subacute combined degeneration notes
Reading File
Finding Sources
Searching PubMed
"subacute combined degeneration" AND "vitamin B12"
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the complete notes.
Subacute Combined Degeneration (SCD)
Subacute combined degeneration (SCD) is a progressive, potentially reversible myelopathy caused primarily by vitamin B12 (cobalamin) deficiency. The word "combined" refers to the simultaneous involvement of the posterior (dorsal) columns AND lateral (corticospinal) columns of the spinal cord - hence the name.
Biochemistry and Mechanism
Cobalamin is essential for two enzymatic reactions:
-
Methylmalonyl-CoA → Succinyl-CoA (requires adenosylcobalamin)
- Deficiency leads to accumulation of methylmalonic acid (MMA)
- MMA may disrupt myelin synthesis by substituting abnormal fatty acids
-
Homocysteine → Methionine (requires methylcobalamin + methionine synthase)
- Methionine is converted to S-adenosylmethionine (SAM)
- SAM is the universal methyl donor for methylation reactions in the nervous system
- Without SAM, myelin maintenance fails
- Homocysteine accumulates (neurotoxic, also cardiovascular risk)
The net effect is demyelination followed by axonal degeneration, predominantly in the white matter of the spinal cord.
- Bradley & Daroff's Neurology in Clinical Practice, p. 1796
Causes of Vitamin B12 Deficiency
| Category | Examples |
|---|---|
| Autoimmune | Pernicious anemia (most common) - anti-parietal cell / anti-intrinsic factor antibodies |
| Dietary | Strict veganism (animal products are the only dietary source) |
| Post-surgical | Gastrectomy, bariatric surgery, ileal resection |
| GI disease | Crohn's disease, atrophic gastritis, blind-loop syndrome |
| Pharmacologic | Nitrous oxide (N2O) abuse - irreversibly inhibits B12-dependent enzymes; metformin (rare) |
| Infection | Fish tapeworm (Diphyllobothrium) |
| Other | AIDS, oral contraceptives, pregnancy (relative deficiency), multiple myeloma |
Important: Body stores (mainly in liver) are large - it typically takes 3-5 years after stopping absorption before deficiency becomes symptomatic.
- Bradley & Daroff's Neurology, p. 1798; Harrison's 22E, p. 1903
Pathology
The histological hallmark is spongiform vacuolation with foci of myelin and axon destruction in the white matter of the spinal cord.
Distribution (most → least affected):
- Posterior (dorsal) columns at cervical and upper thoracic levels - most severely affected
- Lateral columns (corticospinal tracts)
- Anterior columns - only in advanced disease
Peripheral nerves: predominantly axonal degeneration, sometimes demyelination.
Also involves: optic nerves and cerebral white matter in advanced cases.

SCD of the spinal cord: Demyelination and axon loss are more widespread in posterior than lateral columns (Weigert stain). - Bradley & Daroff's Neurology, Fig. 85.2
- Bradley & Daroff's Neurology, p. 535
Clinical Features
The onset is subacute (weeks to months). Signs are generally symmetric and reflect posterior + lateral column dysfunction.
Symptoms (roughly in order of onset):
Early:
- Paresthesias (tingling, numbness) in hands and feet - often the first symptom
- Loss of vibration sense and proprioception (posterior column)
- Lhermitte's sign may occur
As disease progresses:
- Progressive spastic weakness (lateral column / corticospinal)
- Sensory ataxia → positive Romberg sign
- Loss of reflexes (from peripheral neuropathy) + Babinski signs (from corticospinal involvement) - this coexistence is a classic diagnostic clue
Advanced:
- Optic atrophy
- Cognitive changes - irritability, memory impairment, dementia
- Cerebral white matter involvement
Mnemonic: The myelopathy is diffuse, not focal; symmetric, not unilateral.
