Oligodendroglioma imaging features
Reading File
Finding Sources
Searching PubMed
oligodendroglioma MRI imaging features
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is the full answer:
Oligodendroglioma: Imaging Features
Molecular definition (WHO 2021): Oligodendroglioma is defined by IDH mutation + 1p/19q codeletion. This molecular signature takes diagnostic priority over microscopic appearances alone.
Location
- Almost exclusively cerebral hemispheres
- Frontal lobe is the most common site (followed by temporal lobe)
- Typically involves both subcortical white matter and cortex (cortico-subcortical involvement is characteristic)
- Patients often present with years of antecedent seizures before diagnosis
CT Features
- Calcification is the hallmark: present in up to 90% of oligodendrogliomas on CT
- Can be central, peripheral, or ribbon-like (gyriform/cortical pattern is characteristic)
- Coarse, dense calcification is more common than in other low-grade gliomas
- Large, partially solid tumour involving cortex
- Cysts may be present
- Mild to moderate enhancement in at least 20% of WHO grade II tumours; does not automatically imply anaplasia
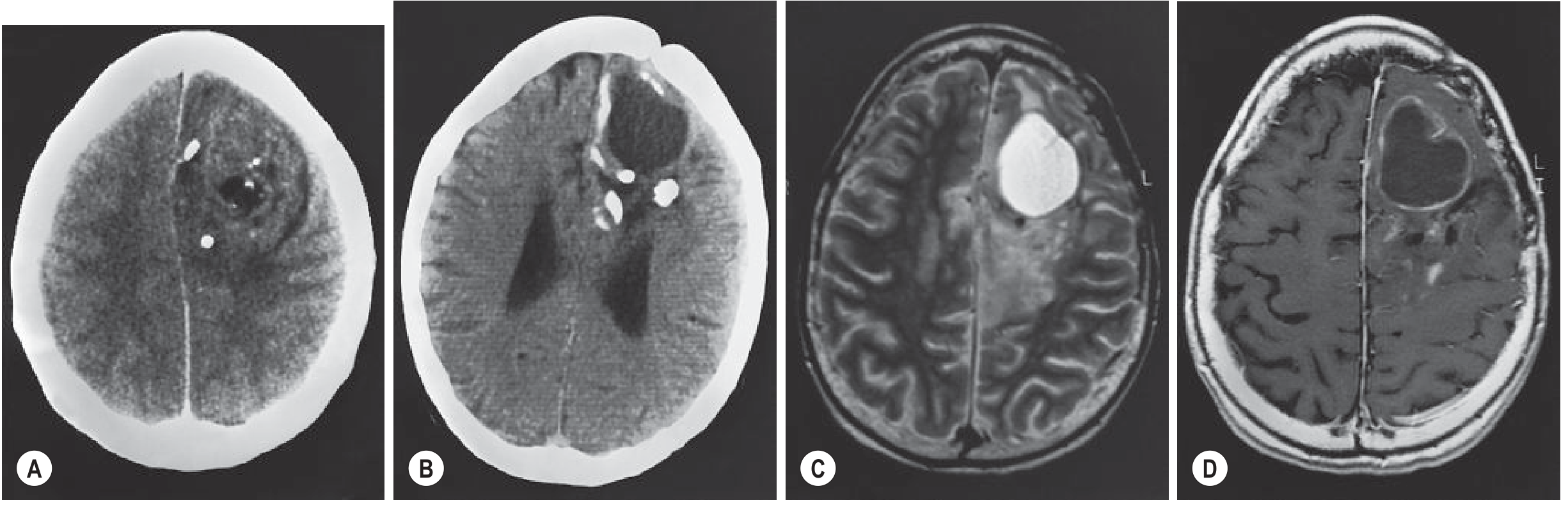
Fig. 55.7 (Grainger & Allison) - WHO Grade II Oligodendroglioma shown below: CT (A) shows large left frontal tumour with cortical involvement, predominantly solid with irregular enhancement, coarse calcification, and cysts. Follow-up CT (B), T2 MRI (C), and T1 post-contrast MRI (D) demonstrate progressive cyst formation and calcification.
MRI Features
| Sequence | Appearance |
|---|---|
| T2/FLAIR | Hyperintense (diffusely infiltrative) |
| T1 | Hypointense |
| T1 post-contrast | Mild-moderate enhancement in ~20-50% of grade II; more common in grade III |
| T2*/SWI | Marked signal loss ("blooming") due to calcification or haemorrhage |
| DWI | Typically no restricted diffusion (unlike higher-grade gliomas) |
Key MRI points:
- Calcification on MRI: Typically T2 hypointense and T1 hyperintense; causes marked signal dropout on T2*/SWI (susceptibility-weighted) sequences
- No FLAIR-mismatch sign - the FLAIR-mismatch sign (T2 bright but FLAIR suppressed solid core) is specific for IDHmut astrocytoma (1p19q-intact), NOT oligodendroglioma - its absence helps differentiate
- Posterior extent and infiltration are best seen on MRI rather than CT
- Calcification appears as non-specific low signal areas on MRI and is much less apparent than on CT
Advanced MRI Features
Perfusion MRI (DSC/PWI)
- Low-grade oligodendrogliomas commonly show moderately elevated rCBV - this can overlap with IDH wild-type (higher grade) features and may prompt early tissue diagnosis
- Both WHO II and III oligodendrogliomas express proangiogenic mitogens and contain regions of increased vascular density with finely branching capillaries ("chicken wire" pattern)
MR Spectroscopy (MRS)
- Increased myo-inositol/glycine, glutamine, and glutamate in low-grade tumours
- Presence of lipid/lactate peaks suggests anaplastic (grade III) transformation
- Where perfusion is non-specifically elevated, MRS can help differentiate anaplastic oligodendroglioma
Enhancement and Grading
- New enhancement or accelerated growth in a known IDHmut 1p/19q-codeleted glioma raises concern for anaplastic transformation (WHO grade III)
- Few, if any, progressive IDHmut 1p/19qdel gliomas ever fulfil histological criteria for glioblastoma (unlike IDHwt astrocytoma)
Imaging vs. Astrocytoma
| Feature | Oligodendroglioma | IDHmut Astrocytoma |
|---|---|---|
| Calcification | Very common (up to 90% on CT) | Less common |
| Enhancement | More common (~20-50% grade II) | Less common in grade II |
| FLAIR mismatch | Absent | Present (~50%) - specific |
| rCBV (perfusion) | Moderately elevated | Usually lower in grade II |
| Gyriform calcification | Characteristic | Rare |
Key Teaching Points
- Calcification on CT is the imaging hallmark - gyriform/cortical pattern is characteristic but not pathognomonic
- On MRI, calcification "blooms" on SWI/T2* - the best sequence to detect it
- Enhancement does not equal high grade, but new/progressive enhancement in a known oligodendroglioma warrants repeat biopsy
- Absence of FLAIR-mismatch sign helps suggest oligodendroglioma over IDHmut astrocytoma when molecular data is unavailable
- Despite elevated perfusion suggesting aggressiveness, prognosis is significantly better than astrocytoma (mean survival ~8-10+ years for grade II)
Sources: Grainger & Allison's Diagnostic Radiology, p. 1407-1408 | Robbins & Kumar Basic Pathology, p. 859-860 | Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.