Colon carcinoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"colorectal cancer" AND "treatment"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have extensive, high-quality content from multiple authoritative sources. Let me compile the comprehensive answer.
Colon Carcinoma
Epidemiology
Colorectal cancer (CRC) is the third most common malignancy worldwide and the second most common cause of cancer death in Europe, North America, and Australasia among non-smokers. In the UK alone, approximately 42,000 new cases are diagnosed annually, with around 16,000 deaths per year. The lifetime risk is approximately 1 in 14 for men and 1 in 19 for women. The burden is greater in men (56% vs 44%). The incidence increases sharply with age - nearly three-quarters of cases occur in people aged 65 or older. CRC is less frequent in resource-poor countries, strongly implicating dietary and environmental factors.
- Bailey and Love's Short Practice of Surgery, p. 1380
- Grainger & Allison's Diagnostic Radiology, p. 572
Aetiology and Risk Factors
Dietary and Environmental
- High intake of red and processed meat (haem iron, N-nitroso compounds) is the strongest dietary risk factor worldwide
- Low dietary fibre - increases colonic transit time, prolonging mucosal exposure to carcinogens; emerging evidence also implicates the colonic microbiota in inflammation and gene methylation
- Smoking and alcohol increase risk; obesity is an independent risk factor
- Aspirin/NSAIDs (prostaglandin inhibitors) have substantial epidemiological evidence for protection against CRC
- High magnesium and calcium intake may be protective
Hereditary Risk Factors (~10% of cases)
- Familial Adenomatous Polyposis (FAP): Hundreds to thousands of adenomatous polyps develop; CRC is virtually inevitable without intervention. The accompanying congenital hypertrophy of the retinal pigment epithelium (CHRPE) helps identify at-risk family members. Prophylactic colectomy is advocated.
- Lynch Syndrome (Hereditary Non-Polyposis CRC, HNPCC): Defective DNA mismatch repair genes (MLH1, MSH2, etc.). Associated with right-sided tumours showing microsatellite instability (MSI). Distinguished from sporadic MSI by absence of BRAF V600E mutation.
- Family history: A first-degree relative with CRC before age 50 suggests a familial syndrome.
Chronic Inflammatory Bowel Disease
Long-standing ulcerative colitis and Crohn's disease are independent risk factors.
- Pye's Surgical Handicraft, p. 275
- Bailey and Love's, p. 1380
Pathogenesis: The Adenoma-Carcinoma Sequence
The adenoma-carcinoma sequence, first described by Fearon and Vogelstein (1990), is the dominant pathway in sporadic CRC. It is not a simple stepwise progression but a complex array of multiple genetic alterations.
Key molecular events:
| Gene | Alteration | Significance |
|---|---|---|
| APC | Mutation | Early event; present in ~2/3 of adenomas |
| KRAS | Activating mutation (codons 12, 13, 61) | Intermediate event; more common in larger lesions; 35-45% of CRCs |
| p53 | Mutation | Marker of invasion; mainly in carcinomas, not adenomas |
| BRAF V600E | Mutation | ~10% of CRCs; mutually exclusive with KRAS; associated with proximal MSI tumours; confers poor prognosis and resistance to anti-EGFR therapy |
| PIK3CA | Mutation (~20%) | Activates AKT1; resistance to anti-EGFR therapy |
| EGFR | Overexpression (~80%) | Poor prognosis; target for cetuximab/panitumumab |
Consensus Molecular Subtypes (CMS)
A recent international consortium identified four CMS categories based on >4000 patients' gene expression:
- CMS1: MSI, right-sided, hypermethylated (Lynch/sporadic)
- CMS2: WNT and MYC signalling activation
- CMS3: Metabolic dysregulation
- CMS4: TGF-beta activation
Evidence for the adenoma-carcinoma sequence:
-
Distribution of adenomas mirrors that of cancers (~70% left-sided)
-
Larger adenomas are more likely to be dysplastic
-
Adenomas found in 1/3 of specimens resected for CRC
-
Colonoscopy screening with polypectomy reduces CRC incidence
-
Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 1836-1837
-
Bailey and Love's, p. 1380
Distribution
- 50-55% of tumours arise in the sigmoid colon and rectum
- The rectum alone accounts for approximately one-third of cases
- Approximately two-thirds of colorectal cancers arise in the colon
Clinical Presentation
Symptoms depend on tumour location:
| Location | Typical Presentation |
|---|---|
| Left colon / sigmoid | Change in bowel habit, rectal bleeding, tenesmus |
| Right colon / caecum | Iron deficiency anaemia (occult bleeding), palpable mass |
| Any site | Weight loss, malignant ascites, symptoms of distant metastases |
| Advanced | Intestinal obstruction, perforation, fistula formation |
Synchronous polyps or carcinomas occur in 3-5% of cases.