- Harrison's 22E, p. 1903; Bradley & Daroff's Neurology, p. 1274
Diagnosis
Blood Tests
| Test | Finding | Notes |
|---|---|---|
| Serum B12 | Low (<200 pg/mL typical) | Can be normal in up to 30% of symptomatic patients |
| Methylmalonic acid (MMA) | Elevated | More sensitive and specific than B12 level alone |
| Homocysteine | Elevated | Also elevated in folate deficiency |
| CBC/peripheral smear | Macrocytic anemia, hypersegmented neutrophils | May be absent if concurrent iron deficiency |
| Anti-intrinsic factor antibodies | Positive in pernicious anemia | Highly specific |
| Anti-parietal cell antibodies | Positive in pernicious anemia | Less specific |
Key point: Hematological abnormalities may be absent at neurological presentation - do NOT rely on anemia alone to rule in/out.
Folic acid can correct the anemia without treating the neurological damage - if folate is given without B12 in a B12-deficient patient, neurological deterioration continues.
- Goldman-Cecil Medicine, p. 3681; Bradley & Daroff's Neurology, p. 938
Neurophysiology
- Nerve conduction studies: small or absent sural nerve sensory potentials (axonal polyneuropathy) in ~50% of patients
- Somatosensory and visual evoked responses: nonspecific abnormalities
- EEG: nonspecific
MRI Spinal Cord
The classic MRI finding is:
-
T2 hyperintensity in the dorsal columns, sometimes also lateral columns
-
Lesions most often at C2-C5 level, bilateral and symmetric
-
Described as an "inverted V" or linear hyperintensity on axial T2
-
T1: may show hypointensity in dorsal columns ± mild cord enlargement
-
Gadolinium enhancement: variable (some series show enhancement, others do not)
-
MRI may be normal - a negative MRI does not exclude SCD
-
Grainger & Allison's Diagnostic Radiology, p. 215; Bradley & Daroff's Neurology, p. 530
Closely Related Conditions
1. Nitrous Oxide (N2O) Myelopathy
- N2O irreversibly oxidizes Co(I) to Co(III) in cobalamin, permanently inactivating methionine synthase
- Produces a myelopathy identical to SCD
- Can occur after a single prolonged anesthetic exposure, especially in patients with marginal B12 stores
- Also from recreational abuse ("whippets")
- Prevention: B12 injections weeks before elective N2O anesthesia in at-risk patients
2. Copper Deficiency Myelopathy
- Clinically and radiologically indistinguishable from SCD but serum B12 is normal
- Low serum copper and ceruloplasmin
- Causes: post-bariatric surgery, excess zinc (supplements, denture creams) - zinc induces metallothionein which sequesters copper
- Treatment: oral copper supplementation 2 mg/day
3. Folate Deficiency Myelopathy
-
Similar but milder than SCD; rarely seen since dietary fortification programs
-
Always exclude B12 deficiency before treating with folate alone
-
Harrison's 22E, p. 1904-1905; Bradley & Daroff's Neurology, p. 535
Treatment
Vitamin B12 (cobalamin) replacement - standard IM regimen:
- 1000 µg IM daily x 5-7 days
- Then 1000 µg IM weekly x 4-8 weeks (1 month)
- Then 1000 µg IM monthly (lifelong maintenance for pernicious anemia)
Oral alternative (for maintenance):
- High-dose cyanocobalamin 1-2 mg orally daily - even in pernicious anemia, passive diffusion (1-5%) absorbs enough at this dose
- Suitable for maintenance once neurological stabilization achieved; requires monitoring
Response to treatment:
-
Serum MMA and homocysteine normalize within ~2 weeks
-
Neurological improvement is delayed and may be incomplete
-
Most symptomatic improvement occurs in the first 6-12 months
-
Prognosis correlates inversely with duration of symptoms before treatment - early diagnosis is key
-
If symptoms progress despite normalized B12, consider copper deficiency
-
Harrison's 22E, p. 1903; Bradley & Daroff's Neurology, p. 547
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| MS myelopathy | Asymmetric, relapsing-remitting, lesions on MRI, younger patient |
| Tabes dorsalis (neurosyphilis) | Lancinating pains, Argyll Robertson pupil, positive syphilis serology |
| Friedreich's ataxia | Autosomal recessive, cardiomyopathy, genetic testing |
| HTLV-1 myelopathy | Tropical spastic paraparesis, positive HTLV-1 serology |
| Copper deficiency myelopathy | Identical to SCD, normal B12, low serum copper |
| HIV myelopathy | Vacuolar myelopathy, positive HIV serology |
| Adrenomyeloneuropathy | Elevated very long chain fatty acids, adrenal involvement |
Summary
| Feature | Detail |
|---|---|
| Primary cause | Vitamin B12 (cobalamin) deficiency |
| Columns affected | Posterior (dorsal) > Lateral > Anterior |
| Classic triad | Peripheral neuropathy + posterior column loss + corticospinal signs |
| Diagnostic clue | Areflexia + Babinski sign in the same patient |
| Key labs | ↓ B12, ↑ MMA, ↑ homocysteine, macrocytic anemia |
| MRI finding | T2 hyperintensity bilateral dorsal columns ("inverted V"), C2-C5 |
| Treatment | IM B12 1000 µg - daily → weekly → monthly |
| Nitrous oxide | Irreversible B12 inactivation, identical syndrome |
| Copper deficiency | Same picture, normal B12, low copper |
Recent literature (2024-2025):
- A 2024 review (Holroyd & Berkowitz, Continuum) covers metabolic myelopathies including SCD with updated diagnostic approach.
