, it becomes painful and is specifically called a neurolipoma. This is the most direct cause of pain in a solitary lipoma. - S. Das Manual on Clinical Surgery, p. 53
2. Angiolipoma
A lipoma with a prominent vascular pattern (increased blood vessels with fibrin thrombi) is called an angiolipoma. These frequently present as painful, multiple lesions, usually on the upper limbs of young adults. They are sometimes described as the most common type of painful lipoma. - Fitzpatrick's Dermatology, p. 2203; Campbell's Operative Orthopaedics 15th Ed
3. Nerve Compression (Location-Related Pain)
Pain can result from the lipoma pressing on adjacent nerves or neurovascular structures, especially in restricted anatomical spaces such as:
- Carpal tunnel
- Tarsal tunnel
- Cubital tunnel
"Painful findings suggest close approximation to a neurovascular structure or, less commonly, a malignant lesion such as liposarcoma." - Schwartz's Principles of Surgery, p. 1982
4. Dercum's Disease (Adiposis Dolorosa)
A rare but important condition where multiple painful fatty infiltrations occur, predominantly affecting the trunk of obese women. The mechanism of pain is poorly understood. Also known as adiposis dolorosa. - S. Das Manual on Clinical Surgery, p. 54; Campbell's Operative Orthopaedics 15th Ed
5. Multiple Lipomatosis (Neurolipomatosis)
Multiple lipomas can contain nerve tissue and become painful as a group - called neurolipomatosis. Mostly seen in the limbs and trunk. - S. Das Manual on Clinical Surgery, p. 54
6. Inflammation or Trauma
Lipomas can develop post-traumatic changes with fat necrosis and inflammation, leading to tenderness. - Fitzpatrick's Dermatology, p. 2203
Key Clinical Points
| Feature | Detail |
|---|---|
| Typical lipoma | Painless, soft, mobile, doughy, skin freely pinchable |
| Pain suggests | Neurolipoma, angiolipoma, nerve compression, or malignancy |
| Red flag: pain + firmness | Rule out liposarcoma (arises de novo, not from lipoma) |
| Skin dimpling | Fibrous strands connect capsule to skin - dimples on skin movement |
| Deep lipomas | Can be large; MRI recommended to assess proximity to critical structures |
Investigations
- Clinical exam alone is usually sufficient for superficial lipomas
- MRI is the investigation of choice for deep lipomas - shows signal identical to subcutaneous fat on all sequences. Recommended when painful or in close proximity to neurovascular structures. If MRI findings are atypical, incisional biopsy is warranted. - Schwartz's Principles of Surgery
- X-ray is usually normal
Complications of Lipoma (if long-standing)
- Myxomatous degeneration
- Saponification
- Calcification
- Infection
- Ulceration (repeated trauma)
- Malignant change - liposarcoma (rare; most authorities believe liposarcoma arises de novo, not from lipoma) - S. Das, p. 53
Treatment of Painful Lipoma
1. Steroid Injection
- Suitable for painful lipomas < 2.5 cm where pathologic examination is likely unnecessary
- Triamcinolone diluted with 1% lidocaine to 10 mg/mL (1-3 mL) injected into the center monthly
- Shrinks the lipoma but rarely eliminates it entirely; recurrences are frequent
- Textbook of Family Medicine 9e, p. 760
2. Liposuction
- Can be performed under local anesthesia with cannula or 16-gauge syringe
- Does not guarantee complete removal
3. Surgical Excision (definitive treatment)
- Recommended for symptomatic, painful, enlarging lipomas, or those causing dysfunction
- Small lipomas: enucleated through a small incision with blunt dissection
- Large lipomas: linear or elliptic incision with blunt/sharp dissection
- Compression dressing for 1-2 days post-op; sutures removed in 5-10 days
- Recurrence after marginal excision is rare (except intramuscular lipoma, which has a higher recurrence rate)
- All specimens should be sent for pathological examination
- Textbook of Family Medicine 9e, p. 760; Schwartz's Principles of Surgery
Summary: Types of Painful Lipoma at a Glance
| Type | Cause of Pain | Notes |
|---|---|---|
| Neurolipoma | Contains nerve tissue | Solitary, painful |
| Angiolipoma | Vascular, fibrin thrombi | Multiple, young adults, upper limbs |
| Neurolipomatosis | Multiple lipomas with nerve tissue | Limbs + trunk |
| Dercum's disease | Unknown mechanism | Obese women, trunk, multiple |
| Compressive lipoma | Nerve/vessel compression | Carpal/tarsal/cubital tunnel |
| Intramuscular lipoma | Infiltrative, may compress muscle | Higher recurrence after excision |
Recent evidence note: A 2026 systematic review (PMID 41604515) on Dercum's disease (painful adipose tissue disorder) has been published in Annals of Plastic Surgery - if managing a patient with multiple painful fatty lesions, consulting that review for updated intervention strategies is worthwhile.