- Bailey and Love's, p. 1381
Colonoscopic Appearance
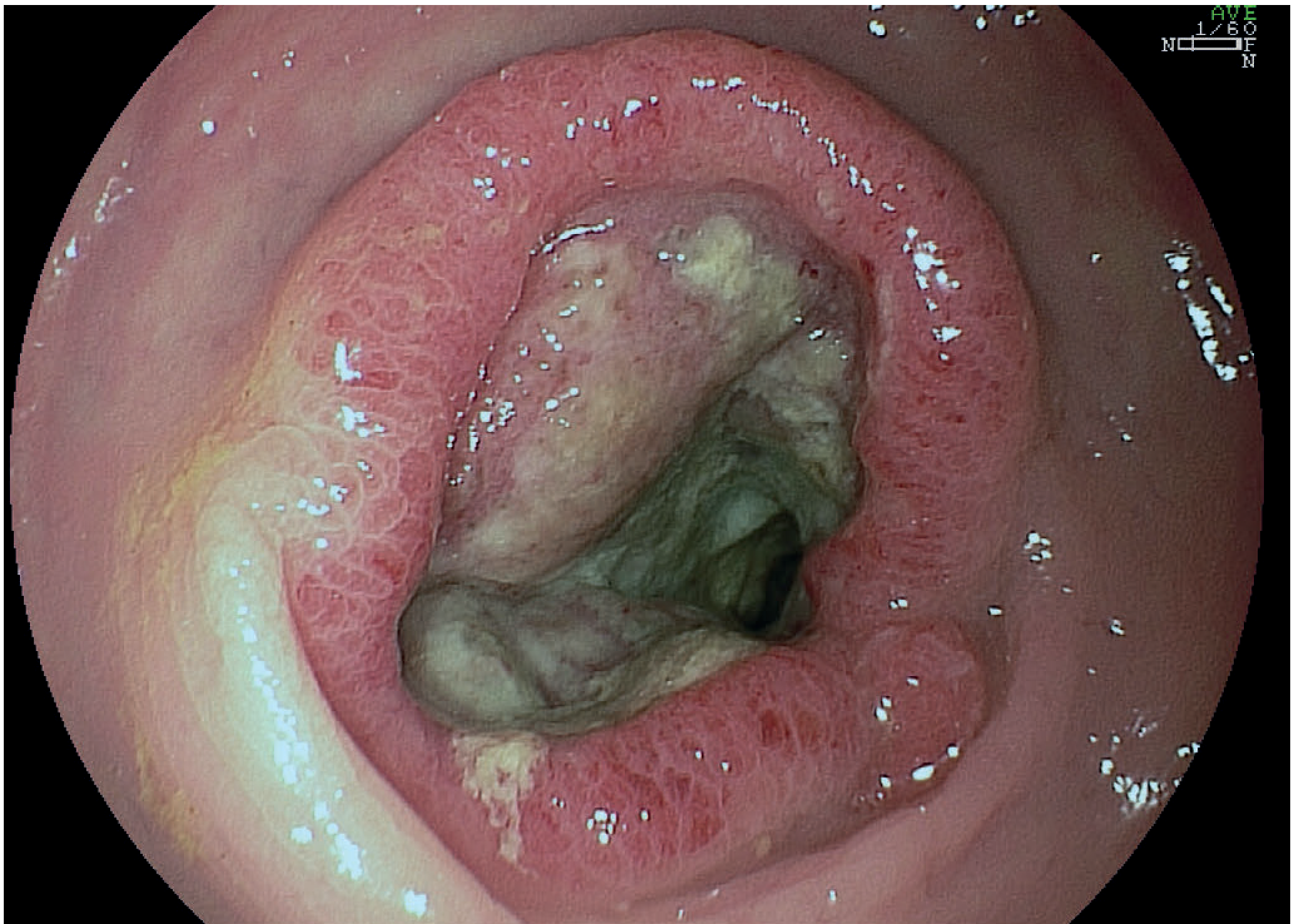
Colon cancer seen at colonoscopy - Bailey and Love's Short Practice of Surgery
Investigation
Screening
Suited to screening because earlier-stage disease has far better prognosis and polypectomy prevents cancer development.
- UK: Faecal Immunochemical Test (FIT) every 2 years for ages 60-74, followed by colonoscopy if positive. Replaced the older guaiac-based FOBT (which showed 15-20% reduction in CRC mortality).