- A 2025 comprehensive review (Bernetti et al., Brain Sci) specifically addresses SCD MRI diagnostic challenges and treatment pathways.
- Recreational nitrous oxide misuse as a cause of SCD is an increasing clinical concern, highlighted in a 2025 review (PMID 40901226).
Sources: Harrison's Principles of Internal Medicine 22E (2025); Bradley & Daroff's Neurology in Clinical Practice; Grainger & Allison's Diagnostic Radiology; Goldman-Cecil Medicine
Describe clinical presentation and Physiotherapy Management in Radial Nerve injury
Reading File
Finding Sources
Finding Sources
Searching PubMed
"radial nerve" AND "rehabilitation" AND "peripheral nerve injury"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
I have comprehensive content from multiple authoritative textbooks. Let me now compile the full notes.
Radial Nerve Injury - Clinical Presentation & Physiotherapy Management
Anatomy Recap (Clinically Relevant)
The radial nerve (C5-C8, T1) is the largest branch of the posterior cord of the brachial plexus. It passes through the triangular interval, winds around the posterior humerus in the spiral (radial) groove, then pierces the lateral intermuscular septum at the junction of the middle and distal thirds of the arm. It divides near the elbow into:
- Superficial branch (purely sensory) - dorsum of hand and digits
- Deep branch / Posterior Interosseous Nerve (PIN) - enters the supinator canal, supplies all extensor muscles of the forearm
The radial nerve is the most frequently injured nerve in the upper limb due to its intimate relationship with the humeral shaft.
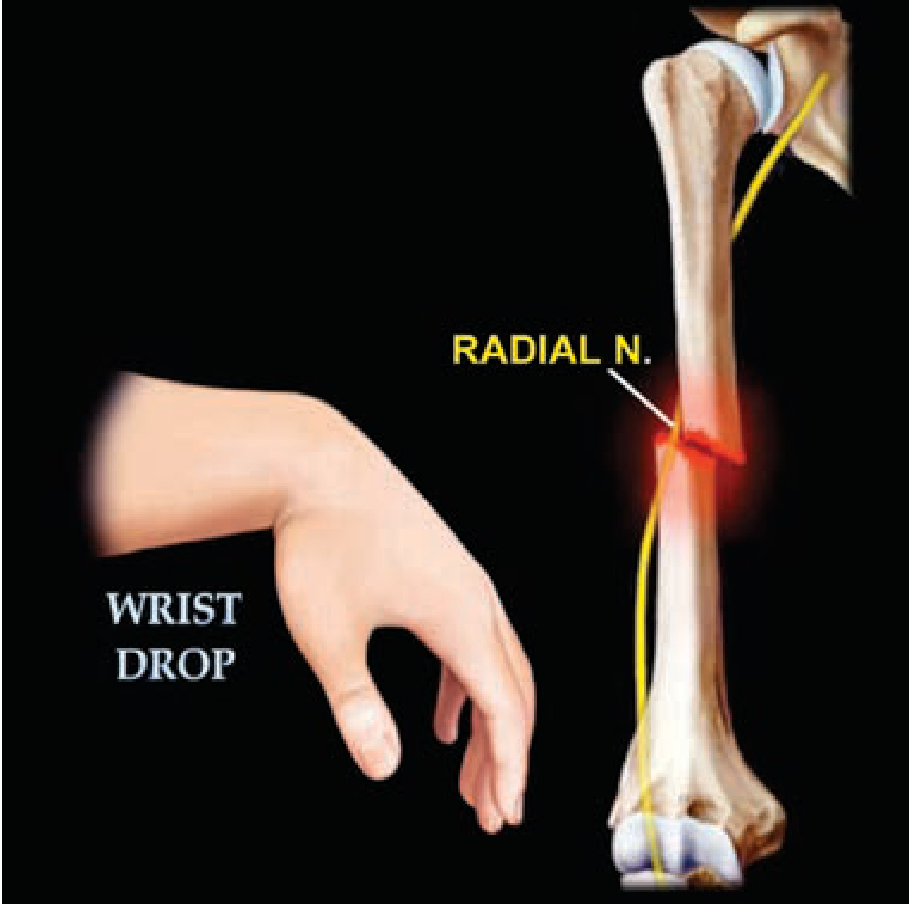
Radial nerve injury at the spiral groove causing wrist drop - Schwartz's Principles of Surgery
Causes by Level
| Level | Common Causes |
|---|---|
| Axilla | Crutch palsy ("crutch paralysis"), humeral head dislocation, pressure from axillary crutches |
