Applied aspect of ischial spine in gynecology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
I now have all the material needed for a comprehensive answer. Here is a structured overview of the applied aspects of the ischial spine in gynecology:
Applied Aspects of the Ischial Spine in Gynecology
Anatomy Recap
The ischial spine is a sharp bony projection from the posterior border of the ischium. It delineates the greater sciatic notch (above) from the lesser sciatic notch (below), and serves as the lateral apex of the sacrospinous ligament. — Berek & Novak's Gynecology, p. 149
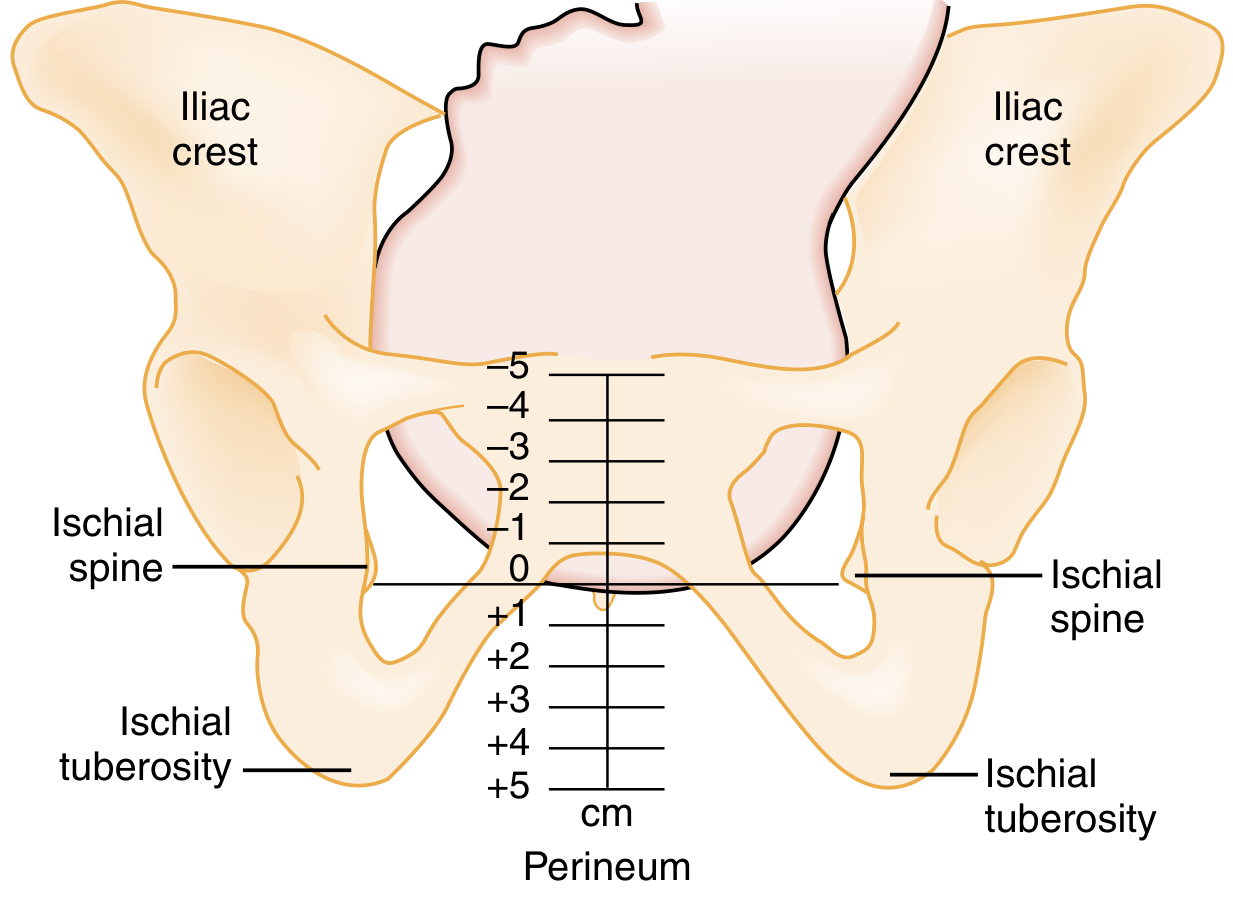
1. Assessment of Fetal Station in Labour
This is the most fundamental obstetric application of the ischial spine.
- The level of the ischial spines = Station 0 — the reference point for measuring fetal descent.
