Hepatorenal syndrome and its management
Reading File
Finding Sources
Searching PubMed
"hepatorenal syndrome" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I now have comprehensive information to write an authoritative answer. Let me compile the full response.
Hepatorenal Syndrome (HRS)
Definition
Hepatorenal syndrome is a form of functional renal failure - occurring without structural kidney pathology - that develops in patients with advanced cirrhosis, acute liver failure, or acute-on-chronic liver failure. The kidneys are histologically normal; their dysfunction is driven by profound renal arterial vasoconstriction secondary to systemic and splanchnic hemodynamic derangements. Importantly, the condition is potentially reversible if the underlying liver disease is corrected.
HRS occurs in roughly 10-30% of hospitalized cirrhotic patients with AKI, with an annual incidence of ~8% among cirrhotics with ascites - rising to ~30% when SBP or infection is present.
Pathophysiology
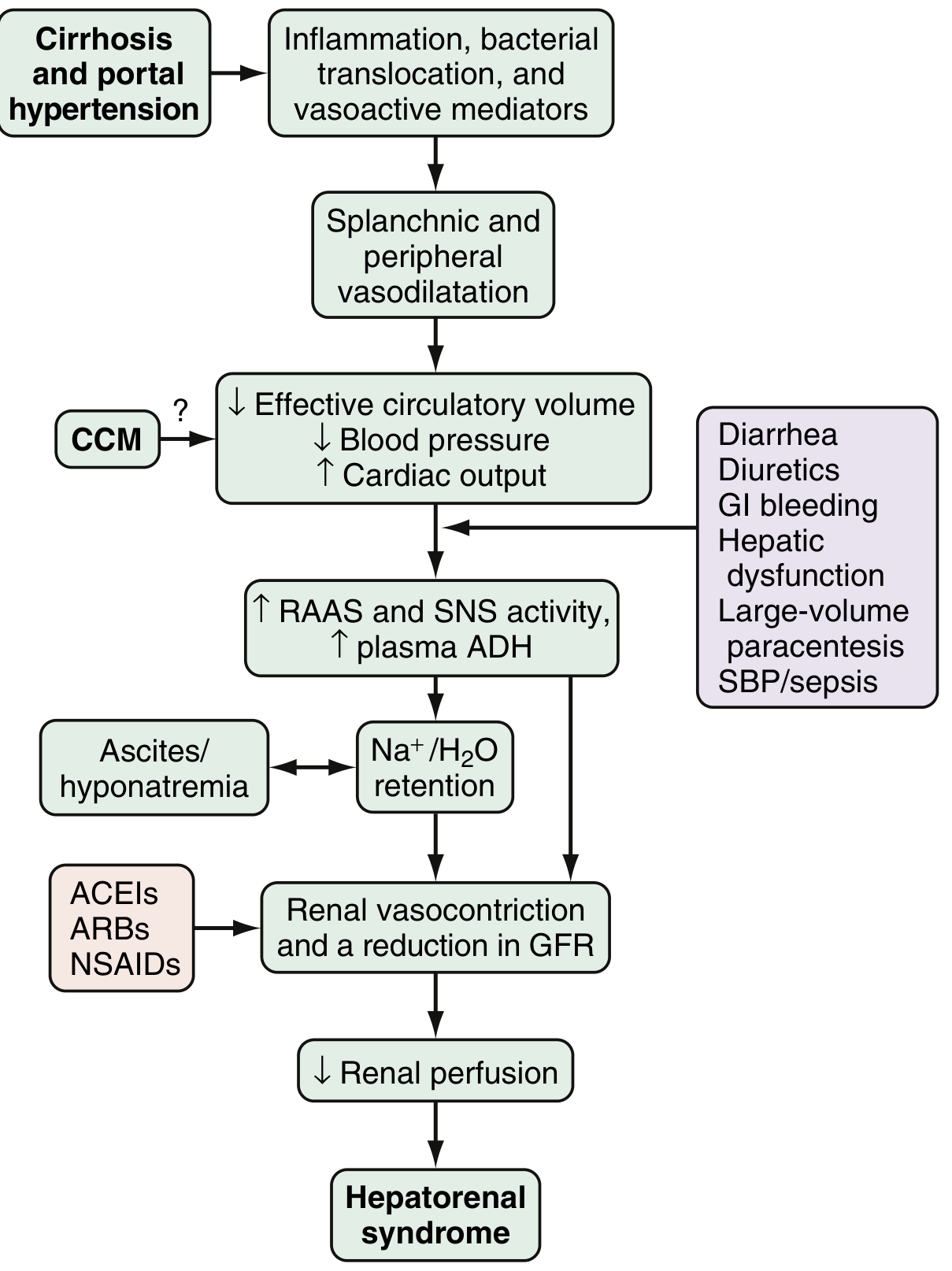
The central mechanism involves three interacting components:
1. Splanchnic and Systemic Arterial Vasodilation
In cirrhosis and portal hypertension, vasoactive mediators - primarily nitric oxide (NO), carbon monoxide, glucagon, prostacyclin, and adrenomedullin - are released in response to inflammation, bacterial translocation, and mechanical signals. This produces marked splanchnic and peripheral vasodilation, reducing effective circulating blood volume and arterial pressure.
