Define blood pressure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a thorough definition of blood pressure drawn from authoritative medical textbooks:
Blood Pressure - Definition
Blood pressure is the force exerted by blood against any unit area of the vessel wall. It is the product of the interaction between cardiac output (myocardial pump function) and peripheral vascular resistance (vascular tone).
- Guyton and Hall Textbook of Medical Physiology
Units of Measurement
Blood pressure is almost universally measured in millimeters of mercury (mmHg) - a standard introduced by Poiseuille in 1846. A pressure of 100 mmHg means the force is sufficient to push a column of mercury upward by 100 mm against gravity. It can also be expressed in centimeters of water (cm H₂O), where 1 mmHg = 1.36 cm H₂O (because mercury is 13.6 times denser than water).
- Guyton and Hall Textbook of Medical Physiology
The Two Components
| Component | Definition | Typical Normal Value |
|---|---|---|
| Systolic BP (SBP) | Peak pressure in the arteries during ventricular contraction (systole) | ~120 mmHg |
| Diastolic BP (DBP) | Minimum pressure in the arteries when the heart is at rest between beats (diastole) | ~80 mmHg |
| Mean Arterial Pressure (MAP) | Average pressure throughout the cardiac cycle | ~93 mmHg |
Blood pressure is written as SBP/DBP (e.g., 120/80 mmHg).
Physiological Determinants
Blood pressure is governed by the relationship:
BP = Cardiac Output (CO) × Total Peripheral Resistance (TPR)
Key factors that influence BP include:
- Heart rate and stroke volume (determinants of cardiac output)
- Arterial wall tone and elasticity (vascular resistance)
- Blood volume (circulating fluid)
- Neurohormonal regulation (sympathetic nervous system, renin-angiotensin-aldosterone system, vasopressin)
Clinical Classifications (Adults)
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Normal | < 120 | < 80 |
| Elevated | 120-129 | < 80 |
| Hypertension Stage 1 | 130-139 | 80-89 |
| Hypertension Stage 2 | ≥ 140 | ≥ 90 |
| Hypertensive Crisis | > 180 | > 120 |
| Hypotension | < 90 | < 60 |
(Based on the 2017 ACC/AHA guideline, as cited in Goldman-Cecil Medicine)
Clinical Significance
Blood pressure is one of the most important prognostic indicators in cardiovascular medicine. Elevated BP (hypertension) damages arterial walls, the heart, kidneys, and brain over time. Low BP (hypotension, SBP < 85-90 mmHg) or signs of poor peripheral perfusion are serious warning signs - particularly in heart failure or shock. Notably, children and fit young adults can maintain a normal BP even in profound shock due to compensatory mechanisms like increased peripheral vasoconstriction.
- Braunwald's Heart Disease; Bailey and Love's Short Practice of Surgery
Define arterial blood pressure. Enumerate different mechanisms for blood pressure regulation. Describe long term regulation of blood pressure.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive, well-sourced content. Let me compile the full answer.
Arterial Blood Pressure - Definition, Regulatory Mechanisms, and Long-Term Regulation
1. Definition of Arterial Blood Pressure
Arterial blood pressure is the force exerted by circulating blood against the walls of the arteries. It is the product of cardiac output (CO) and total peripheral resistance (TPR):
BP = Cardiac Output × Total Peripheral Resistance
- Cardiac output is determined by heart rate and stroke volume (influenced by filling pressure/preload, contractility, and afterload).
- Total peripheral resistance is regulated primarily at the arteriolar level by neural (sympathetic) and humoral (angiotensin II, catecholamines, endothelin, nitric oxide, prostaglandins) factors.
Blood pressure is expressed in mmHg as systolic / diastolic:
| Parameter | Description | Normal Value |
|---|---|---|
| Systolic BP | Peak pressure during ventricular contraction | ~120 mmHg |
| Diastolic BP | Minimum pressure during cardiac relaxation | ~80 mmHg |
| Pulse Pressure | Systolic - Diastolic | ~40 mmHg |
| Mean Arterial Pressure (MAP) | DBP + 1/3 Pulse Pressure | ~93 mmHg |
Both low pressure (hypotension → organ ischemia) and high pressure (hypertension → vessel and end-organ damage) are pathological. Systemic and local blood pressure must be held within a narrow range to maintain health.
