Give me the notes of migraine medicine topic, detailed notes.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed to write comprehensive notes. Here are the detailed migraine medicine notes:
🧠 Migraine Medicine — Detailed Notes
1. Overview & Classification
Migraine is a prevalent, largely familial neurological disorder affecting 10–20% of the population. It is characterized by periodic, commonly unilateral, pulsatile headaches that begin in childhood, adolescence, or early adult life. Women are 3× more likely than men to be affected.
Two main clinical types (IHS classification):
| Type | Features |
|---|---|
| Migraine without aura (Common migraine) | Unheralded onset; severe, unilateral, throbbing; lasts 4–72 h; accompanied by nausea, photophobia, phonophobia, aggravated by movement |
| Migraine with aura (Classic migraine) | Preceded by neurological symptoms (aura), usually visual (flashes, zigzag lines, glare); aura lasts ~20–40 min before headache |
Diagnostic criteria (IHS):
Repeated attacks lasting 4–72 h with ≥2 of: unilateral pain, throbbing, aggravated by movement, moderate/severe intensity — PLUS ≥1 of: nausea/vomiting, photophobia & phonophobia.
2. Pathophysiology
2a. Vascular & Neural Mechanisms
- Migraine with aura: begins as cortical spreading depression — hypoperfusion spreading forward over the cortex, persisting through the aura and into the headache phase
- Migraine without aura: no hypoperfusion, but pain arises from extracranial and intracranial arterial vasodilation
- Vasodilation leads to release of neuroactive molecules: substance P, neurokinin A, and CGRP (calcitonin gene-related peptide)
2b. Serotonin (5-HT) Hypothesis
Evidence implicating 5-HT:
- Plasma/platelet 5-HT concentrations vary with migraine phases
- Urinary 5-HT and metabolites are elevated during most attacks
- Migraine can be precipitated by agents that release 5-HT (e.g., reserpine, fenfluramine)
- 5-HT1B/1D receptor agonists (triptans) are highly effective acutely
2c. CGRP Role
- CGRP is a potent vasodilatory and proinflammatory neuropeptide
- Plasma CGRP levels are elevated during acute migraine attacks
- Successful triptan treatment correlates with decreased blood levels of CGRP
- CGRP blockade is now a central therapeutic strategy
2d. Brainstem Involvement
- PET studies show hypothalamic, dorsal midbrain, and dorsolateral pontine activation during migraine (including the noradrenergic locus coeruleus)
- Lateralization of pontine changes correlates with side of head pain in hemicranial migraine
3. Acute Treatment of Migraine
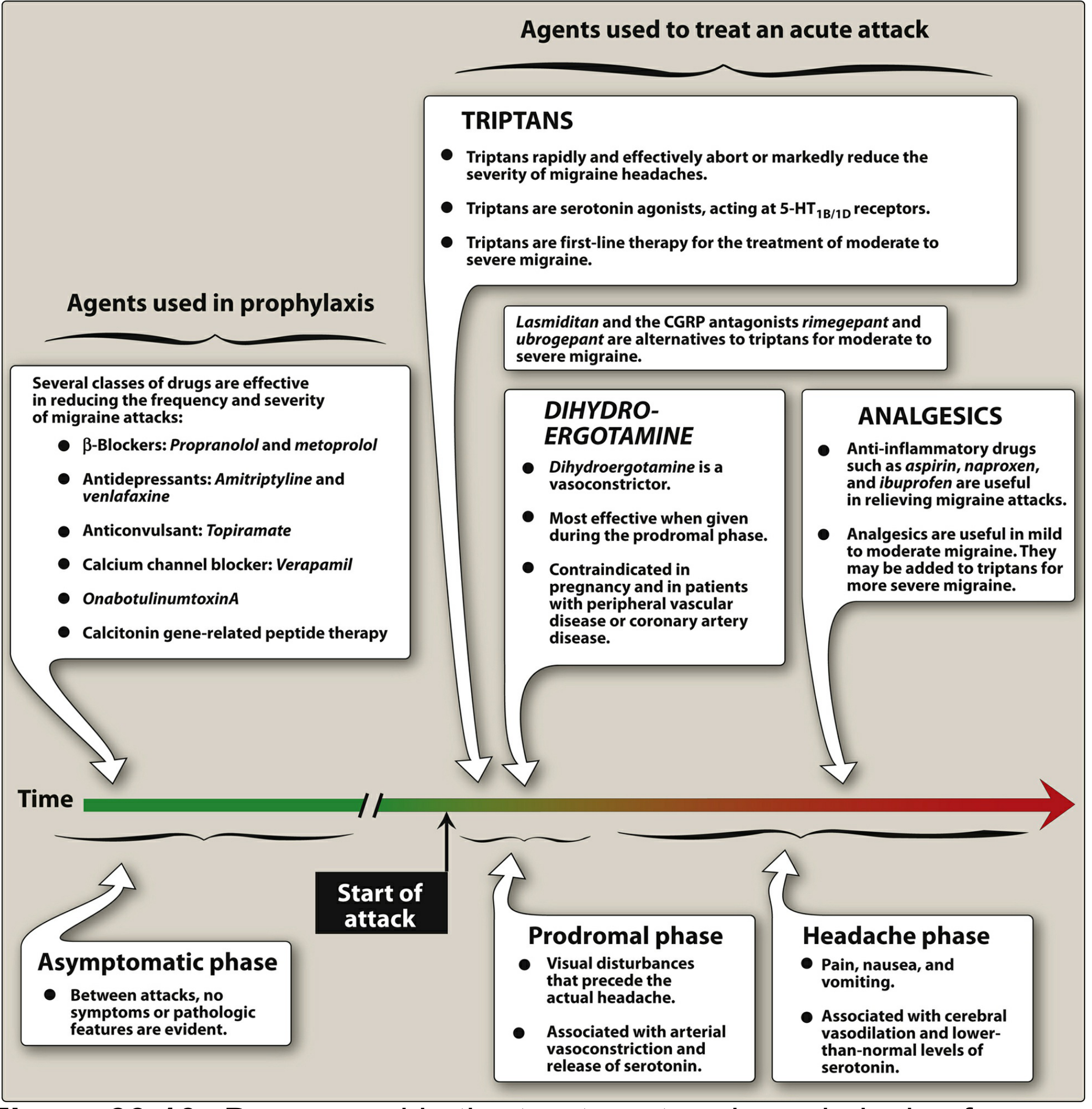
Strategy
- Nonspecific (symptomatic): NSAIDs, analgesics, antiemetics
- Migraine-specific: Triptans, ergot alkaloids, ditans (lasmiditan), CGRP receptor antagonists (gepants)
3.1 Triptans (5-HT1B/1D Receptor Agonists) — First-Line
Agents: Sumatriptan (prototype), almotriptan, eletriptan, frovatriptan, naratriptan, rizatriptan, zolmitriptan