- USA (Goldman-Cecil / USPSTF): Routine screening for adults aged 45-75; options include annual high-sensitivity FOBT/FIT, multitargeted stool DNA (every 1-3 years), CT colonography (every 5 years), or colonoscopy (every 10 years).
Endoscopy
- Flexible sigmoidoscopy: Rapid, no sedation needed; detects up to 70% of cancers; cannot visualise proximal colon. Finding left-sided polyps mandates completion colonoscopy.
- Colonoscopy: Gold standard - provides histological diagnosis AND detects synchronous lesions. Risk of perforation: 1:1000.
Radiology
- CT colonography (virtual colonoscopy): Equivalent sensitivity to colonoscopy for detecting CRC; picks up polyps ≥6 mm. Less invasive but cannot provide biopsy.
- CT chest/abdomen/pelvis: Standard staging for systemic disease. Colon cancer staging.
- MRI pelvis: Essential for local staging in rectal cancer; increasingly being evaluated for locally advanced colon cancer.
CT Staging Image
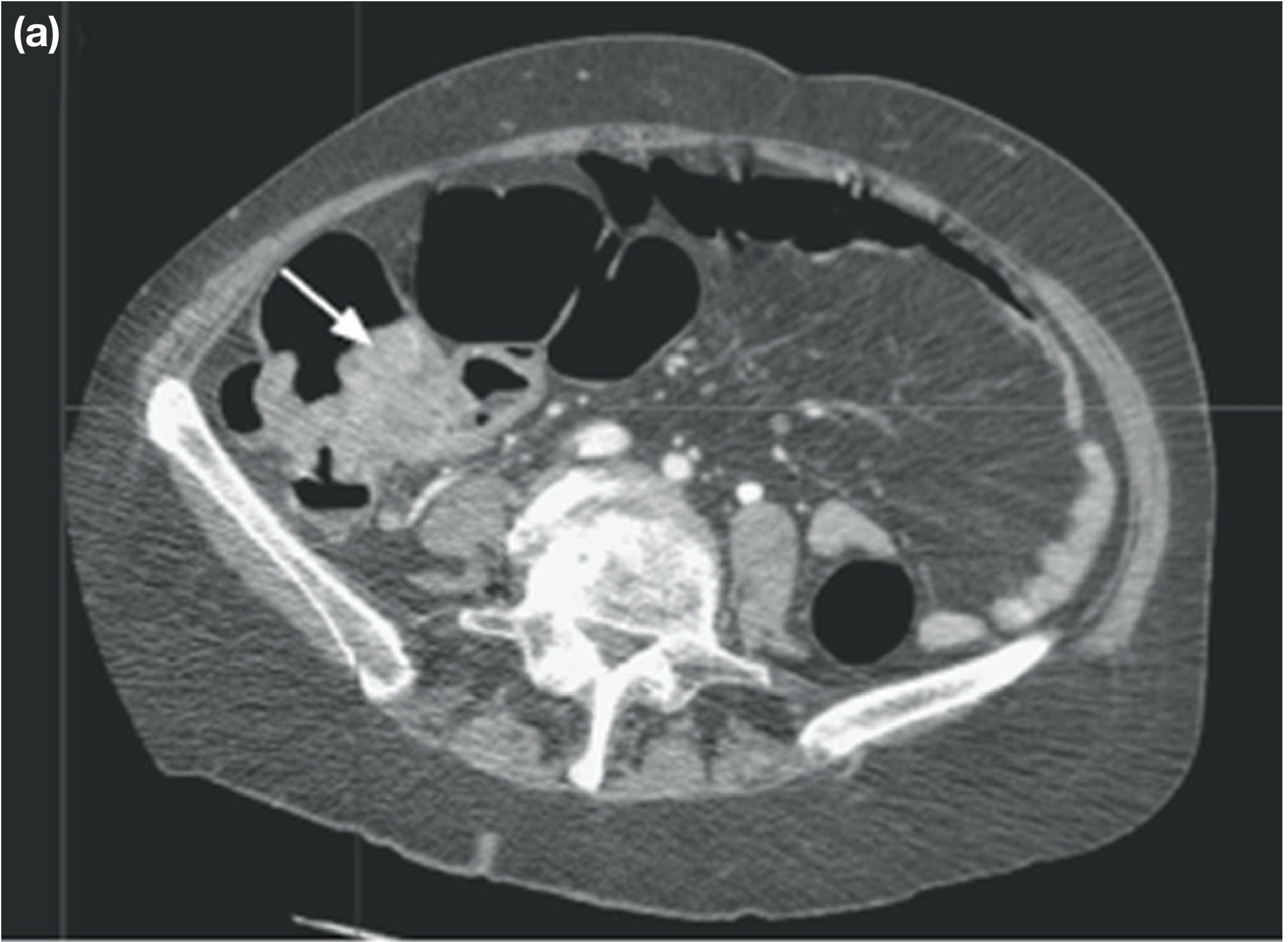
CT scan of abdomen showing a caecal tumour (arrow) - Bailey and Love's Short Practice of Surgery
Staging
TNM System (8th Edition - International Standard)
| UICC/TNM | Tumour Extent | Dukes | 5-Year Survival |
|---|---|---|---|
| Stage I | T1: Submucosa; T2: Muscularis propria - N0M0 | A | 85-95% |
| Stage II | T3: Pericolic tissue; T4a: Visceral peritoneum; T4b: Adjacent organs - N0M0 | B | 60-80% |
| Stage III | N1: 1-3 nodes; N2: ≥4 nodes | C | 30-60% |
| Stage IVa | M1a: Single distant organ | D | <10% |
| Stage IVb | M1b: Multiple distant organs | D | <10% |
| Stage IVc | M1c: Peritoneal metastasis | D | <10% |
Dukes' Staging (Simplified, Widely Used)
- A: Invasion into but not breaching muscularis propria
- B: Breaching muscularis propria, no lymph node involvement
- C: Lymph node metastases present
- D: Distant metastases (not originally described by Dukes himself)
Prognostic Factors
-
Degree of cellular differentiation (grade)
-
Lymphovascular invasion
-
Preoperative CEA elevation
-
Microsatellite instability status
-
Amount of lymphocyte infiltration
-
Extent of fibrotic stromal reaction (greater fibrosis = worse outlook)
-
Grainger & Allison's, p. 573; Pye's Surgical Handicraft, p. 275; Bailey and Love's, p. 1381
Molecular Biomarkers for Treatment Planning
| Marker | Frequency | Clinical Relevance |
|---|---|---|
| KRAS/NRAS mutation | 35-45% | Predicts NO benefit from anti-EGFR therapy (cetuximab, panitumumab) |