| Spiral groove (mid-humerus) | Humeral shaft fracture (~11-22% of cases), "Saturday night palsy" / "park bench palsy" (prolonged arm-over-chair compression), tourniquet, deep IM injection |
| Lateral intermuscular septum | Distal 1/3 humeral fracture, fibrous band compression |
| Radial tunnel / elbow | Radial tunnel syndrome, dislocation of radial head (Monteggia fracture-dislocation), lateral epicondylitis surgery |
| Posterior interosseous nerve (PIN) | Supinator muscle entrapment (supinator syndrome), radius fracture, lipoma, ganglion |
| Superficial branch (Wartenberg's) | Wristwatch/bracelet compression, handcuffs ("handcuff neuropathy"), de Quervain's surgery |
- Thieme Atlas of Anatomy, p. 388-389; Rockwood & Green's Fractures 10th Ed 2025, p. 789
Clinical Presentation by Level of Injury
1. High Radial Nerve Injury (Axilla)
Motor loss:
- Triceps (elbow extension) - weak/paralysed
- Brachioradialis
- All wrist extensors (ECRL, ECRB, ECU)
- Finger extensors (EDC, EI, EDM)
- Thumb extensors and abductor (EPL, EPB, APL)
Sensory loss:
- Posterior cutaneous nerve of arm (dorsum of arm)
- Posterior cutaneous nerve of forearm
- Superficial radial nerve territory: dorsum of hand (radial 3½ digits), first dorsal web space (most consistent/exclusive area)
Signs: Wrist drop + loss of triceps reflex + elbow flexion weakness (brachioradialis)
2. Spiral Groove (Most Common) - Mid-Humeral Injury
Motor loss:
- Triceps spared (branches to triceps leave before the groove)
- Brachioradialis weak/paralysed
- All wrist and finger extensors paralysed
- Thumb extensors/abductor paralysed
Sensory loss:
- Dorsum of hand and digits (superficial branch territory)
- Posterior cutaneous nerve of arm spared (branches before groove)
Signs: Classic wrist drop + absent brachioradialis reflex; triceps reflex intact
Diagnostic tip: Test brachioradialis (forearm in mid-prone position, flex elbow against resistance - muscle stands out). If brachioradialis is intact, injury is below the spiral groove.