Mechanism:
- Potent agonists at 5-HT1B and 5-HT1D receptors
- Two proposed mechanisms:
- Vasoconstriction of intracranial blood vessels (including AV anastomoses), restoring normal blood flow
- Presynaptic inhibition — block release of proinflammatory neuropeptides (substance P, CGRP) at trigeminal perivascular nerve terminals
Clinical use:
- Effective for acute treatment of migraine with or without aura
- NOT for prophylaxis
- Start treatment as soon as possible after headache onset
- Effective in ~70% of patients
- Sumatriptan 6 mg SC: onset ~20 min; oral: 1–2 h
- Frovatriptan has the longest half-life (>24 h) — useful for menstrual migraine
- Headache may recur within 24–48 h; a second dose is usually effective
Available formulations:
- Sumatriptan: SC injection (fastest), intranasal, oral, oral + naproxen combination
- Zolmitriptan: oral tablet or nasal spray
- All others: oral only
Adverse effects:
- Chest, neck, throat, jaw pressure/pain sensations
- Dizziness, malaise
- Elevated blood pressure
Contraindications:
- Coronary artery disease (or significant risk factors without prior cardiac evaluation) — due to coronary vasospasm risk
- Do not use within 24 h of ergot alkaloids — risk of coronary ischemia
3.2 Ergot Alkaloids
Agents: Ergotamine, Dihydroergotamine (DHE)
Mechanism:
- Complex action at 5-HT1 receptors, α-adrenergic receptors, and dopamine receptors
- 5-HT1 agonism on intracranial blood vessels → vasoconstriction
Ergotamine:
- Available sublingually, orally (+ caffeine), suppository
- Most effective in early stages of migraine
- Strict daily and weekly dosage limits due to risk of dependence and rebound headaches
Dihydroergotamine (DHE):
- IV or intranasal
- Efficacy similar to sumatriptan
- Reserved for severe migraine
- Common adverse effect: nausea
- IV protocol for severe migraine in ED: prochlorperazine 5 mg + DHE 0.5 mg over 2 min
Contraindications:
- Angina and peripheral vascular disease (significant vasoconstrictors)
- Pregnancy
- Do not combine with strong CYP3A4 inhibitors — risk of life-threatening peripheral ischemia
3.3 Ditans — Lasmiditan (5-HT1F Agonist)
Mechanism:
- Selective 5-HT1F receptor agonist
- Reduces activation of trigeminal nerve system pain pathways
- Does NOT cause vasoconstriction — unlike triptans and ergots
Clinical use:
- Oral agent for acute migraine
- Indicated for patients with contraindications or intolerance to triptans (e.g., cardiovascular disease)
Adverse effects / Special considerations:
- Potential for abuse — classified as a controlled substance
- Can cause significant driving impairment — patients must avoid hazardous activities
3.4 CGRP Receptor Antagonists (Gepants)
Agents:
- Ubrogepant — acute treatment only
- Rimegepant — acute treatment AND prevention
- Atogepant — prevention only
- Vazgepant (intranasal) — investigational for acute treatment