| BRAF V600E mutation | ~10% | Worse prognosis; resistance to anti-EGFR; distinguishes sporadic from Lynch MSI |
| PIK3CA mutation | ~20% | Resistance to anti-EGFR; may coexist with KRAS mutations |
| MSI-H/dMMR | ~15% | Better response to immunotherapy (pembrolizumab); poor response to 5-FU alone |
| EGFR overexpression | ~80% | Target for cetuximab/panitumumab in KRAS/NRAS/BRAF wild-type patients |
NCCN and ASCO guidelines state that patients with any known KRAS or NRAS mutation should not receive EGFR inhibitors.
- Henry's Clinical Diagnosis and Management, p. 1837-1839
Surgical Treatment
Surgery is the mainstay of treatment for all stages of colon cancer.
Surgical Principles
- Resection of the segment of colon bearing the tumour with its draining locoregional lymph nodes
- Extent of resection governed by the anatomy of the blood supply
- Complete mesocolic excision (CME): Dissection along embryological planes to maximise lymph node harvest - analogous to TME in rectal cancer
- Primary anastomosis where possible; defunctioning stoma if healing is uncertain
- Stapling and hand-suturing techniques have comparable anastomotic leak rates
Specific Operations by Tumour Location
| Tumour Location | Operation |
|---|---|
| Caecum / ascending colon | Right hemicolectomy (ligation of ileocolic artery at origin from SMA) |
| Transverse colon | Extended right or transverse colectomy |
| Descending colon | Left hemicolectomy (ligation of inferior mesenteric artery) |
| Sigmoid colon | Sigmoid colectomy or high anterior resection |
| Rectum | Anterior resection or abdominoperineal excision of the rectum (APER) with permanent end colostomy |
Laparoscopic vs Open Surgery
Laparoscopic colectomy is increasingly the standard approach; it is associated with shorter hospital stay, faster recovery, and equivalent oncological outcomes.
Liver Metastases
Colon cancers have a marked propensity to metastasise to the liver. Solitary or limited hepatic metastases may be resected or ablated with curative intent. Intraoperative ultrasonography helps detect occult hepatic lesions.
Enhanced Recovery After Surgery (ERAS)
Key elements: carbohydrate loading preoperatively, minimal fasting, epidural/regional analgesia, early mobilisation, early oral feeding, and avoidance of routine nasogastric tubes and drains.
Mechanical bowel preparation combined with oral antibiotics is now supported by evidence for reducing surgical site infection, anastomotic leak, and mortality.