- Robbins & Kumar Basic Pathology; Guyton and Hall Textbook of Medical Physiology
2. Mechanisms for Blood Pressure Regulation
The regulatory mechanisms are classically classified by their speed of onset:
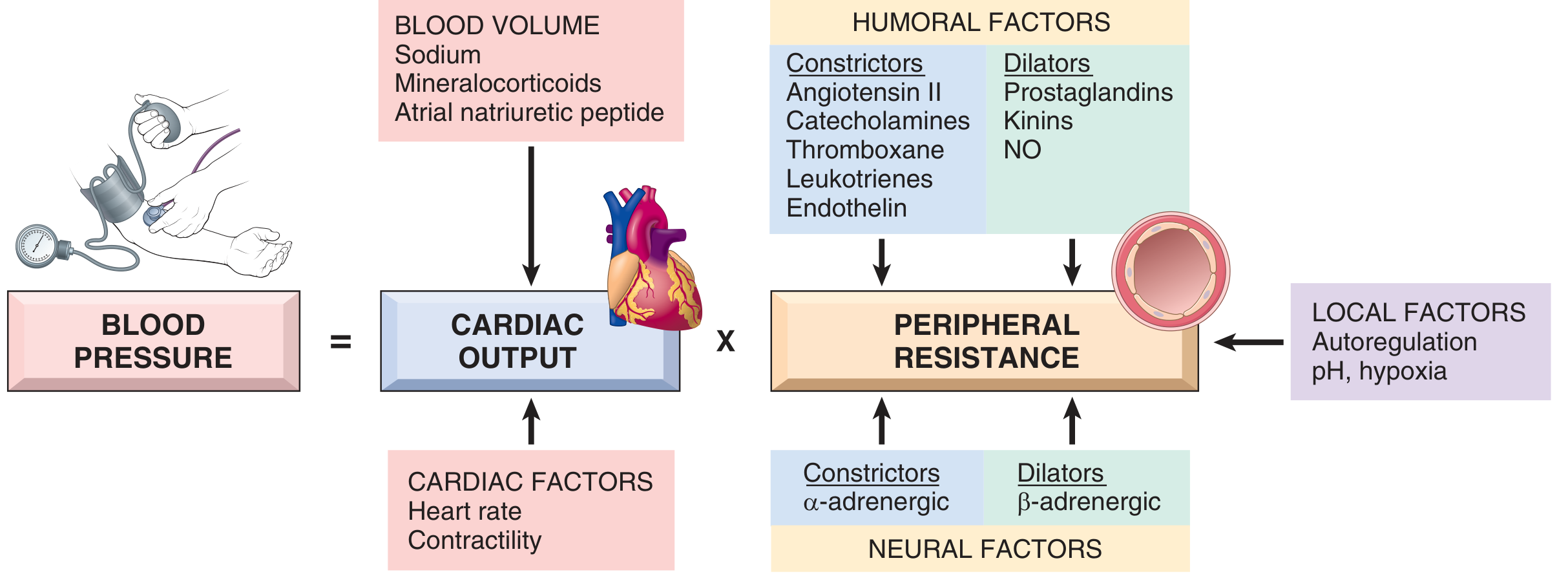
Fig. 8.2 - Blood pressure regulation (Robbins & Kumar Basic Pathology)
A. Rapid (Short-Term) Mechanisms - Seconds to Minutes
These are all negative feedback reflex loops composed of: detector → afferent pathway → CNS coordinating center → efferent pathway → effector.
1. Baroreceptor Reflex (Most Important)
The best-known mechanism for rapid pressure control.