Mechanism:
- Block CGRP receptor signaling, reducing vasodilation and neuroinflammation in the trigeminal system
Clinical use:
- Oral agents indicated for acute migraine in patients with contraindications or intolerance to triptans
- Rimegepant and atogepant also used for prevention
Adverse effects:
- Nausea, somnolence (incidence is low)
Drug interaction:
- Ubrogepant: contraindicated with strong CYP3A4 inhibitors
3.5 NSAIDs and Analgesics
- Both the severity and duration of a migraine attack can be reduced significantly by NSAIDs
- Agents: ibuprofen, naproxen, aspirin, indomethacin, ketorolac, diclofenac
- Naproxen combined with sumatriptan (Treximet) is FDA-approved
- For mild to moderate migraine: combination of acetaminophen + aspirin + caffeine is FDA-approved
- Useful adjunct with triptans for more severe migraine
3.6 Antiemetics / Dopamine Receptor Antagonists
- Drug absorption is impaired during migraine (reduced gastric motility), even without overt nausea
- Oral dopamine antagonists (metoclopramide 10 mg, prochlorperazine 10 mg, domperidone 10 mg) enhance gastric absorption of co-administered drugs AND reduce nausea
- Parenteral forms (chlorpromazine, prochlorperazine, metoclopramide IV/IM) can provide significant acute migraine relief; can be combined with parenteral triptans/DHE
- RCT evidence shows prochlorperazine is superior to hydromorphone in ED setting
3.7 Opioids
- Modestly effective; IV meperidine 50–100 mg used in ED
- Not recommended for recurrent headache:
- Do not address underlying headache mechanism
- May decrease future triptan response
- Opioid craving/withdrawal can worsen migraine
- Reserve for: severe but infrequent headaches unresponsive to other approaches, or when other therapies are contraindicated
3.8 Neuromodulation (Acute)
- Single-pulse transcranial magnetic stimulation (sTMS): FDA cleared; 2 pulses at attack onset
- Non-invasive vagus nerve stimulator (nVNS): FDA cleared; 1–2 doses of 120 s each
- Remote electrical neuromodulation: smartphone-app-controlled stimulation of upper arm, 30–45 min
- Transcutaneous supraorbital nerve stimulation: 60 min
- These offer non-pharmaceutical options
4. Preventive (Prophylactic) Treatment of Migraine
When to Initiate Prophylaxis
- ≥4 migraine days/month
- Attacks unresponsive or poorly responsive to acute treatments
- Attacks causing significant disability or neurologic compromise
General principles
- Most agents must be taken daily
- Lag of 2–12 weeks before effect is seen
- Once effective, continue for 6–12 months, then slowly taper
- Probability of success with any one drug: ~40–50%
- Topiramate and valproate are now less attractive in females of reproductive age (fetal developmental concerns)
Harrison's Table: Preventive Treatments in Migraine
| Drug | Dose | Selected Side Effects |
|---|---|---|
| Propranolol (β-blocker) | 40–120 mg bid | Reduced energy, tiredness, postural hypotension; contraindicated in asthma |