- Bailey and Love's, p. 1382-1384; Pye's Surgical Handicraft, p. 275
Adjuvant and Palliative Therapy
Adjuvant Chemotherapy
- Stage III (Dukes' C): FOLFOX (5-fluorouracil + leucovorin + oxaliplatin) or CAPOX (capecitabine + oxaliplatin) are standard adjuvant regimens
- Stage II: Adjuvant chemotherapy is generally reserved for high-risk features (T4, perineural invasion, obstruction/perforation, <12 lymph nodes examined, poorly differentiated histology)
Metastatic/Palliative (Stage IV)
- Backbone: 5-FU-based regimens (FOLFOX, FOLFIRI)
- Add bevacizumab (anti-VEGF) for KRAS/NRAS/BRAF wild-type
- Add cetuximab or panitumumab (anti-EGFR) only for RAS/BRAF wild-type tumours
- BRAF V600E mutated tumours: targeted therapy with BRAF inhibitor + MEK inhibitor combinations (e.g. encorafenib + binimetinib + cetuximab) now show efficacy per recent network meta-analysis (PMID: 41355781)
- MSI-H/dMMR tumours: pembrolizumab (immune checkpoint inhibitor) is first-line in metastatic setting
- Colonic stenting for obstructing tumours as a bridge to surgery or palliation
Radiotherapy
- More commonly used in rectal cancer due to the pelvic position
- Preoperative chemoradiotherapy reduces local recurrence in stage II-III rectal cancer
- Limited role in colon cancer (mobile, not pelvic-fixed)
Surveillance After Curative Resection
- CEA monitoring every 3-6 months for the first 3 years
- CT chest/abdomen/pelvis annually for 3-5 years
- Colonoscopy at 1 year post-resection, then every 3-5 years to detect metachronous lesions
Key Recent Evidence
A 2025 network meta-analysis in BMJ (PMID: 41355781) evaluating targeted therapy in advanced BRAF-mutated CRC confirms the superiority of BRAF inhibitor combinations over standard chemotherapy in this subgroup. A 2025 systematic review and meta-analysis (PMID: 40079672) confirms benefits of prehabilitation programmes (multimodal exercise/nutrition) before colorectal cancer surgery, particularly relevant in elderly/frail patients.
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | Henry's Clinical Diagnosis and Management by Laboratory Methods | Grainger & Allison's Diagnostic Radiology | Pye's Surgical Handicraft 22nd Ed. | Goldman-Cecil Medicine
CEAP classification
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have comprehensive content from four authoritative sources. Here is the full answer.
CEAP Classification of Chronic Venous Disorders
CEAP was introduced in 1994 and revised in 2004, with the most recent update in 2020 (Lurie F et al., J Vasc Surg Venous Lymphat Disord. 2020;8:342-352). Modelled after the TNM system for cancer, it provides a standardised, reproducible framework for classifying chronic venous disease (CVD) used in clinical decision-making and outcomes research worldwide. The consensus statement was published in 25 journals in 8 languages.
CEAP stands for:
C - Clinical | E - Etiologic | A - Anatomic | P - Pathophysiologic
C - Clinical Classification
The highest applicable descriptor should be used in basic CEAP. Each class carries a suffix indicating symptoms:
- S (symptomatic): aches, pain, tightness, skin irritation, heaviness, muscle cramps
- A (asymptomatic)
| Class | Description |
|---|---|
| C0 | No visible or palpable signs of venous disease |
| C1 | Telangiectasias or reticular veins |
| C2 | Varicose veins |
| C2r | Recurrent varicose veins (added in 2020 revision) |
| C3 | Oedema |
| C4 | Changes in skin and subcutaneous tissue secondary to CVD |
| C4a | Pigmentation (haemosiderin) or eczema (stasis dermatitis) |
| C4b | Lipodermatosclerosis or atrophie blanche |
| C4c | Corona phlebectatica (added in 2020 revision) |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
| C6r | Recurrent active venous ulcer (added in 2020 revision) |
Key additions in the 2020 revision:
- C2r and C6r - explicit recognition of recurrent disease
- C4c (corona phlebectatica) - fan-shaped telangiectasias around the medial/lateral ankle, representing a marker of advanced disease
Example: A symptomatic patient with stasis dermatitis = C4aS
Clinical image of C6 (active venous ulcer):

C6 active venous ulcer - note the surrounding haemosiderin pigmentation (C4a changes) on the gaiter area of the ankle (Current Surgical Therapy 14e)
E - Etiologic Classification
| Code | Meaning |
|---|---|
| Ec | Congenital (present since birth; e.g. Klippel-Trenaunay syndrome, Ehlers-Danlos syndrome, clonal trisomies) |
| Ep | Primary (undetermined cause; valvular incompetence without prior DVT) |
| Es | Secondary - post-thrombotic (previously Es alone; 2020 update splits into Es-intravenous and Es-extravenous) |
| En | No venous etiology identified |
Secondary causes include:
- Intravenous: post-thrombotic syndrome, prior DVT
- Extravenous: extrinsic compression syndromes - May-Thurner syndrome (left common iliac vein compressed by right iliac artery), Nutcracker syndrome (left renal vein compression), trauma, muscle pump dysfunction
A - Anatomic Classification
Identifies which venous segment(s) are affected:
| Code | Segment |
|---|---|
| As | Superficial veins (great saphenous vein, small saphenous vein, tributaries) |
| Ap | Perforating (communicating) veins |
| Ad | Deep veins (femoral, popliteal, iliac, IVC) |
| An | No venous location identified |
Multiple segments may be recorded simultaneously (e.g. As,d = superficial and deep).