- Stations are expressed in cm above (−) or below (+) the ischial spines, ranging from −5 to +5.
- Engagement of the fetal head is clinically defined as the leading bony part of the head reaching station 0 (at or below the ischial spines). When the lowermost portion of the fetal head is above the ischial spines, the biparietal diameter has likely not passed through the pelvic inlet.
- The ischial spines are palpated transvaginally during labour to assess descent.
Exception: When there is significant moulding or caput succedaneum, the head may appear at 0 station without true engagement. — Pfenninger & Fowler's Procedures for Primary Care, p. 1174
2. Pudendal Nerve Block
The ischial spine is the key landmark for pudendal nerve block, used in:
- Pain relief during the second stage of labour (when epidural is unavailable or contraindicated)
- Instrumental (forceps/vacuum) deliveries
- Repair of perineal lacerations/episiotomy
- Certain chronic pelvic pain conditions, anorectal, and urological procedures
Anatomical basis: The pudendal nerve (S2–S4) exits the pelvis through the greater sciatic foramen, hooks around the ischial spine and sacrospinous ligament, and re-enters the perineum through the lesser sciatic foramen. This U-turn at the ischial spine makes it the ideal injection site.
Technique:
- A finger inserted into the vagina palpates the ischial spine.
- The needle is directed transcutaneously (or transvaginally) to the medial aspect of the ischial spine, just posterior to the sacrospinous ligament attachment.
- Local anaesthetic is infiltrated to anaesthetize the perineum.
- Can also be performed under ultrasound, CT, or fluoroscopic guidance.
— Gray's Anatomy for Students, p. 512; Morgan & Mikhail's Clinical Anesthesiology

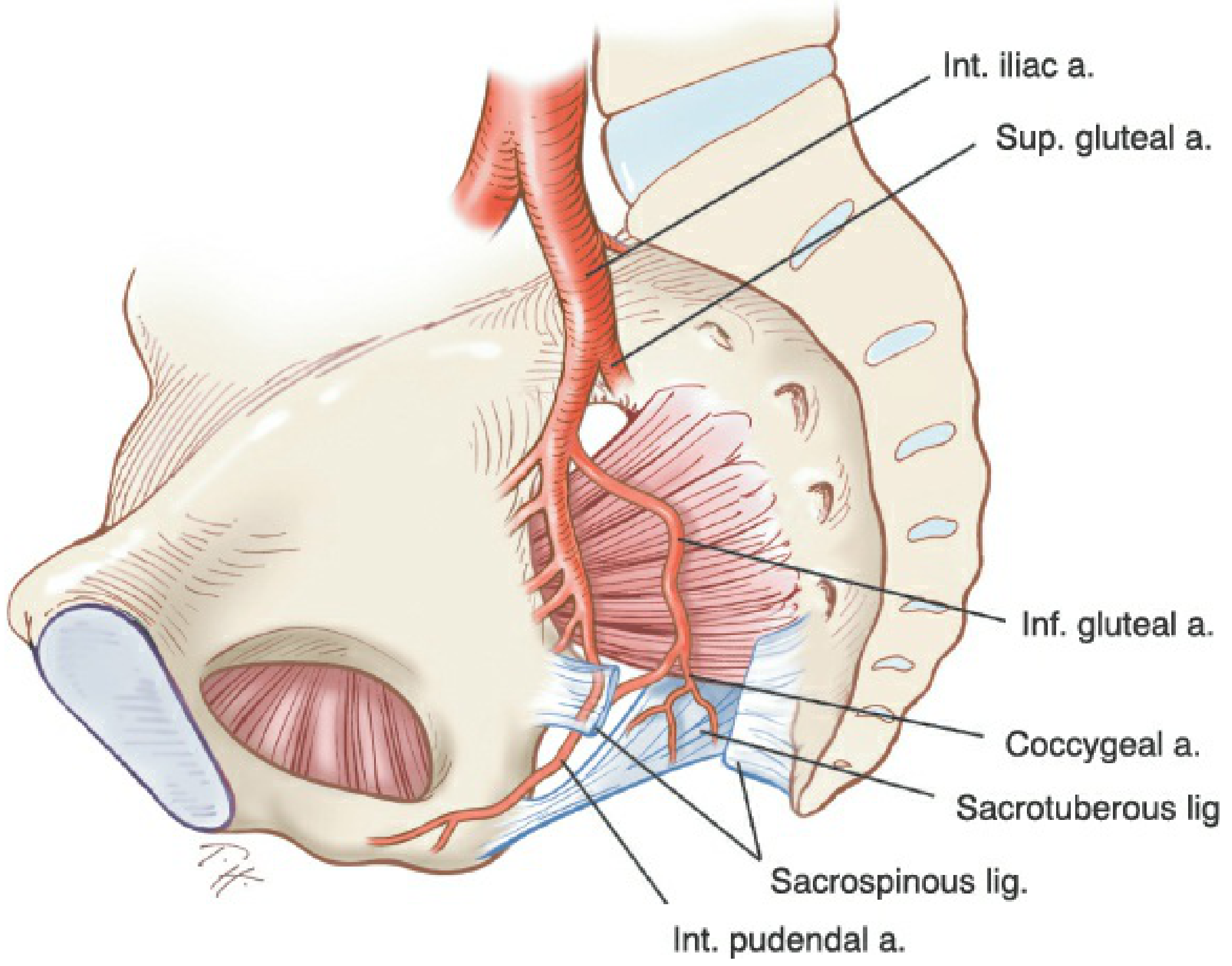
3. Sacrospinous Ligament Fixation (Vaginal Vault Suspension)
The sacrospinous ligament extends from the ischial spine to the lateral sacrum and is widely used for vaginal vault suspension in pelvic organ prolapse.
Relevance of the ischial spine:
- The ischial spine marks the lateral extremity of the sacrospinous ligament — the most accessible end during transvaginal surgery.
- Sutures must be placed at least 2 fingerbreadths medial to the ischial spine to avoid:
- The pudendal nerve and internal pudendal vessels (lie anterior to the ligament at the ischial spine attachment)
- The inferior gluteal artery (lies between the sacrospinous and sacrotuberous ligaments)
— Berek & Novak's Gynecology, p. 152