- Receptors: Spray-type stretch receptors (baroreceptors/pressoreceptors) located in the walls of large arteries, especially:
- Carotid sinus (internal carotid artery, above carotid bifurcation)
- Aortic arch
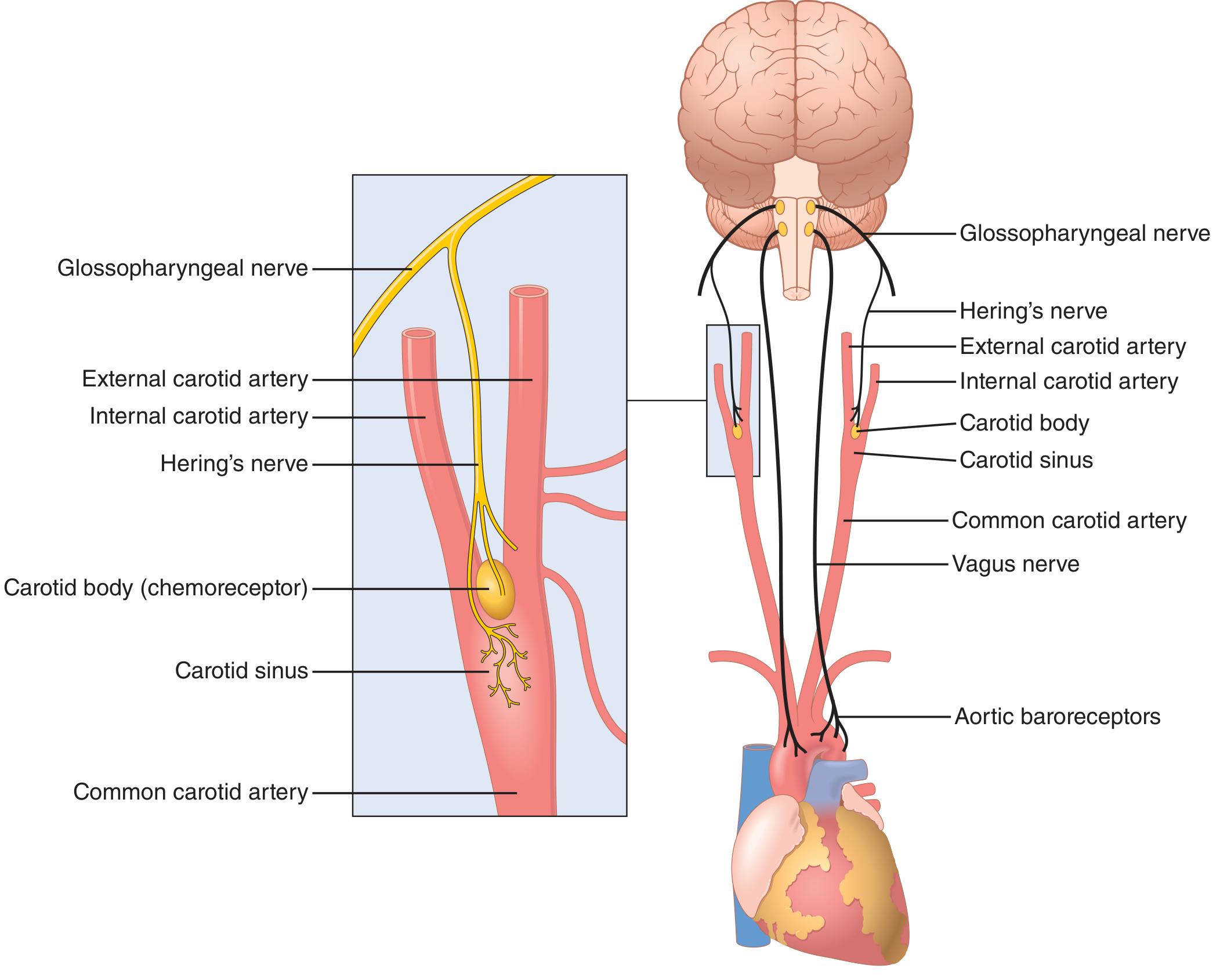
Fig. 18.5 - Baroreceptor system for controlling arterial pressure (Guyton and Hall)
-
Afferent pathways:
- Carotid sinus → Hering's nerve → glossopharyngeal nerve (CN IX) → nucleus tractus solitarius (NTS) in medulla
- Aortic arch → vagus nerve (CN X) → NTS
-
How it works:
- Rise in BP → baroreceptors stretched → ↑ firing to NTS → inhibition of vasomotor center + activation of vagal center → vasodilation + bradycardia → BP falls back to normal
- Fall in BP → ↓ baroreceptor firing → sympathetic excitation → vasoconstriction + tachycardia + ↑ contractility → BP rises
-
Operating range: Baroreceptors respond most sensitively in the 60-180 mmHg range. Aortic receptors operate ~30 mmHg higher than carotid receptors.
-
Buffer function: The baroreflex acts as a "pressure buffer," reducing minute-by-minute BP variation to about one-third of what it would be without baroreceptors. After baroreceptor denervation in dogs, BP fluctuated from 50 to >160 mmHg throughout the day.
-
Guyton and Hall Textbook of Medical Physiology
2. Chemoreceptor Reflex
-
Peripheral chemoreceptors - carotid bodies (between external and internal carotid arteries) and aortic bodies (under aortic arch concavity)
-
Stimulated by ↓ PO₂, ↑ PCO₂, or ↓ pH in arterial blood
-
Afferents travel via CN IX (carotid body) and CN X (aortic bodies) to the medulla
-
Intrinsic medullary response: vasoconstriction and bradycardia
-
Unlike baroreceptors (which exert negative drive on the vasomotor center), peripheral chemoreceptors exert a positive drive on the vasomotor center
-
Primary role is ventilatory regulation, but they also contribute to BP control
-
Medical Physiology (Boron & Boulpaep)
3. CNS Ischemic Response
-
When blood flow to the vasomotor center in the lower brain stem falls severely, causing cerebral ischemia (BP < 60 mmHg), CO₂ and lactic acid accumulate locally
-
This causes massive sympathetic excitation - the most powerful of all sympathetic vasomotor activators
-
Can raise arterial pressure to as high as 250 mmHg for up to 10 minutes
-
Renal arteriolar constriction may be so severe that urine output ceases entirely
-
Acts as a "last-resort" mechanism - does not activate until BP is critically low
-
Guyton and Hall Textbook of Medical Physiology
4. Bainbridge Reflex (Atrial Stretch Reflex)
-
Stretch receptors in the atria respond to increased blood volume/atrial filling
-
Afferents via vagus → medulla → efferent sympathetic and vagal nerves
-
Results in tachycardia and increased contractility to prevent venous pooling and congestion
-
Direct atrial stretch of the sinus node can increase heart rate by ~15%; the Bainbridge reflex adds a further 40-60%
-
Guyton and Hall Textbook of Medical Physiology
B. Intermediate Mechanisms - Minutes to Hours
These activate over minutes to hours and act via hormonal and vascular mechanisms.
| Mechanism | Time Course | Action |
|---|---|---|
| Renin-Angiotensin System (acute) | 20-60 min | Vasoconstriction via Ang II, ↑ aldosterone |
| Stress Relaxation of Vessels | Minutes | Vessel walls relax/contract to adjust capacity |
| Capillary Fluid Shift | 10-60 min | Fluid moves between interstitium and capillaries to adjust blood volume |
| Vascular autoregulation | Minutes | Local tissues regulate own blood flow based on metabolic need, pH, hypoxia |
C. Long-Term Mechanisms - Hours to Days
The primary long-term control mechanism is the renal-body fluid system.
3. Long-Term Regulation of Blood Pressure
Long-term regulation is the most powerful and the only mechanism with near-infinite feedback gain - capable of returning BP precisely to its set point regardless of the magnitude of the initial disturbance.
The Renal-Body Fluid System (Pressure Natriuresis/Diuresis)
The kidneys regulate blood pressure by controlling blood volume through adjustments in salt and water excretion:
- Pressure diuresis: When arterial pressure rises, the kidneys dramatically increase water output
- Pressure natriuresis: Simultaneously, sodium output increases proportionally
- At 50 mmHg → urine output ≈ 0
- At 100 mmHg (normal) → normal urine output
- At 200 mmHg → urine output is 4-6 times normal
The equilibrium point: The arterial pressure must stabilize at exactly the point where renal fluid output equals fluid intake. This creates an infinitely powerful negative feedback:
- If BP rises above equilibrium → fluid output > intake → blood volume falls → BP returns to equilibrium
- If BP falls below equilibrium → fluid output < intake → blood volume rises → BP returns to equilibrium
This means, under ideal conditions, the kidney will not stop correcting until BP has returned exactly to the equilibrium point - giving the system near-infinite gain for long-term pressure control.