3. Posterior Interosseous Nerve (PIN) / Distal Injury
Motor loss:
- Wrist extension partially preserved (ECRL and ECRB supplied before PIN enters supinator)
- Finger extension at MCP joints lost (EDC, EI, EDM)
- Thumb extension and abduction lost (EPL, EPB, APL)
- No wrist drop (wrist can extend, but deviates radially due to preserved ECRL/ECRB)
Sensory loss: None (superficial branch already separated before supinator canal)
4. Superficial Radial Nerve (Wartenberg's Syndrome)
Motor: None
Sensory: Burning pain, paresthesia, numbness over dorsal radial aspect of hand and first dorsal web space only
Hallmark Sign: Wrist Drop
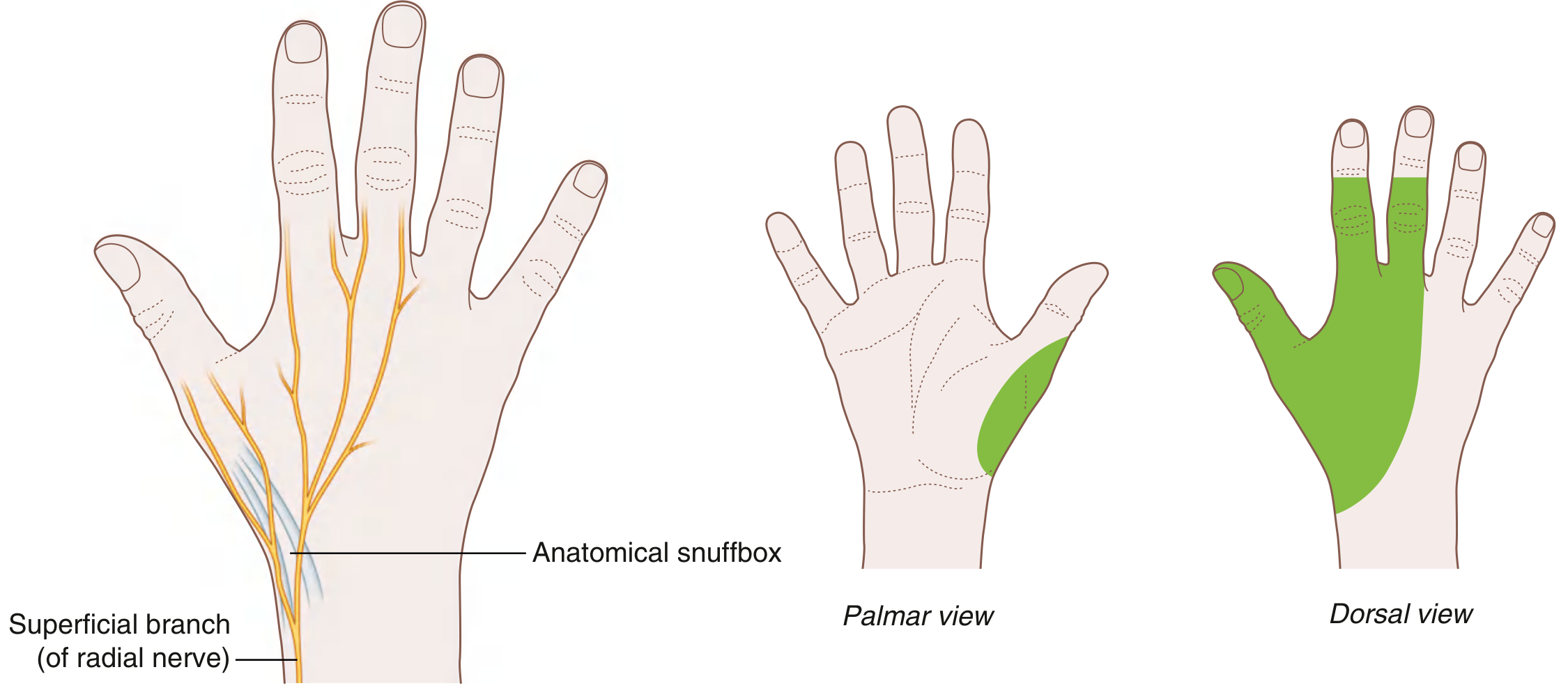
Radial nerve distribution in the hand - Gray's Anatomy for Students
-
Inability to actively extend the wrist (hangs in flexion)
-
Inability to extend MCPJs of fingers (can extend IPJs via interossei - ulnar nerve)
-
Inability to extend/abduct thumb (EPL, EPB, APL)
-
Key clinical pearl: IP joint extension via the interossei (ulnar nerve) remains intact - do NOT mistake this for nerve recovery
-
S. Das Manual on Clinical Surgery 13th Ed; Thieme Atlas, p. 387
Investigations
| Investigation | Purpose |
|---|---|
| Clinical examination | Level of injury, Tinel's sign progression |
| EMG/NCS | Confirm diagnosis, degree of axonal loss vs. neurapraxia, prognostication |
| Nerve ultrasound | Detect nerve continuity, entrapment, neuroma in continuity |
| X-ray / CT | Associated humeral fracture |
| MRI | Soft tissue masses, nerve visualization |
EMG timing protocol:
-
If no clinical recovery at 3 weeks: perform EMG/NCS
-
Repeat at 3 months if no recovery
-
At 6 months without recovery: consider surgical exploration
-
Harrison's 22E, p. 999; Campbell's Operative Orthopaedics 15th Ed 2026
Natural History and Prognosis
Most radial nerve injuries (spiral groove) are neurapraxia or axonotmesis - not neurotmesis.
-
Spontaneous recovery: 70% or more of cases
-
Mean time to onset of recovery: 7 weeks (range 2 weeks to 6 months)
-
Mean time to full recovery: 6 months (range 3-12 months)
-
Transection (neurotmesis) is rare - mainly with open fractures
-
Rockwood & Green's Fractures, p. 789-790
Physiotherapy Management
Physiotherapy is central to both the waiting/recovery phase (conservative) and post-surgical recovery. Management is staged.
Phase 1: Acute / Early Phase (0-6 weeks)
Goals: Prevent deformity, maintain joint mobility, prevent oedema, protect the nerve, educate patient
1. Splinting (Orthotic Management)
- Cock-up wrist splint (wrist extension splint, 20-30° extension): the primary splint. Prevents wrist flexion contracture, maintains functional position for grip
- Dynamic extension splint (lively splint): allows passive wrist/finger flexion with active elastic-assisted extension - preferred for daytime functional use as it enables some hand function
- Splint worn most of the day; removed for exercise sessions