Hernia examination
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, structured guide to Hernia Examination drawn from Bailey & Love's Surgery, S. Das Manual on Clinical Surgery, and Schwartz's Principles of Surgery:
Hernia Examination
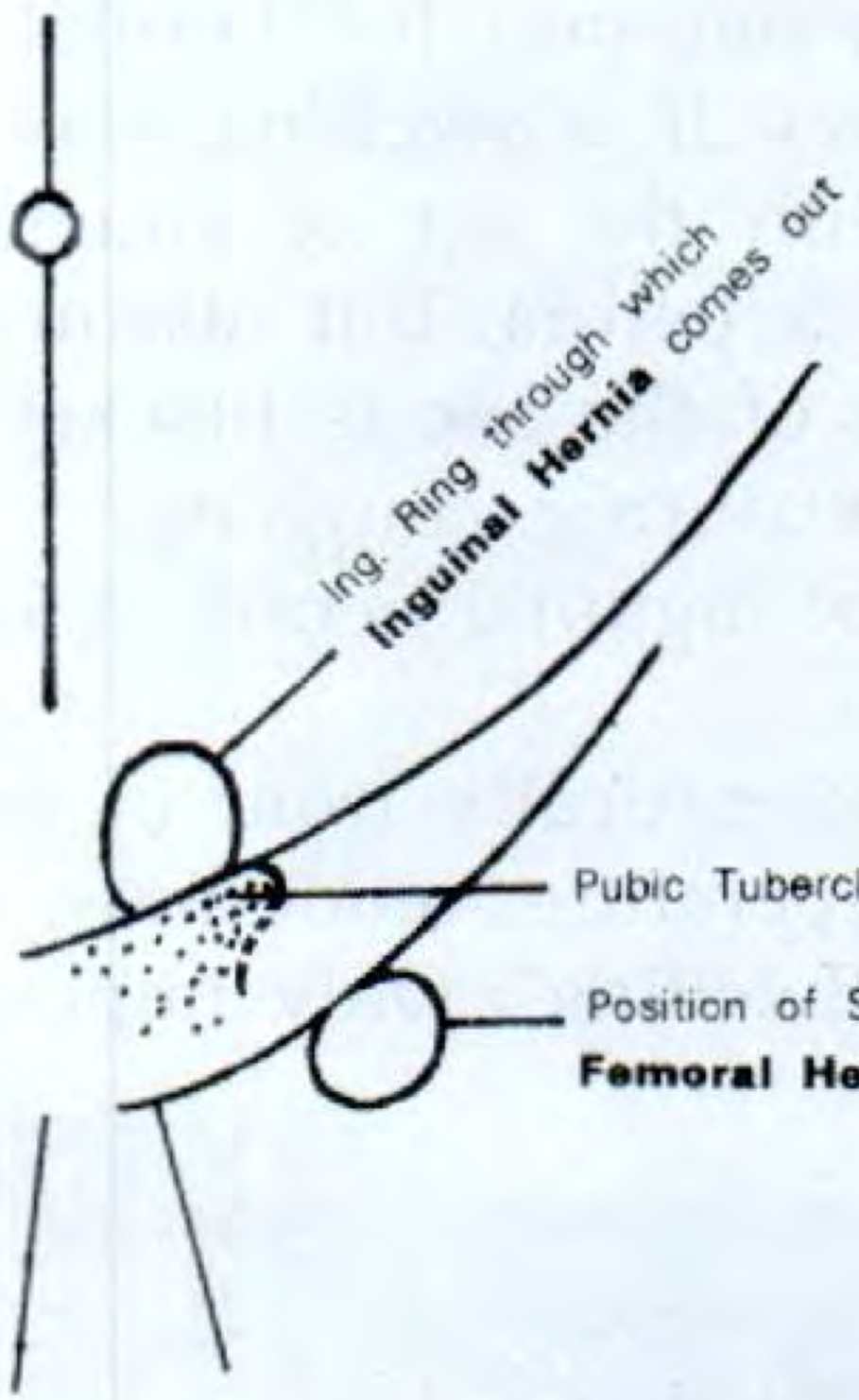
Anatomy Reference
The diagram below shows the close relationships between direct inguinal, indirect inguinal, and femoral hernias - key to understanding examination:

General Principles of Hernia Examination
Patient Positioning
- Examine the patient lying down first, then standing - standing usually increases hernia size
- Some hernias are only apparent with the patient standing
- Ask the patient to cough or perform a Valsalva manoeuvre to make the hernia appear
- For divarication of recti: ask the supine patient to simply lift their head off the pillow
"If a patient describes an intermittent swelling but the surgeon finds no hernia on examination, there still may be a hernia present." - Bailey & Love's Surgery, 28th Ed
Systematic Examination Steps (S. Das)
1. Inspection
- Note site, size, shape, skin color
- Overlying skin is usually normal color
- Cellulitis over the hernia = strangulation = surgical emergency
- Inguinal hernia: look for a swelling above and medial to the pubic tubercle
- Femoral hernia: swelling below and lateral to the pubic tubercle, then turns upward
2. Site Relative to the Pubic Tubercle
This is the single most important landmark to differentiate inguinal from femoral hernia:
| Hernia Type | Relation to Pubic Tubercle |
|---|---|
| Inguinal | Above and medial |
| Femoral | Below and lateral (saphenous opening is 4 cm below and lateral to the pubic tubercle) |
3. Consistency
- Doughy/granular - omentum inside (omentocele/epiplocele)
- Elastic - bowel inside (enterocele)
- Tense and tender - strangulated hernia (most important sign)
4. Relation to Testis and Spermatic Cord (males)
- Inguinal hernia: lies in front and sides of spermatic cord; testis is incorporated within the swelling