- Guyton and Hall Textbook of Medical Physiology
The Renin-Angiotensin-Aldosterone System (RAAS)
The RAAS amplifies the renal pressure mechanism and is the primary hormonal axis for long-term BP control:
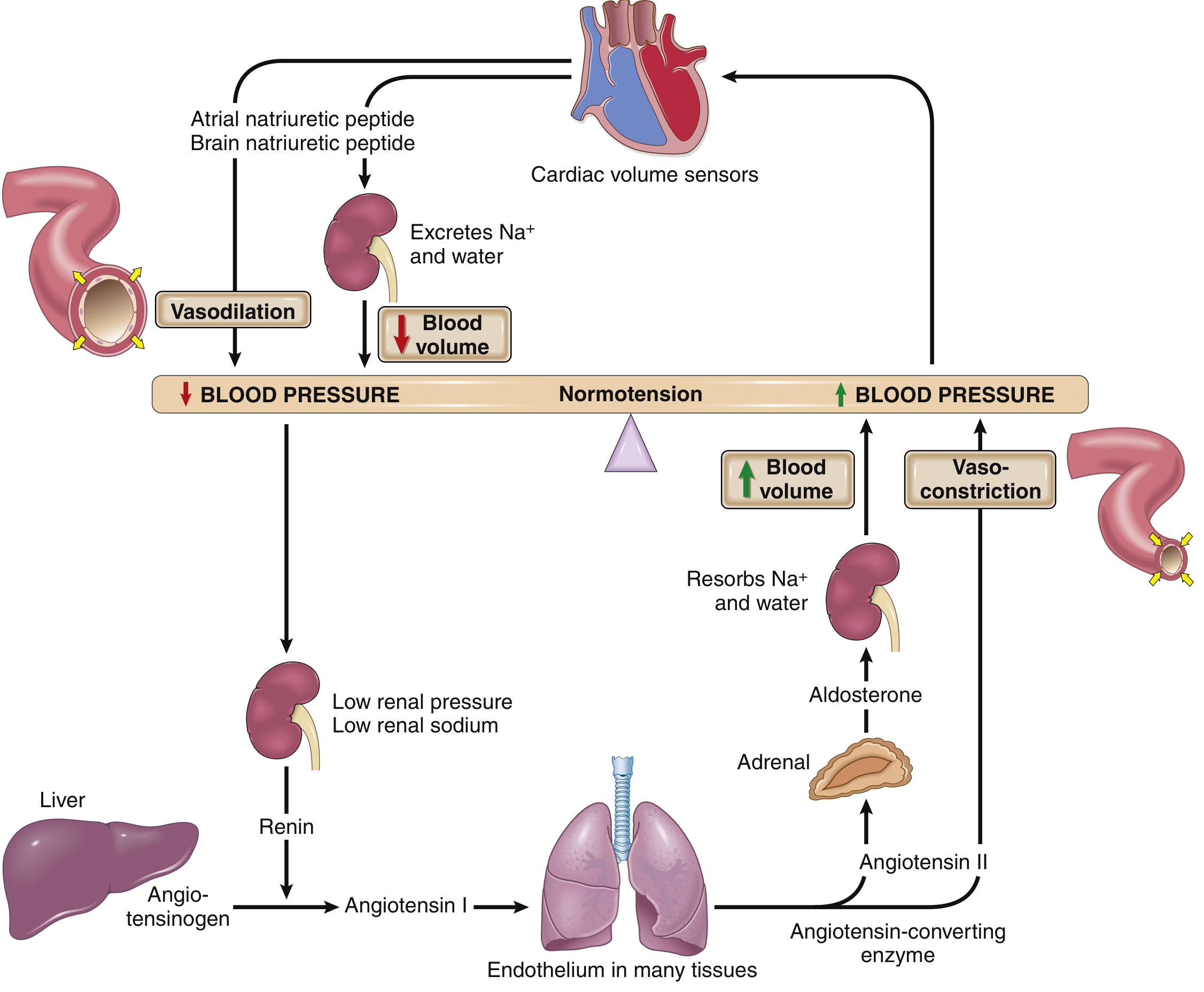
Fig. 8.3 - Renin-angiotensin-aldosterone and natriuretic peptide interplay (Robbins & Kumar Basic Pathology)
Steps in RAAS activation:
-
Renin is released from renal juxtaglomerular (JG) cells in response to:
- Low perfusion pressure in afferent arterioles
- Low sodium in the distal convoluted tubule (macula densa sensing)
- Sympathetic stimulation
-
Renin cleaves hepatic angiotensinogen → Angiotensin I
-
ACE (angiotensin-converting enzyme), produced mainly in vascular endothelium, converts Ang I → Angiotensin II
-
Angiotensin II raises BP by:
- Direct vasoconstriction of arterial smooth muscle
- Stimulating aldosterone release from the adrenal cortex
- Increasing tubular sodium reabsorption directly
-
Aldosterone increases sodium (and water) reabsorption in the distal convoluted tubule and collecting duct via ENaC (epithelial sodium channel), expanding blood volume → ↑ BP
- Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease
Vasodilator Counter-Regulation
The system is balanced by vasodilatory mechanisms:
- Natriuretic Peptides (ANP/BNP): Released from atrial/ventricular myocardium when blood volume expands. They inhibit distal tubular sodium reabsorption, cause diuresis, and induce systemic vasodilation - acting as "cardiac volume sensors" to counteract volume overload.
- Renal vasodilators: Prostaglandins and nitric oxide produced by the kidney counterbalance angiotensin II's vasopressor effects.
- Vascular endothelium: Continuously produces NO (vasodilatory) to maintain baseline vascular tone.
Neural and Hormonal Amplification of Pressure Natriuresis