Harrison's 22E: "Treatment consists of cock-up wrist and finger splints, avoiding further compression, and physical therapy to avoid flexion contracture."
2. Passive Range of Motion (PROM) Exercises
- Daily passive mobilisation of all joints in the affected limb:
- Wrist: flexion/extension/deviation
- MCP and IP joints of fingers
- Thumb CMC, MCP, IP joints
- Elbow and shoulder
- Goal: prevent flexion contractures and maintain full joint range
- 2-3 times daily, 10-20 repetitions each
3. Oedema Management
- Elevation of the limb
- Retrograde massage
- Compression bandaging if oedema present
4. Sensory Protection and Education
- Educate patient to avoid heat, pressure, trauma to anaesthetic skin
- Avoid tight watch straps, jewellery, sleeping on the arm
- Regular skin inspection
5. Maintain Proximal Strength
- Active exercises for unaffected muscles (shoulder, elbow flexion/pronation-supination)
- Prevent disuse atrophy of proximal muscles
Phase 2: Recovery Phase (6 weeks - 6 months)
Goals: Facilitate nerve regeneration, begin active muscle re-education, restore function
1. Monitor Recovery
- Track Tinel's sign progression distally along the nerve course (sign of axonal regeneration)
- Serial manual muscle testing (MRC grading)
- Re-check EMG at 3 months if no improvement
2. Active Assisted and Active Exercises
- As soon as any active wrist/finger extension returns (MRC grade ≥2):
- Active-assisted wrist extension
- Active extension of MCPJs
- Thumb extension and abduction
- Progress from gravity-eliminated positions → gravity-resisted positions
- Use mirror therapy or biofeedback to facilitate motor re-education
3. Muscle Re-education Techniques
- Facilitation techniques: tapping, vibration, quick stretch over wrist extensors
- Proprioceptive Neuromuscular Facilitation (PNF): patterns involving radial extensors (e.g., D2 extension pattern)
- Electrical stimulation / Neuromuscular electrical stimulation (NMES/FES): applied to wrist and finger extensors to maintain muscle bulk, prevent atrophy, and facilitate re-education of recovering muscles
- EMG biofeedback: visual/auditory feedback of muscle activity to reinforce voluntary effort
4. Strengthening Exercises
- Progressive resistive exercises for extensors as grades improve
- Theraband / putty exercises for wrist extension
- Grip strengthening (flexors work against gravity with wrist supported)
5. Sensory Re-education
- Once sensation starts recovering:
- Desensitisation (textures, vibration, temperature discrimination)
- Sensory discrimination training (moving vs. static two-point discrimination)
- Progression from coarse to fine textured materials
Phase 3: Functional Rehabilitation (3-12 months)
Goals: Restore full grip, pinch, fine motor function; return to occupation and daily activities
1. Functional Task Training
- Activities of daily living (ADL) training: writing, dressing, food preparation