P - Pathophysiologic Classification
Describes the underlying haemodynamic mechanism:
| Code | Mechanism |
|---|---|
| Pr | Reflux (valvular incompetence) |
| Po | Obstruction (thrombosis, extrinsic compression) |
| Pr,o | Both reflux and obstruction |
| Pn | No pathophysiology identified |
The degree and duration of venous hypertension (raised ambulatory venous pressure, AVP) determines clinical severity:
- Skin manifestations are uncommon with AVP <35 mmHg
- Skin manifestations are almost certain with AVP >90 mmHg
How to Write a Complete CEAP Description
Using all four components produces a precise clinical descriptor. The format is:
C[class][S/A]; E[code]; A[code(s)]; P[code]
Examples:
| Patient | CEAP |
|---|---|
| Symptomatic patient with stasis dermatitis, primary GSV reflux | C4aS; Ep; As; Pr |
| Varicose veins + swelling + lipodermatosclerosis (single highest C used) | C4b; Ep; As; Pr |
| Symptomatic patient with active ulcer, post-thrombotic deep + perforator reflux and obstruction | C6S; Es; Ap,d; Pr,o |
| Symptomatic patient with stasis dermatitis, primary disease of superficial AND deep veins, reflux | C4aS; Ep; As,d; Pr |
Relationship to Other Scoring Systems
CEAP is a descriptive/diagnostic classification - it is not a severity score. It is complemented by:
- Venous Clinical Severity Score (VCSS): Assesses severity of individual signs and symptoms on a 0-3 scale across 10 domains (pain, varicose veins, oedema, pigmentation, inflammation, induration, ulcers, etc.); useful for longitudinal outcomes research
- Venous Segmental Disease Score (VSDS): Quantifies anatomic extent
- Quality of Life (QoL) instruments: CIVIQ, VEINES-QOL
CEAP is the correct diagnostic label; VCSS and QoL scores are the correct instruments for tracking treatment outcomes over time.
Diagnostic Investigation
The principal test supporting CEAP classification is venous duplex ultrasonography, which:
- Detects venous obstruction (absence of flow, echogenic thrombus, non-compressibility)
- Detects venous reflux (prolonged reversal of flow on Valsalva or compression-release manoeuvre)
- Establishes the E, A, and P descriptors
MR venography, CT venography, and conventional venography are reserved for suspected proximal obstruction (iliac/IVC), May-Thurner syndrome, or IVC filter occlusion.
Clinical Application and Treatment by CEAP Stage
| CEAP | Management |
|---|---|
| C0-C1 | Reassurance, lifestyle advice; compression stockings if symptomatic |
| C2 | Compression (20-30 mmHg); endovenous ablation (EVLA, RFA), foam sclerotherapy, or surgery |
| C3 | Graduated compression 20-30 mmHg; treat underlying incompetence |
| C4a-C4b | Graduated compression; treat underlying reflux to prevent progression |
| C5-C6 | Compression 30-40 mmHg is standard of care; wound care; treat incompetent veins to promote/sustain healing; HIPEC or other advanced wound-care options for recalcitrant ulcers |
Sources: Fischer's Mastery of Surgery 8th Ed. | Current Surgical Therapy 14th Ed. | Harrison's Principles of Internal Medicine 22nd Ed. (2025) | Dermatology 2-Volume Set 5th Ed. (Bolonia) | Lurie F et al. 2020 CEAP Update, J Vasc Surg Venous Lymphat Disord.
BBD
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a comprehensive answer. Let me compile it.