| Metoprolol (β-blocker) | 25–100 mg bid | Same as above |
| Amitriptyline (TCA) | 10–75 mg at night | Drowsiness |
| Nortriptyline (TCA) | 25–75 mg at night | Drowsiness |
| Venlafaxine (SNRI) | 75–150 mg/d | — |
| Topiramate (anticonvulsant) | 25–200 mg/d | Paresthesias, cognitive symptoms, weight loss, glaucoma |
| Valproate (anticonvulsant) | — | Weight gain, teratogenic |
| Verapamil (CCB) | — | — |
| Erenumab (anti-CGRP mAb) | SC monthly | — |
| Fremanezumab (anti-CGRP mAb) | SC monthly or quarterly | — |
| Galcanezumab (anti-CGRP mAb) | SC monthly | — |
| Eptinezumab (anti-CGRP mAb) | IV quarterly | — |
| Rimegepant (gepant) | Oral | Nausea |
| Atogepant (gepant) | Oral | Nausea |
| OnabotulinumtoxinA (Botox) | — | Approved for chronic migraine only (negative in episodic migraine trials) |
4.1 Beta-Blockers — Drugs of Choice for Prophylaxis
- Propranolol and metoprolol are the first-line agents
- Mechanism in migraine prophylaxis is not entirely clear (likely not serotonin-related)
- Contraindicated in asthma, heart block, severe depression
4.2 Antidepressants
- Amitriptyline (TCA): most studied; effective regardless of comorbid depression
- Nortriptyline, venlafaxine: alternatives
- Low doses used; benefit unrelated to antidepressant effect
4.3 Anticonvulsants
- Topiramate and Divalproex/valproate: FDA-approved for migraine prevention
- Topiramate: paresthesias, cognitive slowing ("cognitive fog"), weight loss, angle-closure glaucoma
- Valproate: weight gain, teratogenicity — avoid in pregnancy and reproductive-age women
4.4 Calcium Channel Blockers
- Verapamil — used especially when other agents fail or are contraindicated
4.5 CGRP Monoclonal Antibodies (Anti-CGRP mAbs)
- Erenumab (targets CGRP receptor), fremanezumab, galcanezumab, eptinezumab (target CGRP ligand)
- Subcutaneous (monthly or quarterly) except eptinezumab (IV quarterly)
- Highly effective; often work within the first month
- Excellent tolerability profile
- Have significantly changed the landscape of preventive treatment
4.6 OnabotulinumtoxinA (Botox)
- FDA-approved for chronic migraine only (≥15 headache days/month)
- Placebo-controlled trials in episodic migraine were negative
- Injected into pericranial and neck muscles every 12 weeks
4.7 Other Agents
- Candesartan (ARB): shows preventive efficacy; well-tolerated
- Cyproheptadine: significant 5-HT antagonism; used especially in children
- Melatonin: controlled trial evidence; not FDA-approved for this indication
- Phenelzine (MAOI): reserved for very refractory cases; tyramine-containing foods contraindicated
5. Medication-Overuse Headache (MOH)
- Acute medications, especially opioids and barbiturate-containing analgesics, can aggravate headache frequency
- Results in refractory daily or near-daily headache (transformation of migraine)
