Weakness
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have a comprehensive picture. Here is the full clinical overview of Weakness:
Weakness - Clinical Overview
What Is "Weakness"?
Patients use the term "weakness" to describe a broad spectrum of complaints - true motor weakness, fatigue, poor energy, dyspnea, or even depression. Clinically, it is important to distinguish true (objective) muscle weakness (loss of power confirmed on examination) from subjective weakness (asthenia, fatigue), as these have entirely different diagnostic implications.
Somewhat paradoxically, patients who complain of "weakness" often do not have confirmatory findings on examination. Conversely, even severe weakness may go unreported by patients. - Goldman-Cecil Medicine
Framework: Localization First
The single most important step in evaluating weakness is anatomic localization. The pattern of weakness and associated signs point to where in the nervous system (or outside it) the lesion lies.
1. Non-Neurological (Systemic) Causes
These should be considered first, especially in the ED setting where up to 10% of visits are for generalized weakness:
- Alterations in plasma volume (dehydration)
- Electrolyte imbalance (hypokalemia, hypophosphatemia)
- Anemia or polycythemia
- Decreased cardiac pump function (myocardial ischemia/HF)
- Decreased systemic vascular resistance (vasodilatory shock)
- Increased metabolic demand (infection, endocrinopathy, toxin)
- Mitochondrial dysfunction (severe sepsis)
- Global CNS depression (sedatives, stimulant withdrawal)
Over half of ED patients presenting with generalized weakness are found to have a serious underlying condition. - Rosen's Emergency Medicine
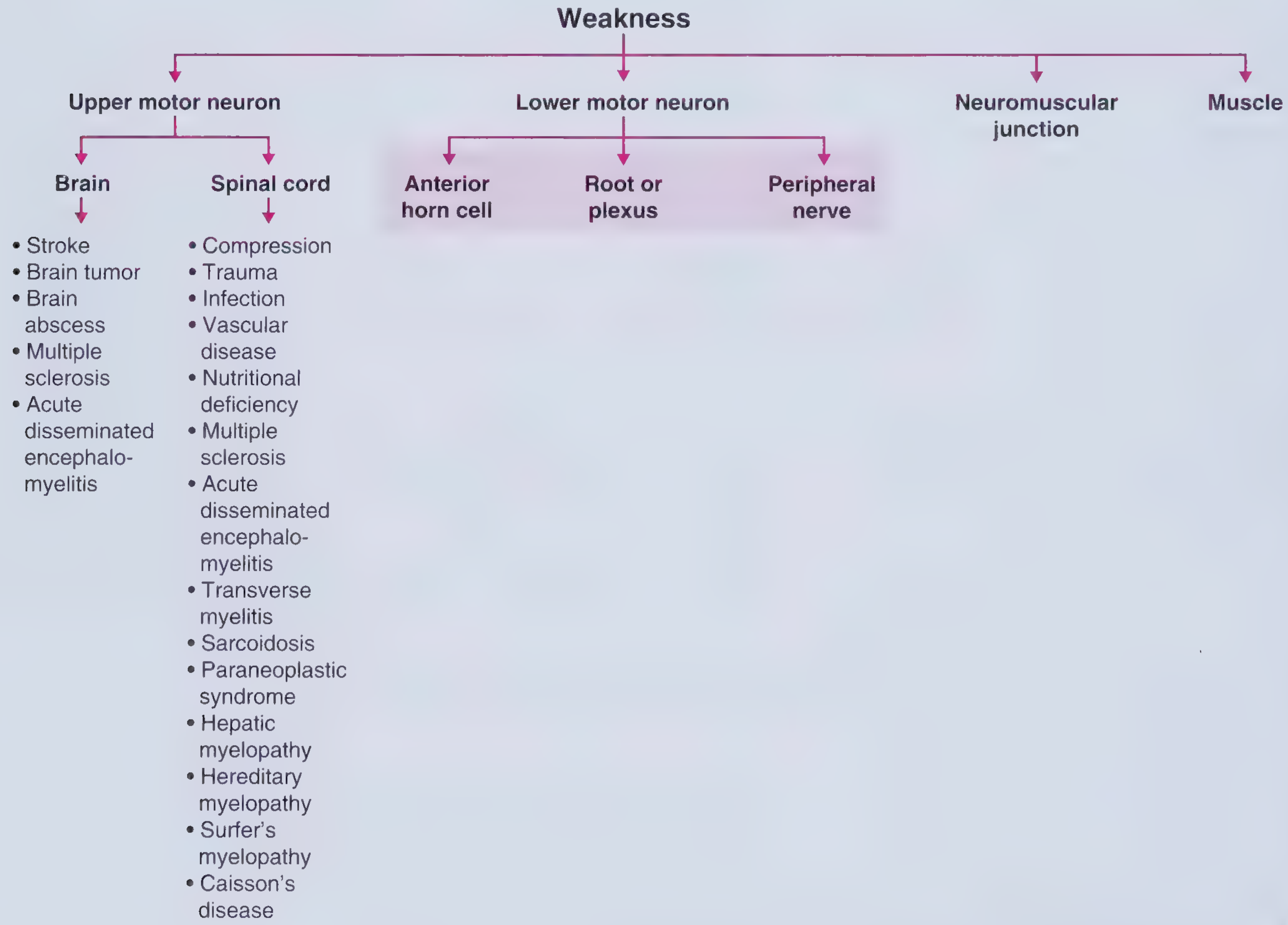
2. Upper Motor Neuron (UMN) Weakness
Lesion sites: Brain (cortex, subcortex) or spinal cord (corticospinal tract)
Signs:
- Spasticity - extension pattern in upper extremities, flexion in lower extremities
- Hyperreflexia
- Pronator drift
- Hoffman's sign, Babinski sign
- Weakness is typically contralateral to a brain lesion
Key causes by location:
| Brain | Spinal Cord |
|---|---|
| Stroke | Compression / trauma |
| Brain tumor | Transverse myelitis |
| Brain abscess | Multiple sclerosis |
| Multiple sclerosis | Paraneoplastic syndrome |
| ADEM | Nutritional deficiency |
3. Lower Motor Neuron (LMN) Weakness
LMN lesion sites: Anterior horn cell, nerve root or plexus, peripheral nerve
Signs:
- Flaccidity
- Decreased/absent reflexes
- Fasciculations
- Muscle atrophy
- Muscle cramps
Causes by sub-level:
| Anterior Horn Cell | Root/Plexus | Peripheral Nerve |
|---|---|---|
| ALS | Disc herniation (radiculopathy) | Guillain-Barre syndrome |
| Progressive muscular atrophy | Brachial/lumbosacral plexopathy | Charcot-Marie-Tooth |