Benign Breast Disease (BBD)
Nomenclature and Concept
The older terminology - fibrocystic disease, fibroadenosis, fibrocystic mastopathy, mastitis - was confusing because these terms did not correlate with clinical or histological findings. The modern framework, developed by the Cardiff Breast Clinic, reconceptualises most benign breast conditions as:
ANDI - Aberrations of Normal Development and Involution
This framework holds that most benign breast disorders represent minor deviations from the normal physiological processes of breast development, cyclical hormonal change, and involution - rather than distinct disease entities. The pathogenesis extends on a spectrum from normal variation to clinical disorder to frank disease.
- Bailey and Love's Short Practice of Surgery 28th Ed., p. 940
- Schwartz's Principles of Surgery 11th Ed.
ANDI Classification
| Phase | Age (yrs) | Normal Process | Disorder | Disease |
|---|---|---|---|---|
| Early reproductive | 15-25 | Lobular development; stromal development; nipple eversion | Fibroadenoma; adolescent hypertrophy; nipple inversion | Giant fibroadenoma; gigantomastia; subareolar abscess; mammary duct fistula |
| Later reproductive | 25-40 | Cyclical changes of menstruation | Cyclical mastalgia; nodularity | Incapacitating mastalgia |
| Involution | 35-55 | Lobular involution; duct involution (dilatation, sclerosis); epithelial turnover | Macrocysts; sclerosing lesions; duct ectasia; nipple retraction; epithelial hyperplasia; bloody nipple discharge | Periductal mastitis; epithelial hyperplasia with atypia |
The key concept: the breast unit affected is the Terminal Duct Lobular Unit (TDLU). Oestrogen and progesterone act as growth factors on its epithelial and stromal cells through every menstrual cycle.
- Schwartz's Principles of Surgery, Table 17-2
Pathological Classification (Page's System) and Cancer Risk
Benign breast lesions are classified into three clinically important groups based on their malignant potential:
Group 1 - Nonproliferative Lesions (No increased cancer risk)
Accounts for ~70% of benign breast conditions.
- Cysts (micro and macro) and apocrine metaplasia
- Duct ectasia
- Mild ductal epithelial hyperplasia (<4 cell layers, not crossing the lumen)
- Calcifications (epithelial-related)
- Simple fibroadenoma
- Mastitis, fibrosis, squamous/apocrine metaplasia
- Columnar cell lesions, fat necrosis
Group 2 - Proliferative Lesions Without Atypia (RR 1.5-2.0×)
- Moderate/florid ductal hyperplasia (>4 cell layers, crosses lumen, RR 1.8)
- Sclerosing adenosis (RR 1.7-2.1)
- Radial scar (RR 1.8; upstaging rate 3-40% - requires biopsy)
- Complex sclerosing lesion (RR 2.6; surgical excision recommended)
- Intraductal papilloma - solitary (RR 2.1); peripheral papillomatosis (RR 3.0-3.5)
- Complex fibroadenoma (RR 1.2-2.2)
Group 3 - Proliferative Lesions With Atypia (RR 4-5×)
- Atypical Ductal Hyperplasia (ADH) - RR 4-fold; if extensive (>2 ducts or >2 mm): RR 7-fold
- Atypical Lobular Hyperplasia (ALH) - RR 4-fold
- LCIS - RR 10-fold (marker lesion, not a direct precursor)
- DCIS - RR 10-fold (true precursor, requires treatment)
Key distinction: ADH is defined as features of low-grade DCIS involving fewer than two ducts or measuring <2 mm. When two or more ducts are involved or the lesion exceeds 2 mm, the lesion is reclassified as DCIS.