4. Arcus Tendineus Fasciae Pelvis (ATFP) and Paravaginal Support
The ischial spine is the posterior anchor of the ATFP (the "white line"):
- The ATFP runs from the anterior pubis to the ischial spine along the obturator internus fascia.
- It provides lateral paravaginal support to the anterior vaginal wall.
- Detachment of the pubocervical/pubourethral fascia from the ATFP leads to a lateral (paravaginal) cystocele.
- Paravaginal defect repair reattaches the lateral vaginal sulcus to the ATFP, tracing it back to the ischial spine.
The arcus tendineus levator ani also terminates at the ischial spine and serves as the attachment point for the pubococcygeus and iliococcygeus muscles.
— Berek & Novak's Gynecology, p. 212
5. Pelvimetry and Pelvic Capacity Assessment
The interspinous diameter (distance between the two ischial spines) is:
- The narrowest diameter of the pelvic outlet in the transverse plane
- Normal value: ≥10.5 cm
- A reduced interspinous diameter predicts obstructed labour and guides decisions about mode of delivery
- Prominent ischial spines that encroach medially narrow this diameter significantly ("funnel pelvis" or android type)
6. Uterosacral Ligament Suspension
In high uterosacral ligament suspension for vaginal vault prolapse, the ischial spine is used as an intraoperative anatomical reference point to identify the level at which uterosacral ligament sutures are placed (typically at or above the ischial spine level to achieve adequate apical support). — Berek & Novak's Gynecology, Chapter on Prolapse Surgery
Summary Table
| Applied Aspect | How the Ischial Spine Is Used |
|---|---|
| Fetal station | Station 0 reference; transvaginal palpation to assess descent |
| Engagement | Head at/below spine = engaged (with caveats for moulding/caput) |
| Pudendal nerve block | Landmark for needle placement; nerve hooks around spine |
| Sacrospinous fixation | Lateral extremity of ligament; sutures ≥2 cm medial to avoid neurovascular injury |
| ATFP / paravaginal repair | Posterior anchor of white line; detachment → lateral cystocele |
| Pelvimetry | Interspinous diameter = narrowest outlet dimension (normal ≥10.5 cm) |
| Uterosacral suspension | Reference for suture placement level |
Sources: Berek & Novak's Gynecology (p. 149–152, 212); Gray's Anatomy for Students (p. 511–512); Rosen's Emergency Medicine; Pfenninger & Fowler's Procedures for Primary Care; Morgan & Mikhail's Clinical Anesthesiology.
This is a shared conversation. Sign in to Orris to start your own chat.