Examination documentation of both bone fracture tibia and fibula of leg in orthopedic
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have thorough content from multiple authoritative textbooks. Let me compose the comprehensive examination documentation.
Examination Documentation: Fractures of the Tibia and Fibula (Leg)
Sources: Rockwood and Green's Fractures in Adults (10th ed., 2025), Rosen's Emergency Medicine (9th ed.), S. Das Manual on Clinical Surgery (13th ed.)
1. History
A thorough history is the foundation of examination. Key points to document:
- Mechanism of injury - high vs. low energy, direct blow, rotational stress, fall, motor vehicle collision
- Time of injury - delays affect management of open fractures and vascular injuries
- Onset and quality of pain - sharp, diffuse, progressive
- Neurological symptoms - numbness, tingling, paresthesias in the foot
- Prior injury/surgery/infection in the affected limb
- Comorbidities - diabetes (neuropathy), peripheral vascular disease, osteoporosis, malignancy, spinal radiculopathy
- Polytrauma screen - in high-energy mechanisms, document associated injuries to vital organ systems
2. Inspection
General Limb Appearance
- Deformity - angulation (varus/valgus/anterior/posterior), rotational malalignment, shortening
- Swelling and bruising - extent, distribution, rapid progression (suggests significant soft tissue injury)
- Skin integrity - any wound on a fractured limb must be assumed to communicate with the fracture until proven otherwise (open fracture)
Skin Compromise
- Skin tenting or puckering must be identified and documented immediately. If untreated, full-thickness skin necrosis can occur within hours, potentially converting a closed to an open fracture under a cast or splint without being noticed.
- Open lateral and posterolateral leg wounds are often associated with a fibula fracture, which may be at a different anatomic level than the tibia fracture.
Ankle Deformity
- Lateral displacement of the foot relative to the tibia suggests distal fibula/malleolar involvement
- Excessive broadening of the ankle suggests inferior tibiofibular diastasis (inferior tibiofibular ligament torn, with the talus wedged between tibia and fibula)
3. Palpation
Bony Palpation (Document at Each Level)
- Tibia shaft - palpate the full anteromedial border from tibial plateau to medial malleolus; note point of maximum tenderness, bony irregularity, step-off, or crepitus
- Fibula shaft - palpate from fibular head to lateral malleolus; note tenderness, deformity, mobility
- Tibial plateau - palpate medial and lateral condyles for tenderness (exclude plateau fracture)
- Fibular head and proximal fibula - tenderness here may indicate a Maisonneuve fracture (proximal fibular fracture with ankle mortise disruption); the entire fibula length must be palpated in any ankle injury
- Medial and lateral malleoli - palpate both, as a malleolar fracture can coexist with a shaft fracture
- Inferior tibiofibular joint - tenderness suggests syndesmotic disruption
Spring Test / Fibula Compression Test
- Squeezing the proximal tibia and fibula together (midshaft compression) produces pain at the fracture site distally - a useful test for fibula shaft fractures.
Crepitus
- Audible or palpable crepitus at the fracture site; document location.
- Do not repeatedly elicit crepitus - it causes pain and further tissue injury.
Joint Palpation
- Knee - effusion, joint line tenderness, stability testing (ligament injury may coexist with tibia shaft fracture)
- Ankle - tenderness at the joint line, malleoli, syndesmosis
4. Neurovascular Examination
This is mandatory before and after any reduction or splinting.
Vascular Assessment
Document at each assessment:
- Popliteal, posterior tibial, and dorsalis pedis pulses - palpate and grade (0 = absent, 1 = diminished, 2 = normal)
- Capillary refill - normal <2 seconds; delayed suggests ischemia
- Skin color - pallor, cyanosis, mottling
- Skin temperature - compare both limbs
- Venous congestion/swelling - may indicate venous outflow obstruction
If pulses do not return after bony reduction, urgent investigation with CT angiography, conventional angiography, or arterial Doppler is required to exclude popliteal or tibial artery injury.
Neurological - Motor Assessment
Grade strength (MRC 0-5) for key muscles. Document limitation by pain explicitly:
| Muscle | Action Tested | Nerve |
|---|---|---|
| Tibialis anterior | Ankle dorsiflexion | Deep peroneal |
| Extensor hallucis longus | Great toe extension | Deep peroneal |
| Extensor digitorum longus | Toe extension | Deep peroneal |
| Peroneus longus/brevis | Ankle eversion | Superficial peroneal |
| Gastrocnemius/soleus | Ankle plantarflexion | Tibial nerve |
| Tibialis posterior | Foot inversion | Tibial nerve |
The peroneal nerve is particularly vulnerable - it wraps around the posterior aspect of the fibular head, and proximal fibula fractures (including Maisonneuve fractures) carry a risk of peroneal nerve injury. A neurovascular examination is mandatory for any proximal fibular fracture.