- Patients with ≥2 headache days/week should be counseled about frequent analgesic use
- MOH is not a separate entity — it reflects migraine biology's reaction to certain medications
6. Special Situations
Menstrual Migraine (Catamenial Migraine)
- In ~15% of female migraineurs, attacks are exclusively perimenstrual
- Related to estrogen withdrawal (though hormonal influence is complex)
- Frovatriptan (longest-acting triptan, t½ >24 h) is particularly useful for perimenstrual prophylaxis
Migraine in Pregnancy
- Migraine tends to improve in 2nd and 3rd trimester in 75–80% of women
- Topiramate and valproate are contraindicated in pregnancy
- DHE is contraindicated in pregnancy
- NSAIDs generally avoided in 3rd trimester
Migraine with Cardiovascular Risk Factors
- Triptans require cardiac evaluation before use in patients with CAD risk
- Lasmiditan is preferred as it causes no vasoconstriction
- Gepants are also an option (no vasoconstriction)
7. Summary Table: Acute Treatment
| Drug Class | Mechanism | Use Case | Key Caution |
|---|---|---|---|
| Triptans | 5-HT1B/1D agonist | First-line, moderate–severe | CVD contraindication; no ergots within 24 h |
| Ergotamine/DHE | 5-HT1/α/DA agonist | Severe/refractory | CVD, pregnancy, CYP3A4 inhibitors |
| Lasmiditan | 5-HT1F agonist | Triptan-intolerant/CVD | Controlled substance; driving impairment |
| Gepants (ubrogepant, rimegepant) | CGRP receptor antagonist | Triptan-intolerant; also prevention | CYP3A4 interaction |
| NSAIDs | COX inhibition | Mild–moderate; adjunct | GI side effects |
| Antiemetics (metoclopramide, prochlorperazine) | DA antagonist | Adjunct; restore GI motility | Extrapyramidal effects |
| Opioids | μ-receptor agonist | Last resort | Dependency; MOH risk |
8. Summary Table: Prophylactic Treatment
| Drug Class | Examples | Notes |
|---|---|---|
| β-Blockers (1st line) | Propranolol, metoprolol | Avoid in asthma |
| Tricyclics | Amitriptyline, nortriptyline | Helpful with comorbid insomnia/depression |
| SNRI | Venlafaxine | Alternative antidepressant |
| Anticonvulsants | Topiramate, valproate | Avoid valproate in reproductive-age women |
| CCB | Verapamil | Second-line |
| CGRP mAbs | Erenumab, fremanezumab, galcanezumab, eptinezumab | Rapid onset, excellent tolerance; game-changer |
| Gepants | Rimegepant, atogepant | Oral; dual acute + prophylactic (rimegepant) |
| Botulinum toxin A | OnabotulinumtoxinA | Chronic migraine only |
| Others | Candesartan, cyproheptadine, melatonin | Off-label but evidence-based |
Sources:
- Lippincott Illustrated Reviews: Pharmacology — Ch. 39
- Goodman & Gilman's Pharmacological Basis of Therapeutics — Ch. 5 (5-HT drugs)
- Harrison's Principles of Internal Medicine 22e — Ch. 441
- Adams and Victor's Principles of Neurology, 12e — Ch. on Headache
- Katzung's Basic and Clinical Pharmacology, 16e — CGRP section
This is a shared conversation. Sign in to Orris to start your own chat.