Ecg
Asking for Preferences
Reading File
Finding Sources
Searching Images
ECG basic interpretation waveform P QRS T intervals
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive guide to basic ECG interpretation, drawn from Braunwald's Heart Disease, Medical Physiology (Boron & Boulpaep), and the Harriet Lane Handbook.
How to Read an ECG — Systematic Approach
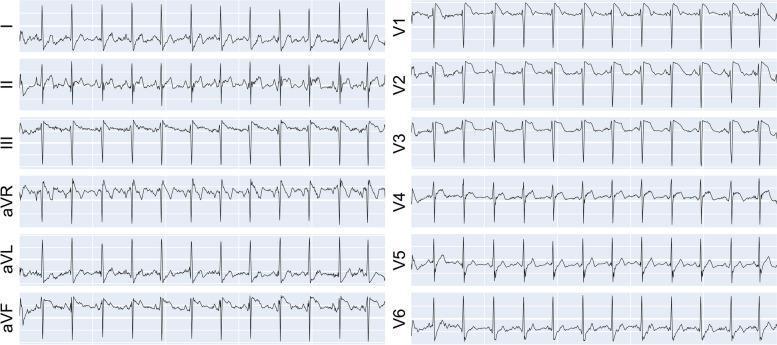
The 12-Lead ECG Layout
A standard 12-lead ECG uses:
- Limb leads: I, II, III, aVR, aVL, aVF (frontal plane)
- Precordial leads: V1–V6 (horizontal plane)
ECG Paper & Calibration
| Measurement | Value |
|---|---|
| Paper speed | 25 mm/sec |
| 1 small box (1 mm) | 0.04 sec horizontally / 0.1 mV vertically |
| 1 large box (5 mm) | 0.20 sec |
| 5 large boxes | 1.0 second |
| Standard voltage | 10 mm = 1 mV |
Step-by-Step Interpretation
1. Rate
Quick method: Count the large boxes between two R waves, then use:
Rate = 300 ÷ (number of large boxes between R peaks)
| Large boxes between R waves | Heart rate |
|---|---|
| 1 | 300 bpm |
| 2 | 150 bpm |
| 3 | 100 bpm |
| 4 | 75 bpm |
| 5 | 60 bpm |
| 6 | 50 bpm |
Normal: 60–100 bpm. <60 = bradycardia. >100 = tachycardia.
2. Rhythm
Ask three questions:
- Where is the pacemaker? — Normal = SA node
- What is the conduction path? — Normal: SA node → AV node → Bundle of His → Purkinje fibers
- Is it regular and at the right rate?
Normal sinus rhythm (NSR) criteria:
- Every QRS is preceded by a P wave
- P wave is upright in leads I and aVF (normal P-wave axis)
- Regular R-R intervals with normal respiratory variation
3. Axis (QRS Axis)
The normal QRS axis in the frontal plane is −30° to +90°.
| Axis | Value |
|---|---|
| Normal | −30° to +90° |
| Left axis deviation (LAD) | More negative than −30° |
| Right axis deviation (RAD) | More positive than +90° |
Quick method: Look at leads I and aVF:
- Both positive → Normal axis
- I positive, aVF negative → Left axis deviation
- I negative, aVF positive → Right axis deviation
- Both negative → Extreme axis deviation
4. Intervals & Waveforms
Waveforms and what they represent
| Waveform | Represents |
|---|---|
| P wave | Atrial depolarization |
| QRS complex | Ventricular depolarization |
| T wave | Ventricular repolarization |
| U wave | Possibly Purkinje repolarization (small, follows T) |
Normal interval values
| Interval | Normal Duration | Clinical Significance |
|---|---|---|
| PR interval | 0.12–0.20 sec (3–5 small boxes) | AV node conduction time |
| QRS duration | <0.12 sec (<3 small boxes) | Ventricular conduction time |
| QT interval | <0.44 sec (rate-corrected) | Ventricular action potential duration |
| QTc (Bazett formula) | ≤0.44 s (males), ≤0.46 s (females) | QT corrected for heart rate |
Bazett formula for QTc:
QTc = QT (sec) ÷ √R-R interval (sec)
5. P-Wave Morphology
- Duration: <0.12 sec in adults
- Amplitude: <2.5 mm (0.25 mV)
- Bifid or broad P → Left atrial enlargement (P mitrale)
- Tall, peaked P >2.5 mm → Right atrial enlargement (P pulmonale)
6. QRS Complex
- Normal duration: <0.12 sec
- R-wave progression (precordial leads): R wave should increase from V1 to V5/V6
- Pathological Q waves: >0.04 sec wide or >1/4 the height of the R wave → suggests prior infarction
- Wide QRS (≥0.12 sec) → Bundle branch block or ventricular origin
7. ST Segment
The ST segment lies between the end of the QRS (J point) and the start of the T wave. Normally it sits at the isoelectric baseline.