The renal fluid system does not act in isolation. During chronic BP elevation:
- ↑ BP → ↓ sympathetic activity (via baroreceptors) → ↓ renal sympathetic tone → ↑ natriuresis
- ↑ BP → ↓ Ang II and aldosterone formation → further ↑ sodium excretion
This combined direct + indirect amplification makes pressure natriuresis/diuresis extremely powerful for long-term BP control.
In most healthy individuals, even a 6-fold increase in salt intake causes only a small change in BP due to the steep chronic renal output curve. However, in salt-sensitive individuals (those with reduced functional nephrons, excess Ang II/aldosterone, or aging-related nephron loss), even moderate salt increases cause significant BP rises.
- Guyton and Hall Textbook of Medical Physiology
Summary Table: BP Regulatory Mechanisms
| Mechanism | Onset | Duration | Gain | Primary Action |
|---|---|---|---|---|
| Baroreceptor reflex | Seconds | Short | Moderate | ↑/↓ sympathetic tone, HR, vasomotor |
| Chemoreceptor reflex | Seconds | Short | Low | Vasoconstriction in hypoxia/hypercapnia |
| CNS ischemic response | Seconds | Short | Very high | Emergency vasoconstriction |
| Bainbridge reflex | Seconds | Short | Low | ↑ HR with volume loading |
| Stress relaxation | Minutes | Intermediate | Moderate | Passive vessel wall adjustment |
| Capillary fluid shift | 10-60 min | Intermediate | Moderate | Blood volume adjustment |
| RAAS (acute) | 20-60 min | Intermediate | Moderate | Vasoconstriction, ↑ Na retention |
| Renal-body fluid (pressure natriuresis) | Hours-Days | Permanent | Near-infinite | Blood volume control via Na/water |
| RAAS (chronic) + Aldosterone | Hours-Days | Sustained | High | Long-term Na/water balance |
| ANP/BNP | Hours | Sustained | Moderate | Counter-regulation of volume overload |
This is a shared conversation. Sign in to Orris to start your own chat.