Cholecystectomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have thorough information from authoritative sources. Let me compile a comprehensive response.
Cholecystectomy
Cholecystectomy is surgical removal of the gallbladder. It is one of the most common abdominal operations performed worldwide - over 750,000 are performed annually in the United States alone. Carl Langenbuch performed the first successful open cholecystectomy in 1882; Philippe Mouret introduced the laparoscopic approach in France in 1987, which quickly became the gold standard.
- Schwartz's Principles of Surgery, 11th ed., p. 1438-1442
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 1270-1271
Indications
| Indication | Details |
|---|---|
| Symptomatic cholelithiasis | Biliary colic, recurrent attacks |
| Acute cholecystitis | Calculous or acalculous |
| Chronic cholecystitis | Repeated episodes of inflammation |
| Choledocholithiasis | CBD stones (with or without ERCP) |
| Biliary pancreatitis | Same-admission for mild/interstitial disease |
| Biliary dyskinesia | Gallbladder EF <35% on HIDA scan; 90% symptom improvement |
| Gallbladder polyps | >1 cm, or symptomatic |
| Gallbladder carcinoma | Where technically resectable |
Contraindications
Absolute:
- Haemodynamic instability
- Uncontrolled coagulopathy
- Frank peritonitis (relative to laparoscopic approach)
- Severe COPD or severe cardiac failure (EF <20%) - inability to tolerate pneumoperitoneum
Formerly absolute, now relative (risk factors for difficult cholecystectomy):
- Acute cholecystitis, empyema/gangrene of gallbladder
- Biliary-enteric fistula, Mirizzi's syndrome
- Morbid obesity, cirrhosis, prior upper abdominal surgery
- Pregnancy, ventriculoperitoneal shunts, portal hypertension
Preoperative Assessment
- Full blood count, liver function tests, coagulation screen, renal function
- Chest X-ray and ECG if clinically indicated
- Abdominal ultrasound (assess stones, gallbladder wall, CBD diameter)
- CBD stone risk stratification (Table below)
- DVT prophylaxis: LMWH + antiembolic stockings
- Antibiotic prophylaxis: second-generation cephalosporin at induction of anaesthesia
- Informed consent (including risks of bile duct injury, conversion to open, bleeding, retained stones)
CBD Stone Risk Assessment (Bailey & Love):
| Risk | CBD Stone Risk | History | LFTs | CBD Diameter | Action |
|---|---|---|---|---|---|