2. Compensatory Renal Vasoconstriction
The fall in effective circulatory volume triggers compensatory activation of:
- The renin-angiotensin-aldosterone system (RAAS)
- The sympathetic nervous system (SNS)
- Non-osmotic release of arginine vasopressin (ADH)
These lead to renal sodium and water retention, but as cirrhosis progresses, compensatory vasoconstriction in the kidney becomes overwhelming. Altered intrarenal production of endothelins, prostaglandins, and F2-isoprostanes further worsen renal perfusion, reducing GFR. With prolonged intense vasoconstriction, tubular damage may occur and HRS transitions from a functional to an organic disease.
3. Cardiac Dysfunction (Cirrhotic Cardiomyopathy)
Impaired cardiac output, seen in cirrhotic cardiomyopathy (CCM), further reduces renal perfusion and is an independent risk factor for HRS development. Studies show patients who develop HRS have lower baseline cardiac output and more severe arterial vasodilation than those who do not.
Precipitants include: SBP/sepsis, GI hemorrhage, large-volume paracentesis without albumin replacement, overdiuresis, lactulose-induced diarrhea, nephrotoxic drugs (NSAIDs, ACEIs, ARBs, aminoglycosides).
Classification (Updated ICA Terminology)
| Old Term | New Term | Characteristics | Prognosis |
|---|---|---|---|
| Type 1 HRS | HRS-AKI | Rapid, progressive renal deterioration over 1-2 weeks; creatinine >2.5 mg/dL or doubles in <2 weeks | Median survival ~2 weeks without treatment |
| Type 2 HRS | HRS-CKD (or HRS-NAKI) | More gradual, stable-to-slowly progressive renal failure; associated with refractory ascites | Median survival 4-6 months |
Diagnostic Criteria (ICA 2015 Revised Criteria)
HRS is a diagnosis of exclusion. All of the following must be present:
- Cirrhosis with ascites
- AKI by ICA-AKI criteria:
- Rise in serum creatinine ≥0.3 mg/dL within 48 hours, OR
- ≥50% rise from baseline within 7 days
- No response after at least 48 hours of diuretic withdrawal AND albumin volume expansion (1 g/kg/day, max 100 g/day)
- Absence of shock
- No current/recent nephrotoxic agents (NSAIDs, aminoglycosides, contrast agents)
- No intrinsic renal disease - i.e., no proteinuria >500 mg/day, no microhematuria (>50 RBC/HPF), no abnormal renal ultrasound
HRS-AKI is classified as Stage 2 or 3 AKI. Typical urine findings: urine sodium <10 mmol/L, urine osmolality > plasma osmolality (tubular function preserved).
Note: Muscle wasting and reduced urea synthesis in end-stage liver disease may lower baseline creatinine, masking the degree of renal impairment. Cystatin C may be a more accurate marker in this setting.