- Femoral hernia: does not give rise to scrotal swelling; testis felt separately
- If the hernia stops just above the testis = funicular/acquired variety
Two Classical Signs of an Uncomplicated Hernia
"Two classical signs of an uncomplicated hernia are: (i) Impulse on coughing and (ii) Reducibility." - S. Das
5. Impulse on Coughing (Expansile Cough Impulse)
- Place hand gently over the swelling and ask the patient to cough
- A expansile impulse = hernia contents force out, separating the fingers
- The root of the scrotum can be held between index finger and thumb and felt for impulse on coughing
Absent cough impulse occurs when:
- Neck of the sac is tight - hernia is irreducible/incarcerated
- Strangulation (tense, tender)
- Adhesions blocking sac entry
- Femoral hernia (tight neck - often misdiagnosed as a lymph node)
"A swelling with a cough impulse is not necessarily a hernia. A swelling with no cough impulse may still be a hernia." - Bailey & Love
6. Reducibility
- Ask the patient to attempt reduction themselves first - they may be well-practised
- For inguinal hernia: flex and internally rotate the thigh, squeeze fundus of the sac with one hand, direct hernia through superficial inguinal ring with the other
- For femoral hernia: reduce through the saphenous opening
- Cannot be reduced = irreducible, obstructed, or strangulated hernia - treat more urgently
Special Tests to Differentiate Hernia Type
7. Zieman's Three-Finger Technique (for diagnosis when hernia is reduced or absent)
Stand on the patient's right side. Place three fingers simultaneously:
| Finger | Position | Detects |
|---|---|---|
| Index finger | Over deep inguinal ring (½ inch above the mid-inguinal point*) | Indirect (oblique) inguinal hernia |
| Middle finger | Over superficial inguinal ring | Direct inguinal hernia |
| Ring finger | Over saphenous opening (4 cm below and lateral to pubic tubercle) | Femoral hernia |
Ask the patient to hold the nose and blow (Valsalva) or cough. The finger that feels the impulse identifies the hernia type.
