Cyanotic congenital heart disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cyanotic congenital heart disease" AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full, detailed response.
Cyanotic Congenital Heart Disease
Cyanotic congenital heart disease (CHD) refers to structural cardiac defects that result in right-to-left shunting of deoxygenated blood into the systemic circulation, causing hypoxemia and clinical cyanosis. The classic group is remembered by the "5 Ts": Tetralogy of Fallot, Transposition of the Great Arteries, Tricuspid Atresia, Truncus Arteriosus, and Total Anomalous Pulmonary Venous Return (TAPVR). All cause cyanosis through right-to-left shunting, though the underlying mechanisms differ.
Pathophysiology: Why Cyanosis Occurs
Right-to-left shunting bypasses the pulmonary circulation, allowing deoxygenated (venous) blood to enter the systemic arterial circulation. This produces:
- Hypoxemia (low PaO2)
- Central cyanosis (visible when reduced hemoglobin > 5 g/dL)
- Compensatory polycythemia (chronic hypoxemia stimulates erythropoiesis)
- Clubbing of fingers/toes (chronic hypoxemia)
The classification by pulmonary blood flow is clinically useful:
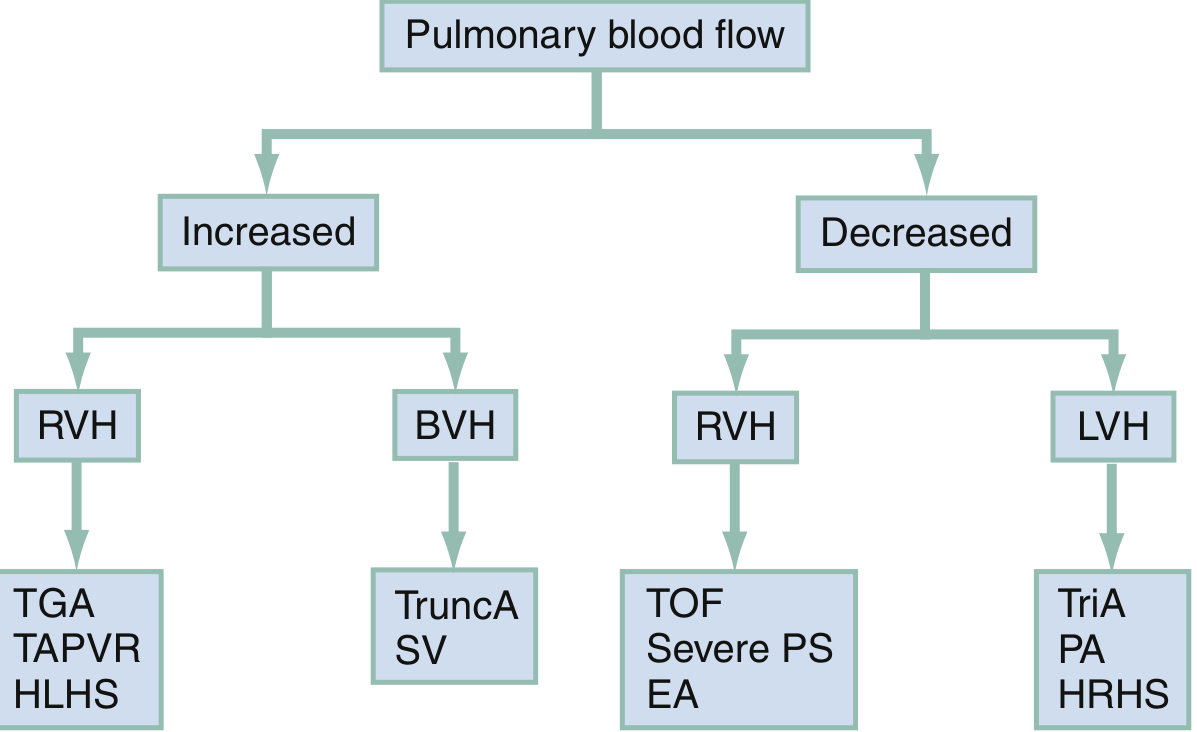
Fig. Clinical clues to diagnosis of cyanotic CHDs based on pulmonary blood flow and ECG findings (Rosen's Emergency Medicine)
The Five Classic Lesions
1. Tetralogy of Fallot (TOF)
Most common cyanotic CHD beyond infancy - ~1 in 2,500 live births.