Neurological - Sensory Assessment
Test sensation in each territory with eyes closed (to eliminate visual cues):
| Territory | Nerve | Test Area |
|---|---|---|
| First dorsal interspace (web space) | Deep peroneal | Dorsum of foot between 1st and 2nd toes |
| Dorsum of foot | Superficial peroneal | Dorsal foot |
| Lateral ankle and heel | Sural nerve | Lateral hindfoot |
| Medial ankle | Saphenous nerve | Medial ankle |
| Plantar surface | Tibial nerve | Sole of foot |
Document each territory as: present/normal, present/diminished, or absent.
5. Compartment Syndrome Assessment
This is one of the most critical components of examination in tibial fractures. The four compartments of the leg must be assessed:
| Compartment | Contents | Test |
|---|---|---|
| Anterior | Tibialis anterior, EHL, EDL, anterior tibial artery, deep peroneal nerve | Passive plantarflexion for pain; test dorsiflexion strength |
| Lateral | Peroneus longus and brevis, superficial peroneal nerve | Passive inversion for pain; test eversion strength |
| Superficial posterior | Gastrocnemius, soleus, plantaris | Passive dorsiflexion for pain |
| Deep posterior | Tibialis posterior, posterior tibial artery | Passive toe/ankle dorsiflexion for pain; test inversion |
Classic Signs (Document Presence or Absence)
- Pain out of proportion to injury severity
- Pain on passive stretch of compartment muscles
- Paresthesias or loss of light touch in compartment's nerve territory
- Tense, woody, or indurated compartment on palpation
- Paralysis of muscles in affected compartments (late sign)
- Pulselessness - unusual; implies very high compartment pressure or concomitant vascular injury
Serial examinations are mandatory in borderline cases. Compartment pressure monitoring is an adjunct in sedated or obtunded patients, but false-positive rates are significant.
6. Radiographic Assessment
Standard Views
- AP and lateral radiographs of the tibia centered at the mid-diaphysis; ideally capturing the entire tibia length
- AP and lateral views of the knee - to assess tibial plateau, proximal tibiofibular joint, and detect lipohemarthrosis (fat-blood level on cross-table lateral = intra-articular fracture)
- AP, lateral, and mortise views of the ankle - to assess distal tibiofibular joint, malleoli, and ankle mortise
When to Add CT or MRI
- Spiral fracture of the distal tibia: CT of the ankle to exclude posterior malleolar fracture (commonly missed on plain films)
- Suspected intra-articular extension at knee or ankle
- Pathologic fracture concern (minimal-energy mechanism, prior malignancy, antecedent pain, irregular bone appearance)
- Equivocal plain films with high clinical suspicion
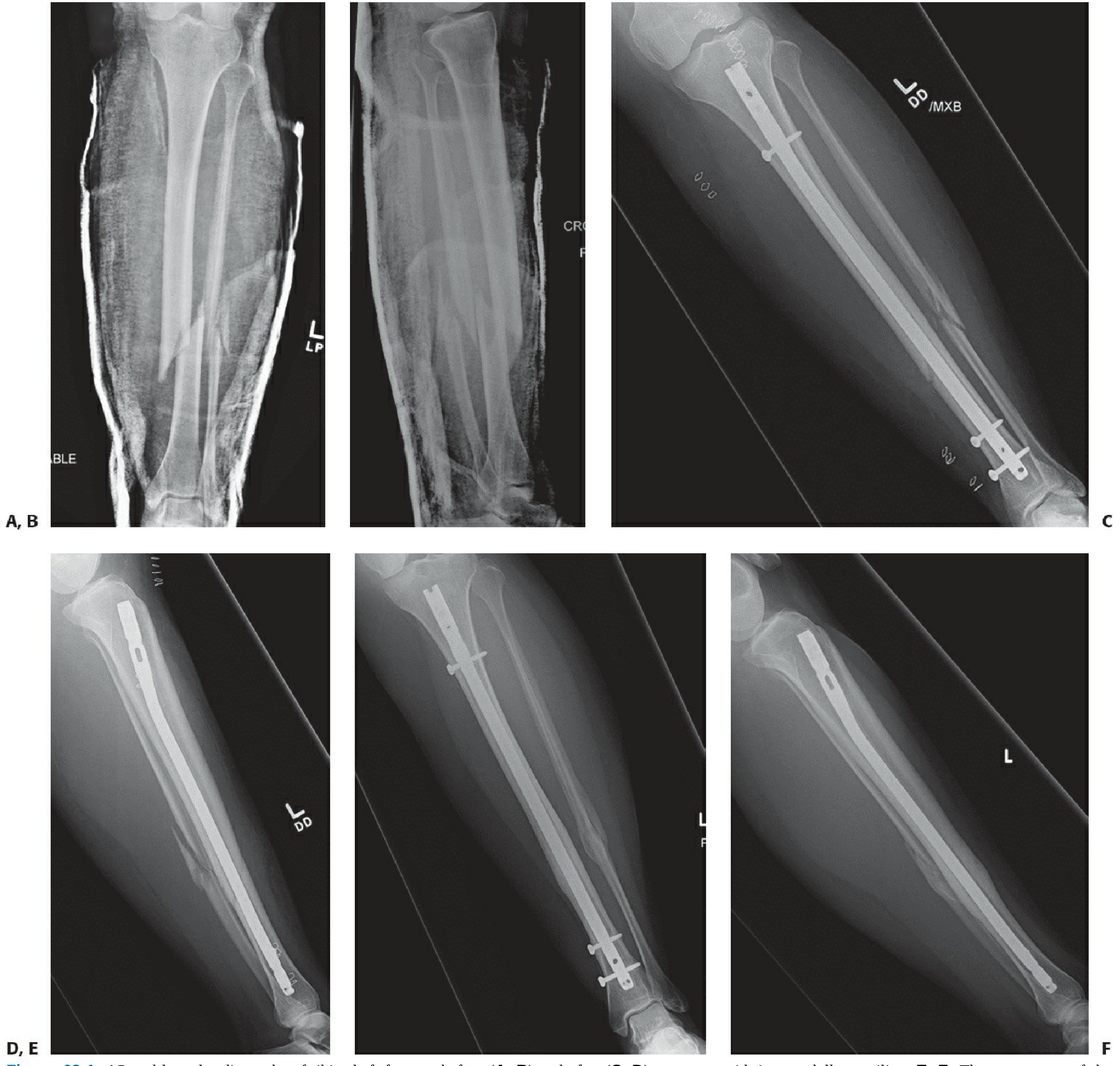
Figure: AP and lateral radiographs of a tibia shaft fracture before (A, B) and after (C, D) intramedullary nailing. Healed fracture at 12 months (E, F). - Rockwood and Green's Fractures in Adults, 10th ed.