| Low | 2-3% | No cholangitis/pancreatitis | Normal | ≤6 mm | None |
| Medium | 20-40% | Cholangitis or pancreatitis | 2x normal | 8-10 mm | MRCP ± ERCP |
| High | 50-80% | Jaundice + cholangitis | 2x normal | ≥10 mm | MRCP ± ERCP |
Laparoscopic Cholecystectomy - Technique
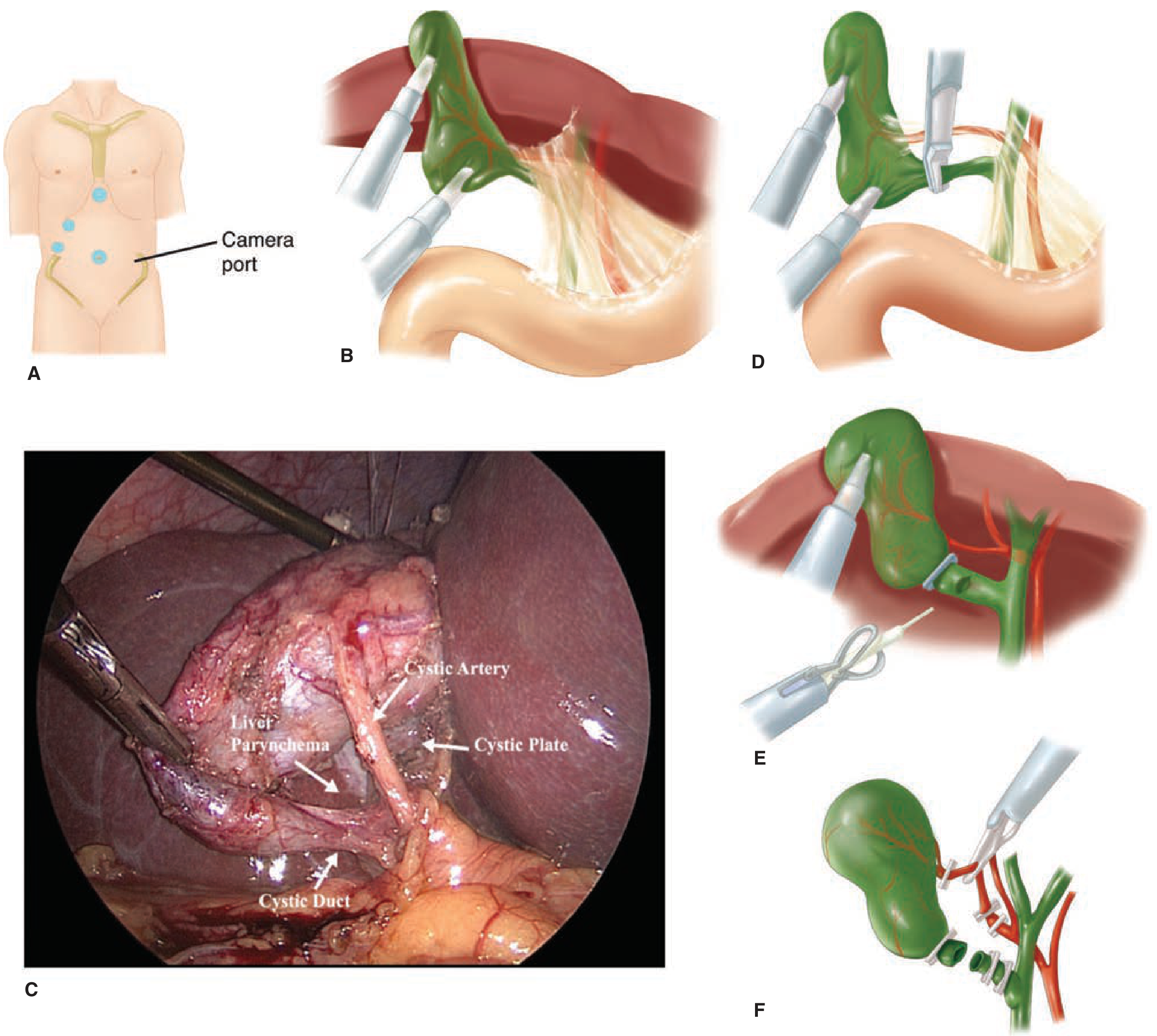
Figure: Laparoscopic cholecystectomy. (A) Trocar placement. (B) Fundus retracted cephalad to expose the hepatoduodenal ligament. (C) Intraoperative photo showing the Critical View of Safety with cystic artery, cystic plate, and cystic duct. (D) Clip on cystic duct. (E) Cholangiogram catheter insertion. (F) Division of cystic duct and artery. - Schwartz's Surgery
Port Placement (Standard 4-port)
- Camera port - supraumbilical (5 or 10 mm), 30° laparoscope
- Working port - epigastric (10-12 mm), surgeon's right hand
- Mid-clavicular port - right mid-clavicular (5 mm), surgeon's left hand
- Lateral port - right flank (5 mm), assistant retraction
Key Operative Steps
1. Pneumoperitoneum
- Established with CO2 via Veress needle (closed) or Hasson technique (open cut-down, preferred when prior surgery). Intra-abdominal pressure typically 12-15 mmHg.
2. Patient Positioning
- Supine, reverse Trendelenburg with left lateral tilt. Surgeon stands at patient's left (or between legs in split-leg position).
3. Retraction - Critical First Step
- Fundus grasped and retracted towards the patient's right shoulder (cephalad, over liver edge)
- Infundibulum retracted inferolaterally towards the right iliac fossa
- This opens the hepatocystic triangle, increases the cystic duct-CBD angle, and limits dissection above Rouvière's sulcus
4. Calot's Triangle Dissection
- Peritoneum on both anterior and posterior aspects of the hepatocystic triangle is divided
- Fat and fibrous tissue are cleared
- Dissection is kept close to the gallbladder wall
5. Critical View of Safety (CVS) - Mandatory Safety Step
Three criteria must ALL be met:
- Hepatocystic triangle cleared of all fat and fibrous tissue
- Lower one-third of the gallbladder separated from the liver to expose the cystic plate
- Only two structures seen entering the gallbladder (cystic duct and cystic artery)
CVS is the most important safety step - if it cannot be achieved, the surgeon must stop, consider alternatives (subtotal cholecystectomy, drain and refer, intraoperative cholangiogram), and not clip or divide any structure.
6. Clipping and Division
- Cystic duct and cystic artery are each double-clipped proximally and single-clipped distally, then divided
- Gallbladder dissected off the liver bed (cystic plate left on liver to prevent bile leak and bleeding)
7. Extraction
- Gallbladder extracted via umbilical port in a retrieval bag (prevents port-site contamination/seeding)
Intraoperative Cholangiogram (IOC)
- Routine vs. selective: remains debated; routine IOC detects CBD stones in ~7% of patients and helps delineate anatomy
- Selective indications: abnormal LFTs, history of jaundice or pancreatitis, dilated CBD on preoperative US, large CBD stones, failed preoperative ERCP, uncertain ductal anatomy
- ICG fluorescence cholangiography: real-time biliary tree visualisation using indocyanine green with special laparoscopic systems - reduces bile duct injury risk
- Technique: clip placed on proximal cystic duct; small incision on anterior surface; catheter secured; contrast injected under live fluoroscopy
Difficult Cholecystectomy - Red Flag Signs (Bailey & Love)
When these appear, stop and reassess before proceeding:
- Failure of timely progression of dissection
- Anatomical disorientation
- Difficulty in visualisation
Risk factors for difficult cholecystectomy include: Male sex, age >65, acute cholecystitis with >72-96 hours since onset, contracted or thickened gallbladder wall (>4-5 mm), distended gallbladder with impacted neck stone, gangrenous gallbladder, Mirizzi's syndrome, cirrhosis/portal hypertension, previous upper abdominal surgery.
Options when CVS cannot be achieved:
- Subtotal (partial) cholecystectomy: remove as much mucosa as possible, close cystic duct stump, wide drainage
- Cholecystostomy (drain the gallbladder, defer definitive surgery)
- Convert to open
- Obtain a cholangiogram to clarify anatomy
Open Cholecystectomy
Performed when laparoscopic approach is contraindicated or conversion is required. Incision options: upper midline, short subcostal (Kocher), or right upper transverse incision over the lateral rectus border.
Approach:
- Packs placed on hepatic flexure of colon, duodenum, and lesser omentum
- Artery/Duval forceps on infundibulum to put peritoneum over Calot's triangle under stretch
- Peritoneum divided close to gallbladder wall; fat cleared from Calot's triangle
- Cystic artery and duct identified, ligated, divided
- Gallbladder dissected from liver bed
"It is the left hand of the assistant that does all the work" - Moynihan (on retraction during open cholecystectomy)
Conversion to Open
- Elective setting: ~5% conversion rate
- Emergency/complicated gallstone disease: 10-30% conversion rate
- Conversion is not a failure - it is sound surgical judgment
- Must always be discussed with the patient preoperatively
Indications for conversion:
- Inability to tolerate pneumoperitoneum
- Complication not correctable laparoscopically
- Failure to identify key anatomical structures
- No progress over a defined period
Complications
| Complication | Detail |
|---|---|
| Mortality | ~0.1% for laparoscopic cholecystectomy |
| Bile duct injury | Most feared complication; historically higher with laparoscopic approach, now comparable to open with modern technique and CVS |
| Bile leak | From cystic duct stump or ducts of Luschka; presents with biloma/pain/fever post-op |
| Retained CBD stones | Managed with ERCP post-operatively |
| Haemorrhage | From cystic artery or liver bed |
| Wound infection | Less frequent than open surgery |
| Port-site hernia | Especially at 10/12 mm ports |
| Visceral injury | Bowel, liver, duodenum |
| Post-cholecystectomy syndrome | Persistent or recurrent symptoms after surgery |
Special Situations
Biliary Pancreatitis:
- Mild/interstitial pancreatitis: same-admission cholecystectomy recommended (reduces recurrence from 18% at 6 weeks to near zero; no increase in conversion rate)
- Moderately severe/necrotizing pancreatitis: interval cholecystectomy after inflammation resolves and fluid collections stabilize (at least 6 weeks)
- If patient cannot undergo surgery: biliary sphincterotomy prevents further AP but does not prevent biliary colic or acute cholecystitis
Biliary Dyskinesia:
- Diagnosed by HIDA scan with gallbladder EF <35%
- Cholecystectomy improves or resolves symptoms in up to 90% of cases
Acalculous Cholecystitis (ICU patients):
- Cholecystectomy when patient stable; percutaneous cholecystostomy as bridge to definitive surgery in critically ill patients
Single-port laparoscopic cholecystectomy:
- Improved cosmesis and possibly less postoperative pain
- But systematic reviews show higher failure rate, longer operative time, and increased blood loss versus standard 4-port approach
Key Anatomical Landmarks
- Triangle of Calot (hepatocystic triangle): Bounded by the cystic duct (inferiorly), common hepatic duct (medially), and inferior border of the liver (superiorly). Contains the cystic artery.
- Rouvière's sulcus: Hepatic fissure on the right lobe surface - dissection should remain anterior/inferior to this landmark
- Cystic plate: Connective tissue between gallbladder and liver bed; exposing its medial third confirms CVS
Sources: Schwartz's Principles of Surgery 11th ed.; Bailey and Love's Short Practice of Surgery 28th ed.; Sleisenger and Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.