Four anatomical defects (all arising from a single embryologic defect - anterosuperior displacement of the infundibular septum):
- Large, unrestrictive, misaligned VSD
- Right ventricular outflow tract obstruction (RVOTO) - subpulmonic stenosis
- Aorta overriding the VSD
- Right ventricular hypertrophy (secondary to pressure overload)
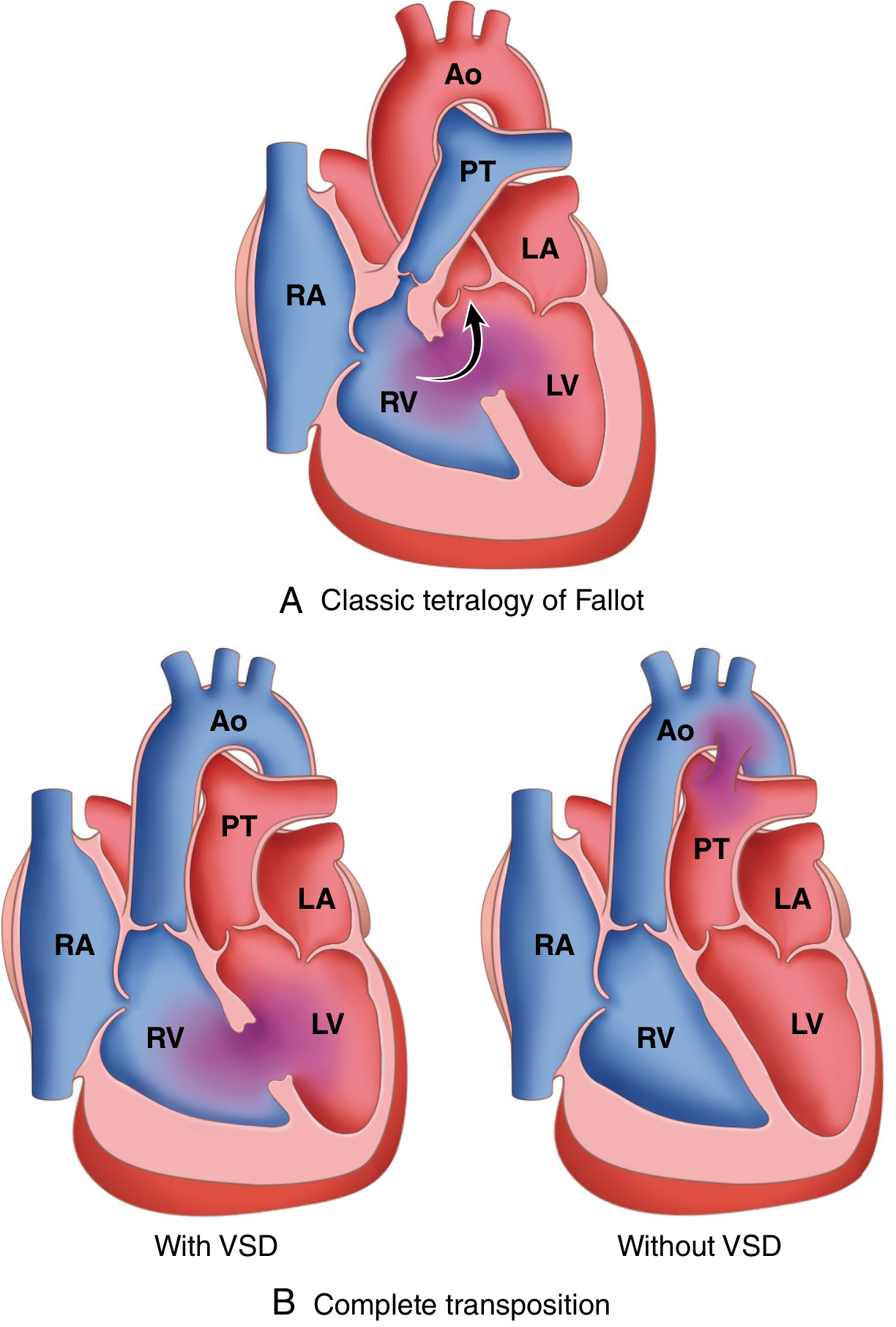
Fig. (A) Classic TOF: right-to-left VSD shunt when subpulmonic stenosis is severe. (B) Complete TGA: with and without VSD (Robbins Pathology)
Clinical presentation:
- Degree of cyanosis depends on severity of RVOTO
- Pink TOF: mild obstruction, may have left-to-right shunt initially
- Severe TOF: profound cyanosis from birth, requires PGE1 to maintain ductal patency
- Systolic ejection murmur at left sternal border
- Right axis deviation + RVH on ECG
- Boot-shaped heart on CXR (coeur en sabot) - concave pulmonary artery segment, normal heart size, decreased pulmonary vascular markings
- Right-sided aortic arch in ~25% of cases
Tet Spells (Hypercyanotic/Hypoxic Spells):
Peak incidence at 2-4 months. Triggered by anything that suddenly lowers SVR (crying, feeding, defecation, hypovolemia, tachycardia). The mechanism is a vicious cycle:
SVR falls → Increased R-to-L shunt across VSD → ↓PaO2, ↑PCO2, ↓pH → Hyperpnea → ↑Venous return to RV → ↑R-to-L shunting → Worsening cyanosis
Management of Tet Spells:
| Intervention | Mechanism |
|---|---|
| Knee-to-chest position | ↑SVR, ↓R-to-L shunt |
| Supplemental O2 | Limited benefit alone |
| Morphine 0.1-0.2 mg/kg IV/IM | Sedation, ↓hyperpnea, ↓SVR |
| Fentanyl 1 µg/kg IV/IM | Alternative to morphine |
| Propranolol IV | ↓Infundibular spasm (β-blockade) |
| Phenylephrine (α-agonist) | ↑SVR directly |
| IV fluids | Correct hypovolemia |
| NaHCO3 | Correct metabolic acidosis |
Surgical treatment:
- Definitive: VSD patch closure + RVOTO relief (transatrial/transpulmonary approach preferred to spare RV function)
- Palliative (if not ready for repair): Modified Blalock-Taussig shunt (subclavian-to-pulmonary artery anastomosis), pioneered in 1944 by Blalock, Taussig, and Vivien Thomas at Johns Hopkins
- Long-term sequelae include pulmonary regurgitation requiring pulmonary valve replacement in adulthood