*Mid-inguinal point = midpoint between anterior superior iliac spine (ASIS) and symphysis pubis
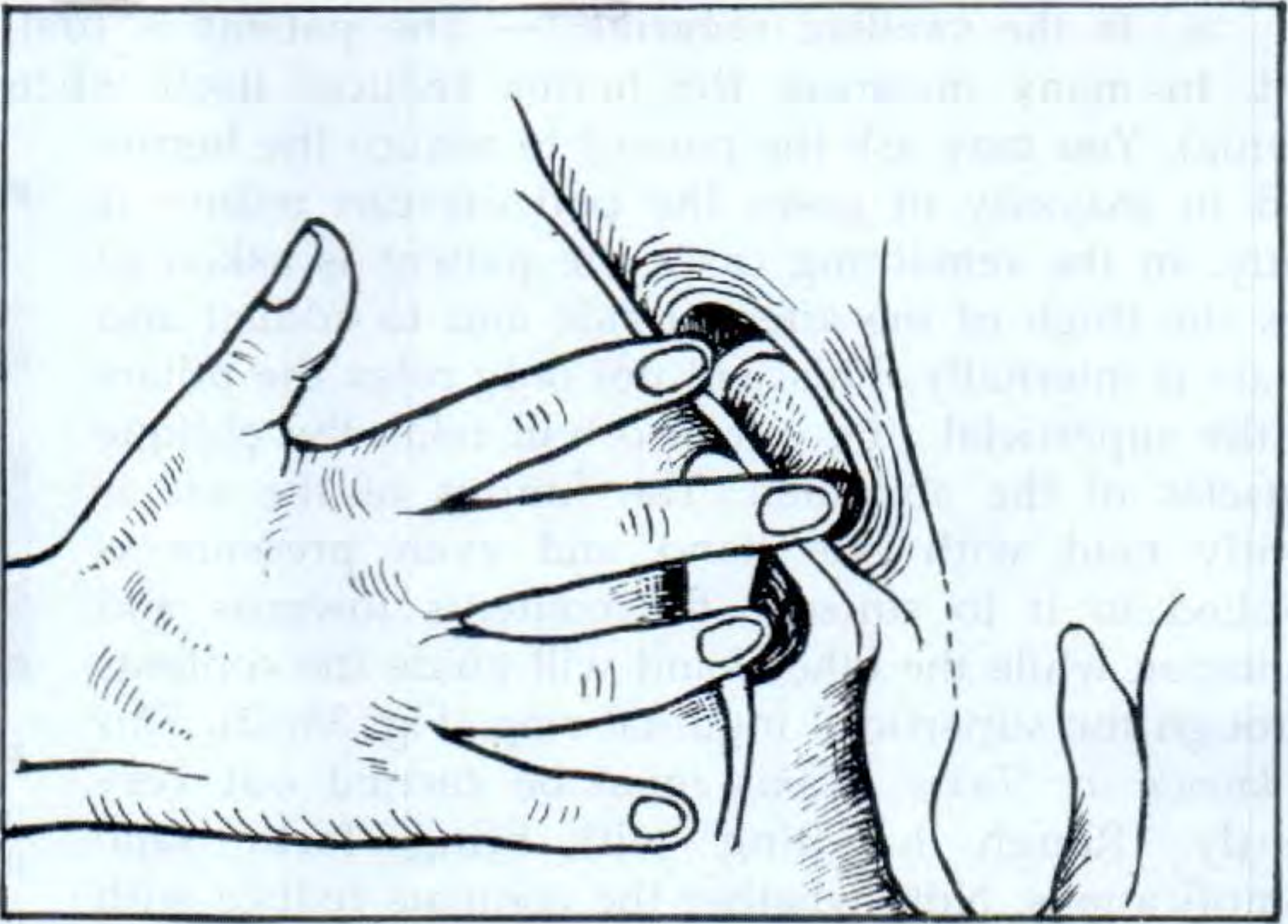
8. Invagination Test (Finger in Ring Test)
- Performed after hernia is reduced, in recumbent position
- Use the little finger (least painful): invaginate the skin from the bottom of the scrotum and push up to palpate the pubic tubercle
- Rotate and push the finger further up into the superficial inguinal ring
- Nail faces anteriorly against the spermatic cord; pulp faces posteriorly toward the ring
- Normal ring = triangular slit admitting only the tip of the finger
- Ask the patient to cough:
- Impulse felt on tip of finger = indirect (oblique) hernia (impulse coming down the canal)
- Impulse felt on pulp of finger = direct hernia (coming straight through posterior wall)
9. Ring Occlusion Test (Confirmatory test: Direct vs. Indirect)
- Performed standing, after hernia is reduced
- Press the thumb firmly over the deep inguinal ring (½ inch above the mid-inguinal point)
- Ask the patient to cough:
| Result | Interpretation |
|---|---|
| No bulge with ring occluded | Indirect hernia (ring is blocked, hernia cannot come out) |
| Bulge appears medial to the thumb | Direct hernia (comes through Hesselbach's triangle, not through the ring) |
| Occluding the femoral canal prevents hernia | Confirms femoral hernia |
Direct vs. Indirect Inguinal Hernia: Key Differences
| Feature | Indirect (Lateral/Oblique) | Direct (Medial) |
|---|---|---|
| Pathway | Through deep inguinal ring, down canal | Through posterior wall (Hesselbach's triangle) |
| Relation to inferior epigastric vessels | Lateral | Medial |
| Type | Congenital or acquired | Acquired only |
| Descent to scrotum | Yes | Rarely |
| Ring occlusion test | Hernia controlled | Hernia NOT controlled (medial bulge) |
| Strangulation risk | Higher | Lower |
| Common in | Young men | Older men |
Femoral Hernia Examination Points