Differential diagnosis of AKI in cirrhosis:
- Pre-renal: GI bleeding, overdiuresis, diarrhea
- Sepsis/SBP (30% of SBP patients develop AKI/HRS)
- Drug-induced: NSAIDs, ACEIs/ARBs, aminoglycosides, contrast
- Intrinsic: acute tubular necrosis, IgA nephropathy, membranoproliferative GN
- Obstructive: rare
Management
Prevention (Most Important Step)
- Avoid intravascular volume depletion: do not over-diurese; give albumin 6-8 g per liter of ascites removed during large-volume paracentesis (>5L)
- Albumin 1.5 g/kg on day 1 + 1 g/kg on day 3 in patients with SBP - reduces AKI and improves survival
- Avoid NSAIDs, ACEIs, ARBs, nephrotoxic antibiotics
- Prompt treatment of infections (SBP prophylaxis with norfloxacin/ciprofloxacin)
- SBP prophylaxis in high-risk patients (prior SBP, variceal hemorrhage)
- Pentoxifylline for severe alcohol-associated hepatitis (though efficacy is debated in recent trials)
Treatment Algorithm
Step 1: Stop precipitants
- Discontinue all diuretics, NSAIDs, ACEIs, ARBs, nephrotoxic agents
- Treat infection if present (antibiotics)
Step 2: Volume expansion
- IV albumin 1 g/kg/day for 48 hours (max 100 g/day)
- If no improvement in creatinine, proceed to vasopressor therapy
Step 3: Vasopressor therapy (combined with albumin)
| Agent | Regimen | Notes |
|---|---|---|
| Terlipressin (1st line) | 1 mg IV q4h; increase to 2 mg q4h if creatinine does not fall ≥25% by day 3. Continue for up to 14 days or until HRS reverses | FDA-approved in the US (2022, CONFIRM trial). Monitor for respiratory failure - check O2 saturation carefully. Ischemic complications possible. |
| Norepinephrine (2nd line) | 0.1-0.7 mcg/kg/min IV; titrate to MAP increase ≥10 mmHg | Requires ICU. Comparable efficacy to terlipressin in some studies. |
| Midodrine + Octreotide + Albumin (3rd line, outpatient-feasible) | Midodrine 2.5-15 mg TID PO; octreotide 100-200 mcg SC TID (or 25 mcg/hr IV); albumin 20-60 g/day | Less efficacious than terlipressin. Titrate midodrine to MAP increase ≥15 mmHg. Commonly used in the US when terlipressin unavailable. |
Goal of vasoconstrictor therapy: Reverse splanchnic vasodilation, increase MAP, and reduce renal vascular resistance. HRS reversal is defined as creatinine returning to within 0.3 mg/dL of baseline.
Step 4: Renal replacement therapy (RRT)
- For patients who do not respond to vasopressors or develop life-threatening uremic complications
- Acts as a bridge to liver transplantation, not a curative treatment
Step 5: TIPS (Transjugular Intrahepatic Portosystemic Shunt)
- Reduces portal hypertension and can improve renal function in selected patients
- Evidence is strongest for HRS-CKD (type 2) and refractory ascites
- Contraindicated in severe hepatic encephalopathy, advanced liver failure (MELD >18-20), cardiac dysfunction
Step 6: Liver Transplantation (Definitive Treatment)
- The only cure for HRS
- Recovery of renal function occurs in the majority after transplant
- Patients with HRS-AKI or HRS-CKD have poor prognosis unless transplant is achieved
- Combined liver-kidney transplant (SLKT) may be considered for patients with prolonged AKI (>4-6 weeks) or underlying CKD
Prognosis
- HRS-AKI (type 1): Median survival ~2 weeks without treatment; with terlipressin + albumin, HRS reversal achieved in ~30-40% but overall mortality remains high without transplant
- HRS-CKD (type 2): Median survival 4-6 months
- After liver transplantation: most patients recover renal function; prognosis is substantially better
Recent Evidence (2024-2026)
The 2024 AGA Clinical Practice Update (Garcia-Tsao et al., Gastroenterology 2024, PMID 37978969) addressed the use of vasoactive drugs and IV albumin in cirrhosis, reinforcing terlipressin as first-line for HRS-AKI, with careful monitoring for respiratory failure. The 2025 AGA Update on Ascites Management (PMID 41114681) also updated guidance on volume management relevant to HRS prevention.
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter 94 (most comprehensive coverage)
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- Sabiston Textbook of Surgery, 21st Ed.
- Goldman-Cecil Medicine
- AGA Clinical Practice Updates 2024-2025 (PMIDs 37978969, 41114681)
This is a shared conversation. Sign in to Orris to start your own chat.