2. Transposition of the Great Arteries (D-TGA)
2-3 per 10,000 live births. The aorta arises from the RV and the pulmonary artery from the LV - ventriculoarterial discordance with normal AV connection. This creates two parallel, independent circuits: systemic venous blood goes RV→Aorta→body (never oxygenated), and pulmonary venous blood goes LV→PA→lungs (never reaches body). Survival requires mixing between the two circuits via ASD, VSD, or PDA.
Clinical features:
- Extreme cyanosis from birth (especially with intact septum - TGA-IVS)
- Single, loud S2; minimal or no murmur (unless VSD/PS present)
- ECG: RAD and RVH (RV acts as systemic ventricle)
- CXR: "Egg on a string" - narrow mediastinum (parallel great vessels), cardiomegaly, increased pulmonary vascular markings
Management:
- PGE1 infusion - maintains ductal patency to improve mixing and pulmonary blood flow
- Balloon atrial septostomy (Rashkind procedure) - creates/enlarges ASD for atrial-level mixing, temporizes until surgery
- Arterial switch operation (Jatene procedure) - definitive repair; great arteries transected and switched back to the correct ventricles, coronary arteries reimplanted; must be performed within first 2 weeks of life before LV "de-trains" from the low-resistance pulmonary circuit
3. Tricuspid Atresia
Complete absence of the tricuspid valve with a hypoplastic RV and pulmonary artery. Requires ASD, PDA, or VSD to survive (to allow right heart blood to reach the lungs via left heart).
Features:
- Single S2 + systolic regurgitant murmur at LLSB if VSD present
- ECG: Superior QRS axis (distinguishes from other cyanotic CHDs) + LVH (LV is the dominant ventricle)
- CXR: Normal or slightly enlarged heart, may be boot-shaped
Management: Staged palliative surgeries toward Fontan circulation:
- Stage 1 (neonatal): BT shunt or PA banding depending on pulmonary flow
- Stage 2 (4-6 months): Bidirectional Glenn (SVC → pulmonary artery)
- Stage 3 (2-4 years): Fontan completion (IVC → pulmonary artery via extracardiac conduit)
4. Total Anomalous Pulmonary Venous Return (TAPVR)
Pulmonary veins drain into systemic venous circulation instead of the left atrium. Must have ASD or PFO for survival (for oxygenated blood to reach left heart).