7. Classification
OTA/AO Classification (Most Widely Used)
For tibia and fibula shaft fractures:
- Type A - Simple fracture (transverse, oblique, or spiral with two fragments)
- Type B - Wedge fracture (butterfly fragment, with maintained contact between main fragments)
- Type C - Complex/comminuted fracture (no contact between main fragments after reduction)
Each type is divided into subgroups of increasing severity (A1 < A2 < A3, etc.).
Open Fracture Classification (Gustilo-Anderson)
- Grade I - Clean wound <1 cm, minimal contamination
- Grade II - Wound 1-10 cm, moderate contamination, no extensive soft tissue damage
- Grade IIIA - Wound >10 cm with adequate soft tissue coverage
- Grade IIIB - Extensive soft tissue loss, periosteal stripping, requiring flap coverage
- Grade IIIC - Any open fracture with arterial injury requiring repair
8. Associated Injuries to Document
- Maisonneuve fracture - proximal fibula fracture with ankle syndesmotic disruption; always palpate the proximal fibula in ankle injuries
- Posterior malleolar fracture - particularly associated with distal-third spiral tibia fractures; may be invisible on plain films
- Proximal tibiofibular joint dislocation - occurs in ~1.5% of tibia shaft fractures (usually with intact fibula); associated with elevated risk of compartment syndrome (29%), open fracture (63%), and peroneal nerve injury (36%)
- Knee ligamentous injury - assess for medial/lateral collateral and cruciate instability
- Ipsilateral femur fracture ("floating knee")
9. Documentation Template Summary
| Category | What to Document |
|---|---|
| History | Mechanism, time, symptoms, past history, comorbidities |
| Inspection | Deformity, swelling, skin integrity, wound, ankle alignment |
| Palpation | Point tenderness (tibia/fibula full length), crepitus, malleoli, fibular head |
| Vascular | DP, PT pulses (pre/post reduction), cap refill, color, temp |
| Motor | Graded MRC 0-5 for dorsiflexors, plantarflexors, evertors, invertors |
| Sensory | Deep/superficial peroneal, tibial, sural, saphenous territories |
| Compartments | All 4 compartments - pain on stretch, tenseness, paresthesias |
| Radiology | AP/lateral tibia, knee, ankle views; CT/MRI when indicated |
| Classification | OTA/AO fracture type; Gustilo-Anderson if open |
| Associated injuries | Maisonneuve, posterior malleolus, PTF dislocation |
References:
- Rockwood and Green's Fractures in Adults, 10th ed. (2025) - Chapter 63, Signs and Symptoms, pp. 3167-3169
- Rosen's Emergency Medicine: Concepts and Clinical Practice - Chapter 48, Leg Injuries
- S. Das, A Manual on Clinical Surgery, 13th ed. - Examination of Injuries About the Ankle and Foot, p. 199
This is a shared conversation. Sign in to Orris to start your own chat.