Cancer Risk Table (Dupont & Page, NEJM 1985)
| Lesion | Relative Risk |
|---|---|
| Nonproliferative lesions | No increase |
| Sclerosing adenosis / intraductal papilloma | No increase |
| Florid hyperplasia | 1.5-2× |
| ADH / ALH | 4× |
| ADH with ductal involvement | 7× |
| LCIS / DCIS | 10× |
Histology of Fibrocystic Changes
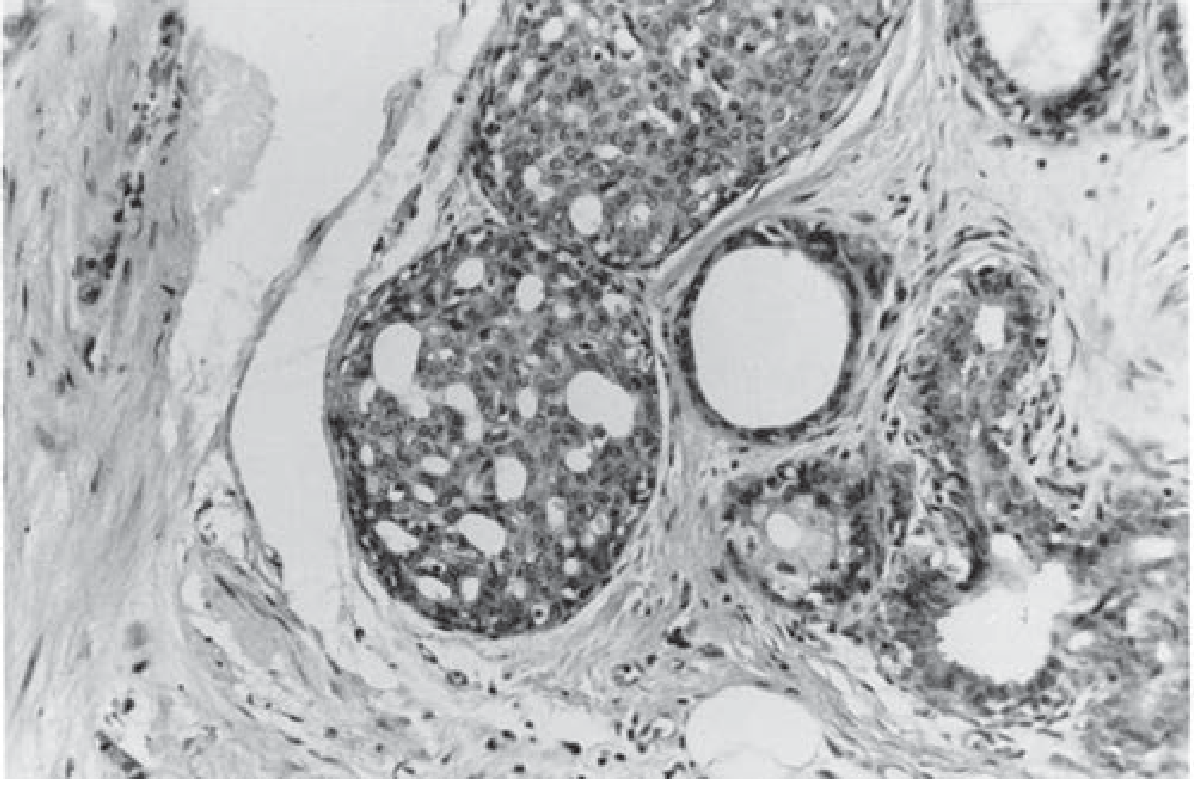
Fibrocystic changes - H&E showing cystic dilatation of terminal ducts/lobules with surrounding fibrous stroma (Schwartz's Principles of Surgery)
Individual Conditions
1. Mastalgia (Breast Pain)
- Affects 50-70% of women presenting to a breast clinic
- Classified as:
Cyclical mastalgia (most common)
- Begins around day 14, peaks at days 27-28, relieved by menses
- Both breasts involved; upper outer quadrant predominance
- Severity measured on Visual Analogue Scale (VAS 0-10)
- Severe forms disrupt sleep and daily activities
Non-cyclical mastalgia
- No relation to menstrual cycle; may be unilateral, localised
- Often associated with duct ectasia or periductal mastitis
- Must exclude referred pain: musculoskeletal (Tietze syndrome), cervical spondylosis, oesophageal reflux, cardiac pain
Management of mastalgia:
| Step | Treatment |
|---|---|
| First | Reassurance (>85% respond); breast pain chart to confirm pattern; well-fitting bra support; evening primrose oil (GLA) |
| Second | Danazol (100-200 mg/day) - most effective; side effects: androgenic (weight gain, acne, irregular menses) |
| Third | Bromocriptine (dopamine agonist, reduces prolactin) - GI side effects common |
| Third | Tamoxifen (10-20 mg/day) - effective; avoid in women trying to conceive |
| Local | Trigger point injection: triamcinolone + lidocaine for non-cyclical localised pain |
2. Fibroadenoma
- Most common discrete breast lump in women under 30; peak incidence 15-25 years
- Arises from aberrant lobular development; oestrogen-dependent
- Clinical features: smooth, firm, rubbery, highly mobile ("breast mouse"), well-circumscribed, non-tender
- Histology: biphasic tumour - epithelial (glandular) and stromal (fibrous) components; two patterns:
- Intracanalicular: stroma compresses ducts into slits
- Pericanalicular: stroma surrounds open, round ducts
- Giant fibroadenoma: >5 cm; common in adolescents and in African women
- Risk: simple fibroadenoma carries no significant increased cancer risk; complex fibroadenoma RR 1.2-2.2×
Management:
- Young women (<25 yrs): ultrasound + reassurance if confident diagnosis; biopsy may not be needed if ultrasound features pathognomonic
- