Hypercalcemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypercalcemia"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have very comprehensive content. Let me compile the full response.
Hypercalcemia
Definition and Severity Classification
Hypercalcemia is defined as a total serum calcium > 10.5 mg/dL (2.62 mmol/L) or ionized calcium > 5.25 mg/dL (1.31 mmol/L).
| Grade | Total Serum Calcium |
|---|---|
| Mild | < 12 mg/dL (3.0 mmol/L) |
| Moderate | 12-14 mg/dL (3.0-3.5 mmol/L) |
| Severe | > 14 mg/dL (3.5 mmol/L) |
Prevalence is ~1-2% in the general population and 2-5% in hospitalized patients. - Goldman-Cecil Medicine, p. 1617
Pathophysiology
Hypercalcemia arises through three main mechanisms:
- Increased bone resorption - the most common (e.g., osteoclast activation by PTH, PTHrP, or lytic metastases)
- Increased GI calcium absorption - excess vitamin D or its analogues
- Decreased renal calcium excretion - e.g., thiazide diuretics, familial hypocalciuric hypercalcemia (FHH)
PTH acts on osteoblasts to upregulate RANKL, stimulating osteoclast differentiation and activity, while inhibiting osteoprotegerin - net result is calcium liberation from bone into the extracellular fluid. - Goldman-Cecil Medicine
Causes (classified by PTH level)
HIGH PTH
- Primary hyperparathyroidism (most common cause overall): solitary adenoma (~80%), hyperplasia (~15%), carcinoma (<1%), familial - MEN 1, MEN 2A, HPT-JT, FIHP
- Tertiary hyperparathyroidism - hyperplasia in chronic renal failure
LOW PTH (suppressed)
Malignancy (most common cause of symptomatic hypercalcemia):
- Humoral hypercalcemia of malignancy (HHM): PTHrP secretion by tumor (~80% of cancer-related cases) - carcinoma of lung, esophagus, renal cell, ovary, bladder
- Local osteolytic hypercalcemia (LOH): multiple myeloma, breast carcinoma
- 1,25(OH)₂D production: lymphoma, germinoma
- Ectopic PTH secretion (rare)
Excess Vitamin D:
- Exogenous: vitamin D toxicity (supplements, cod liver oil)
- Endogenous: granulomatous disorders (sarcoidosis, TB, histoplasmosis, coccidioidomycosis, leprosy, berylliosis), lymphoma
Drugs:
- Thiazide diuretics, lithium, milk-alkali syndrome, vitamin A toxicity, total parenteral nutrition, estrogens/antiestrogens, aminophylline, foscarnet
Other endocrine disorders:
- Thyrotoxicosis (mild, <12 mg/dL - responds to beta-blockers)
- Pheochromocytoma, acute adrenal insufficiency, VIPoma
Immobilization (especially in Paget disease, prolonged bed rest)
ALTERED CALCIUM-SENSING RECEPTOR SET POINT
- Familial Hypocalciuric Hypercalcemia (FHH) types 1-3 - autosomal dominant, asymptomatic, very low urinary calcium (calcium-to-creatinine clearance ratio <0.01); mutations in CaSR, G-protein alpha-11, or AP2S1
Primary hyperparathyroidism + malignancy account for nearly 90% of all cases. - Robbins Pathology, p. 1682
PTH-Based Diagnostic Differentiation
The intact PTH assay is the key first test in any hypercalcemia workup:
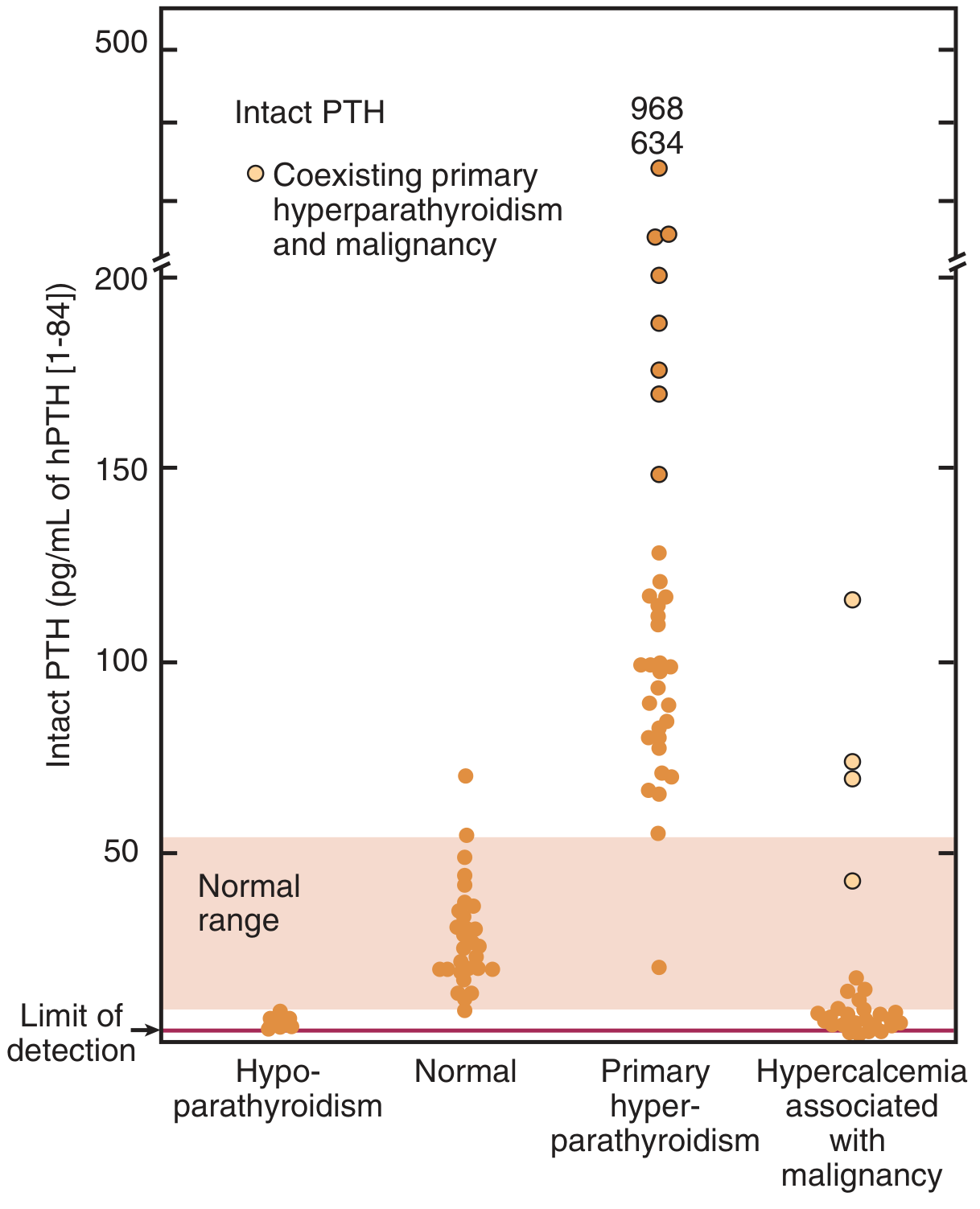
In primary hyperparathyroidism, PTH is elevated or inappropriately normal. In malignancy-associated hypercalcemia, PTH is low to undetectable. PTHrP assay is useful for confirming humoral hypercalcemia of malignancy.
Clinical Features: "Bones, Stones, Moans, and Abdominal Groans"
| System | Manifestations |
|---|---|
| Renal | Nephrolithiasis, nephrocalcinosis, polyuria, polydipsia (nephrogenic DI), renal insufficiency |
| Bone | Bone pain, fractures, osteitis fibrosa cystica, brown tumors (severe/chronic) |
| GI | Nausea, vomiting, constipation, anorexia, peptic ulcers, pancreatitis, gallstones |
| Neuromuscular | Weakness, fatigue, proximal muscle weakness, hyporeflexia |
| CNS/Psychiatric | Depression, lethargy, confusion, stupor, coma (in severe cases) |
| Cardiac | Shortened QT interval, aortic/mitral valve calcifications, hypertension |
Symptoms tend to correlate with the rapidity of rise rather than absolute level alone. Calcium levels >14 mg/dL are often symptomatic regardless. - Goldman-Cecil Medicine; Textbook of Family Medicine
Diagnosis: Workup
- Confirm true hypercalcemia - correct for albumin: corrected Ca = measured Ca + 0.8 × (4 - albumin g/dL); or measure ionized calcium directly
- Intact PTH - first and most important test
- Elevated/normal PTH → think primary hyperparathyroidism or FHH
- Suppressed PTH → think malignancy, vitamin D toxicity, granulomatous disease
- PTHrP if PTH suppressed and malignancy suspected
- 25-OH vitamin D and 1,25(OH)₂D - elevated 1,25(OH)₂D in granulomatous disorders and lymphoma
- 24-hour urinary calcium - low in FHH (Ca:Cr clearance ratio <0.01), high in primary hyperparathyroidism
- Serum phosphorus - tends to be low in primary HPT (PTH effect)
- Alkaline phosphatase, bone markers if bone disease suspected
- Imaging: neck ultrasound and sestamibi scan for parathyroid adenoma localization before surgery; DEXA scan for bone density in PHPT
Biochemical profile in primary hyperparathyroidism (Table of Family Medicine): serum Ca ~10.7 mg/dL, PTH ~119 pg/mL (ref 10-65), serum phosphorus ~2.8 mg/dL, elevated urinary calcium.
Management
Acute/Severe Hypercalcemia (Ca >13.5-14 mg/dL or symptomatic)
Step 1 - Aggressive IV hydration:
- Normal saline 2-4 L/day (first-line; expands volume, increases renal calcium excretion)
- Furosemide (loop diuretic) can be added in patients at risk of fluid overload (NOT thiazides)
Step 2 - Bisphosphonates (mainstay for malignancy-associated):
- IV zoledronic acid or pamidronate - inhibit osteoclast-mediated bone resorption
- Onset 2-4 days; peak effect at 4-7 days
Step 3 - Calcitonin:
- Salmon calcitonin 4 IU/kg SC/IM q12h - rapid onset (hours), but tachyphylaxis within 48-72h
- Used as a bridge while bisphosphonates take effect
Step 4 - Denosumab:
- Anti-RANKL monoclonal antibody - effective for bisphosphonate-refractory hypercalcemia
- Note: Rebound hypercalcemia can occur after denosumab discontinuation (recent systematic review, PMID 41571922)
Step 5 - Glucocorticoids:
- Useful for granulomatous disease (sarcoidosis) and vitamin D toxicity; reduce 1,25(OH)₂D production by activated macrophages
- Prednisolone 40-60 mg/day
Step 6 - Dialysis - last resort in severe refractory cases or renal failure
For malignancy-related 1,25(OH)₂D excess (lymphoma): glucocorticoids and ketoconazole are effective in addition to standard measures. (See systematic review PMID 34581546 on this entity.)
Chronic Management / Primary Hyperparathyroidism
Parathyroidectomy is the only cure and is indicated if ANY of these criteria are met:
- Any complication of PHPT (nephrolithiasis, osteitis fibrosa cystica)
- Serum Ca >1 mg/dL above upper normal limit
- Marked hypercalciuria (>400 mg/24h in men, >300 mg/24h in women) with increased stone risk
- Creatinine clearance <60 mL/min
- BMD T-score < -2.5 or vertebral fracture
- Age <50 years
- Episode of life-threatening hypercalcemia
Success rate ~98% by experienced surgeons. Bone mineral density improves over 6-10 years post-op with reduced fracture risk. - Goldman-Cecil Medicine, p. 1836
Watchful waiting (asymptomatic patients not meeting surgery criteria):
- Annual serum Ca, PTH, 25-OH-D, eGFR, 24h urine Ca
- DEXA every 1-2 years
- Ensure adequate hydration; avoid thiazides and immobilization
Cinacalcet (calcimimetic):
- Allosteric activator of the calcium-sensing receptor
- Indicated when surgery is not feasible; reduces PTH and calcium
- Dose: 30 mg once daily, titrated to max 180 mg/day
- Also used for severe secondary hyperparathyroidism in dialysis patients
Special Entities
Familial Hypocalciuric Hypercalcemia (FHH)
- Autosomal dominant, lifelong asymptomatic hypercalcemia
- Key distinction from PHPT: Ca:Cr clearance ratio <0.01, hypermagnesemia, normal PTH in 80%
- Genetic testing (CaSR, GNA11, AP2S1) is definitive
- Parathyroidectomy is NOT beneficial; these patients are often misdiagnosed with PHPT
Milk-Alkali Syndrome
- Caused by excessive calcium carbonate ingestion (antacids, supplements)
- Triad: hypercalcemia, metabolic alkalosis, renal insufficiency
Hypercalcemia of Immobilization
- Occurs with prolonged immobilization, especially in young patients and those with high bone turnover (Paget disease)
- Treatment: mobilization, saline hydration, bisphosphonates if needed
Key Summary Points
- Most common cause overall: Primary hyperparathyroidism
- Most common cause of symptomatic/acute hypercalcemia: Malignancy
- These two causes account for ~90% of cases
- First test: Intact PTH
- Acute treatment priority: IV saline hydration first, then IV bisphosphonates
- Only cure for PHPT: Parathyroidectomy
- Do not confuse with FHH - check urinary calcium and genetic testing
Sources: Goldman-Cecil Medicine 22E; Brenner & Rector's The Kidney; Robbins Pathology; Textbook of Family Medicine 9E; Schwartz's Principles of Surgery 11E
This is a shared conversation. Sign in to Orris to start your own chat.