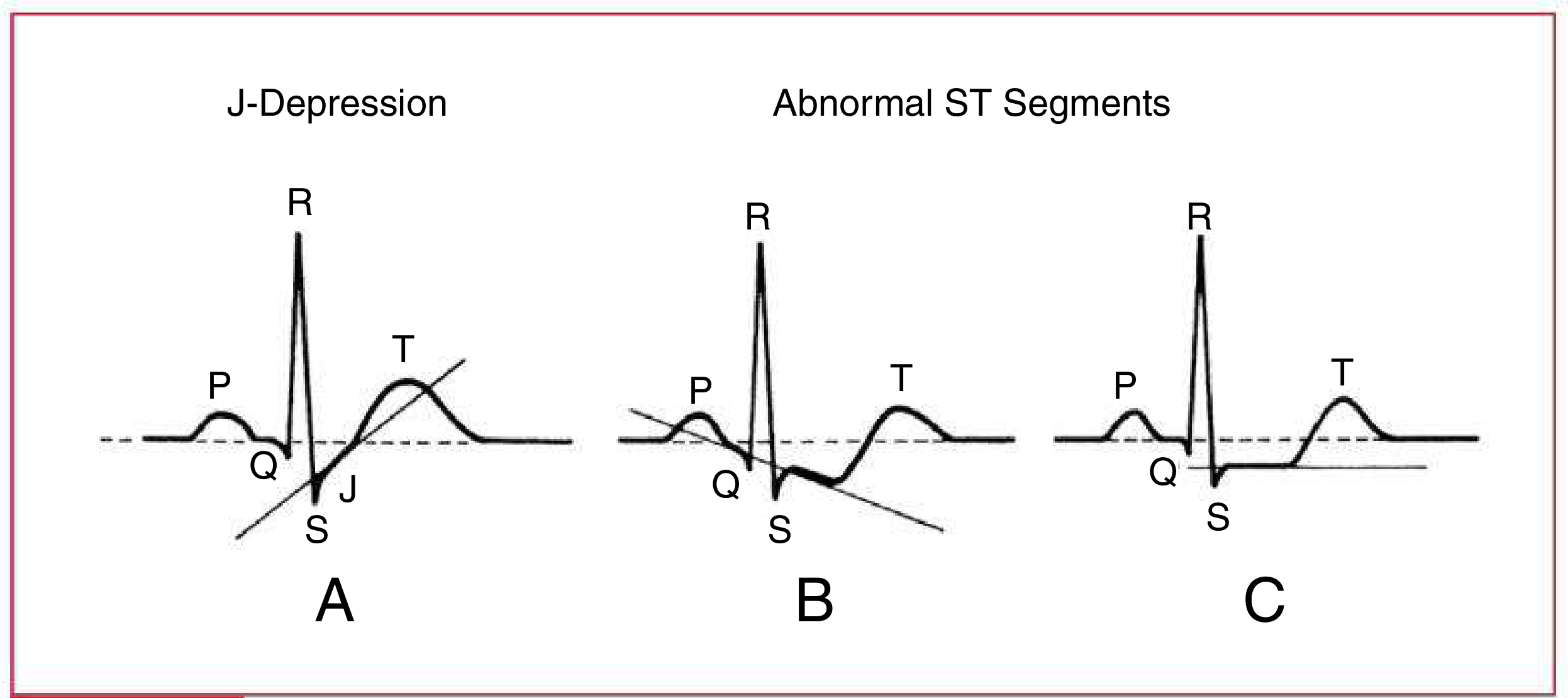
- ST elevation (≥1 mm in limb leads, ≥2 mm in precordial leads) → STEMI until proven otherwise
- ST depression (horizontal or downsloping) → Ischemia or NSTEMI
- J-depression with upsloping ST → Non-ischemic, benign variant
8. T-Wave
- Normally upright in leads I, II, V4–V6
- Normally inverted in aVR (always)
- T inversion in V1–V4 → Right heart strain, RBBB, or ischemia
- Tall, peaked T waves → Hyperkalemia or hyperacute MI
Summary: The 8-Step Checklist
| Step | What to assess |
|---|---|
| 1 | Rate — tachycardia / bradycardia? |
| 2 | Rhythm — sinus? Regular? |
| 3 | Axis — normal / LAD / RAD? |
| 4 | PR interval — prolonged (heart block)? Short (WPW)? |
| 5 | QRS duration — wide (BBB) or narrow? |
| 6 | ST segment — elevation or depression? |
| 7 | T waves — inverted, peaked, or flat? |
| 8 | QTc — prolonged (risk of torsades)? |
Sources: Medical Physiology (Boron & Boulpaep), Box 21-2 | Braunwald's Heart Disease, Ch. 61 | Harriet Lane Handbook, Ch. 7
This is a shared conversation. Sign in to Orris to start your own chat.