Types (by drainage site):
| Type | Drainage | Frequency |
|---|---|---|
| Supracardiac | Superior vena cava or innominate vein | Most common (~50%) |
| Cardiac | Coronary sinus or right atrium | ~25% |
| Infracardiac/Subdiaphragmatic | IVC, portal vein, hepatic vein | ~25%, most often obstructed |
| Mixed | Multiple sites | ~5% |
Features:
- Hyperactive RV impulse, fixed split S2, systolic ejection murmur at LUSB, mid-diastolic rumble at LLSB
- ECG: RAD, RVH (RSR' in V1)
- CXR: "Snowman" sign (figure-of-8 appearance) from dilated vertical vein + SVC - seen in supracardiac type, rarely before 4 months
- Obstructed TAPVR (especially infracardiac): presents with pulmonary edema and severe cyanosis at birth - surgical emergency
Management: Surgical reconnection of the pulmonary venous confluence to the left atrium.
5. Truncus Arteriosus
A single arterial trunk arises from both ventricles and gives rise to the aorta, pulmonary arteries, and coronary arteries. Always associated with a large VSD. Associated with DiGeorge syndrome (22q11 deletion).
Features:
- Cyanosis + signs of pulmonary overcirculation (since pulmonary arteries arise from the trunk at systemic pressure before PVR drops)
- ECG: Biventricular hypertrophy
- Loud single S2, early systolic ejection click, systolic murmur
Management: Early surgical repair - VSD closure, separation of pulmonary arteries from the trunk, and placement of a RV-to-PA conduit (Rastelli-type repair).
Other Cyanotic CHDs
| Lesion | Key Features |
|---|---|
| Pulmonary atresia with intact septum | Duct-dependent; PGE1 + balloon valvotomy or BT shunt |
| Ebstein anomaly | Apical displacement of tricuspid valve; atrialized RV; Wolff-Parkinson-White often associated; wide split S2, "sail sound" |
| Hypoplastic left heart syndrome (HLHS) | Hypoplastic LV, aorta, mitral valve; presents in newborn period with circulatory collapse; Norwood → Glenn → Fontan |
| Double outlet right ventricle (DORV) | Both great vessels arise from RV; management depends on VSD location |
| Pulmonary atresia with VSD and MAPCAs | Major aortopulmonary collateral arteries supply lungs; requires unifocalization surgery |
General Approach to the Cyanotic Newborn
- Hyperoxia test (nitrogen washover test): Administer 100% O2 for 10 minutes. If PaO2 rises above 150-200 mmHg, cyanosis is likely pulmonary in origin. If PaO2 remains low (<100 mmHg), cardiac cause is likely (fixed R-to-L shunt).
- Immediate stabilization: PGE1 (0.05-0.1 µg/kg/min) if duct-dependent lesion is suspected - opens/maintains ductus arteriosus
- Echocardiography - definitive anatomical diagnosis
- Chest X-ray: Pulmonary blood flow (increased vs. decreased) and cardiac silhouette guide diagnosis
- ECG: Axis and chamber hypertrophy pattern narrow the differential
Diagnostic Summary Table
| Lesion | CXR | ECG | Key Murmur |
|---|---|---|---|
| TOF | Boot-shaped, ↓PVM | RAD, RVH | SEM at LMSB/LUSB |
| TGA | Egg on string, ↑PVM | RAD, RVH | Minimal (unless VSD) |
| Tricuspid atresia | Boot-shaped, ↓PVM | Superior axis, LVH | Systolic at LLSB (if VSD) |
| TAPVR | Snowman sign, ↑PVM | RAD, RVH (RSR') | SEM at LUSB + mid-diastolic rumble |
| Truncus arteriosus | Cardiomegaly, ↑PVM | BVH | SEM + early click |
| Ebstein anomaly | Massive cardiomegaly, ↓PVM | RBBB, delta waves (WPW) | TR murmur at LLSB |
Complications of Chronic Cyanosis
- Polycythemia and hyperviscosity - risk of stroke
- Brain abscess (R-to-L shunt bypasses pulmonary filter)
- Paradoxical embolism
- Coagulopathy (thrombocytopenia, clotting factor defects)
- Infective endocarditis
- Cerebrovascular accidents (thromboembolic or hemorrhagic)
- Growth retardation and developmental delay
- Gout (hyperuricemia from increased red cell turnover)
- Eisenmenger syndrome (irreversible pulmonary hypertension from long-standing L-to-R shunt that reverses)
Sources:
- Rosen's Emergency Medicine, 9th Ed. - Cyanotic Congenital Heart Defects section
- Sabiston Textbook of Surgery - Congenital Heart Disease, Chapter 113
- Robbins & Cotran Pathologic Basis of Disease - Right-to-Left Shunts
- Harriet Lane Handbook, 23rd Ed. - Cyanotic CHD
- Fuster and Hurst's The Heart, 15th Ed. - Cyanotic CHD categories
This is a shared conversation. Sign in to Orris to start your own chat.