| Poliomyelitis / post-polio | Thoracic outlet syndrome | Diabetic neuropathy |
| West Nile virus | Neoplastic invasion | Vasculitic neuropathy |
| Spinal muscular atrophy | Toxic/drug neuropathy |
4. Neuromuscular Junction (NMJ) Disorders
Present with fatigable weakness - weakness that worsens with sustained/repeated activity and improves with rest.
- Myasthenia gravis - autoantibodies against AChR (or MuSK); ptosis and diplopia are classic
- Lambert-Eaton myasthenic syndrome - usually paraneoplastic (small-cell lung cancer); proximal muscle weakness, reduced reflexes that transiently improve with exercise
- Botulism - descending flaccid paralysis, dilated pupils, dry mouth
5. Muscle (Myopathic) Weakness
Typically proximal and symmetric (difficulty rising from chair, climbing stairs, raising arms).
- Inflammatory myopathies: Polymyositis, dermatomyositis, inclusion body myositis
- Endocrine myopathies: Hypothyroid, hyperthyroid, Cushing's, Addison's
- Toxic/drug-induced: Statins (rare severe myopathy/rhabdomyolysis), steroids, alcohol
- Inherited: Duchenne/Becker MD, facioscapulohumeral MD, mitochondrial myopathies
- Metabolic: Glycogen storage diseases, periodic paralysis (channelopathy)
6. Special Pattern: Episodic/Intermittent Weakness
This pattern in a patient with normal baseline strength suggests:
- Channelopathy - periodic paralysis (hypo- or hyperkalemic)
- NMJ disorder - myasthenia gravis, Lambert-Eaton
- Narcolepsy - sleep paralysis
- Demyelinating disease - MS with heat-induced Uhthoff's phenomenon
Key UMN vs LMN Comparison
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Tone | Increased (spastic) | Decreased (flaccid) |
| Reflexes | Hyperreflexia | Hyporeflexia / absent |
| Atrophy | Mild (disuse only) | Marked |
| Fasciculations | Absent | Present |
| Babinski sign | Present (upgoing toe) | Absent |
| Distribution | Often hemibody / regional | More focal / segmental |
Diagnostic Approach Summary
- History - onset (acute vs. subacute vs. chronic), pattern (focal vs. generalized), progression, associated symptoms (sensory loss, pain, sphincter involvement), medications, family history
- Vital signs - fever, hypotension, bradycardia, tachycardia all suggest systemic cause
- Neurological exam - confirm and localize weakness (UMN vs. LMN pattern, cranial nerve involvement, sensory level)
- Targeted workup based on localization:
- Systemic: CBC, metabolic panel, TFTs, CRP/ESR, glucose
- CNS: MRI brain/spine
- Peripheral nerve/NMJ: EMG/nerve conduction studies
- Muscle: CK, aldolase, myositis panel; muscle biopsy if needed
- NMJ: acetylcholine receptor antibodies, repetitive nerve stimulation
Sources: Frameworks for Internal Medicine, p. 605-607; Goldman-Cecil Medicine; Rosen's Emergency Medicine, p. 130
This is a shared conversation. Sign in to Orris to start your own chat.