- Appears below and lateral to the pubic tubercle, lies in the upper leg
- Often rapidly becomes irreducible and loses cough impulse
- May be only 1-2 cm - easily mistaken for a lymph node
- More common in thin, elderly women
- 50% present as an emergency with very high strangulation risk
- Diagnostic error is common due to inadequate exposure
- No scrotal swelling
Differential diagnosis of femoral hernia swelling:
- Inguinal hernia
- Lymph node
- Saphena varix (also has cough impulse - distinguish by compressibility and thrill)
- Femoral artery aneurysm
- Psoas abscess
- Rupture of adductor longus with haematoma
Examination Checklist (Bailey & Love Summary)
| Check | What to Assess |
|---|---|
| Reducibility | Can it be reduced manually? |
| Cough impulse | Expansile = positive; absent in strangulation/tight neck |
| Tenderness | Suggests obstruction or strangulation |
| Overlying skin | Erythema = strangulation (emergency) |
| Multiple defects | Check contralateral side - occult hernia in up to 20% |
| Signs of previous repair | Scar |
| Scrotal content | For groin hernias |
| Associated pathology | Ascites, abdominal masses |
Examination in Children
- Thick fat pad may hide a small hernia - ask the child to jump off the examining table or make it cry
- Palpate the spermatic cord at the superficial ring: thicker than the contralateral side = hernia present
- All inguinal hernias in neonates and children are indirect (congenital) - patent processus vaginalis
Investigations
- Clinical diagnosis is usually sufficient for inguinal hernia
- Ultrasound or CT if doubt exists (especially for femoral hernia)
- MRI for occult/recurrent hernias or atypical presentations
Sources: S. Das Manual on Clinical Surgery 13th Ed, pp. 602-606; Bailey & Love's Short Practice of Surgery 28th Ed, pp. 1086-1090, 1087-1090, 2287-2347; Schwartz's Principles of Surgery 11th Ed
This is a shared conversation. Sign in to Orris to start your own chat.