- Occupational tasks relevant to the patient's work
- Progressive difficulty of task demands
2. Strengthening and Endurance
- Resistive wrist extension with free weights, Theraband
- Finger extension exercises against resistance
- Grip and pinch strengthening (dynamometer-guided)
3. Coordination and Dexterity
- Pegboard exercises, manipulation of small objects
- Fine motor tasks: buttoning, picking up coins
4. Work/Sport-Specific Rehabilitation
- Simulate occupational demands
- Return-to-sport conditioning as appropriate
Electrotherapy Modalities
| Modality | Role |
|---|---|
| NMES / FES | Prevent denervation atrophy, facilitate muscle re-education |
| TENS | Pain and dysaesthesia management |
| Ultrasound therapy | Promote nerve healing (some evidence for pulsed ultrasound in nerve regeneration) |
| Low-level laser therapy (LLLT) | May accelerate nerve regeneration |
| Shortwave / PEMF | Reduce pain and oedema (acute phase) |
| Interferential therapy | Pain management, muscle stimulation |
Indications for Surgical Referral (from Physiotherapy Perspective)
Refer if:
- No clinical improvement (Tinel's sign not advancing) after 6-8 weeks of conservative management
- EMG at 3 months shows no reinnervation
- Open fracture / penetrating injury (early exploration indicated)
- Evidence of nerve entrapment or rupture on ultrasound/MRI
- No functional recovery at 6 months
Surgical options include: neurolysis, nerve repair, nerve grafting, tendon transfers (especially if recovery fails - e.g., FCU→EDC transfer for finger extension).
- Rockwood & Green's Fractures 10th Ed 2025; Harrison's 22E, p. 999; Campbell's Operative Orthopaedics 15th Ed 2026
Summary Table: Physiotherapy by Phase
| Phase | Timeframe | Key PT Interventions |
|---|---|---|
| Acute | 0-6 weeks | Cock-up/dynamic splint, PROM, oedema management, sensory protection, proximal strengthening |
| Recovery | 6 weeks - 6 months | AROM/AAROM, muscle re-education, PNF, NMES, sensory re-education, Tinel monitoring |
| Functional | 3-12 months | Resistance training, ADL training, fine motor, work/sport rehab |
Differential Diagnoses for Wrist Drop
| Condition | Key Differentiator |
|---|---|
| C7 radiculopathy | Neck pain, triceps weakness, reflex changes at triceps |
| Posterior cord brachial plexopathy | Deltoid and teres minor also weak |
| Central lesion (stroke, etc.) | UMN signs, pyramidal pattern, no sensory dermatomal pattern |
| Lead poisoning | Bilateral wrist drop, brachioradialis often spared |
| PIN syndrome | No wrist drop, no sensory loss, radial deviation of wrist |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Gray's Anatomy for Students; Thieme Atlas of Anatomy; S. Das Manual on Clinical Surgery 13th Ed; Rockwood & Green's Fractures in Adults 10th Ed (2025); Campbell's Operative Orthopaedics 15th Ed (2026)
This is a shared conversation. Sign in to Orris to start your own chat.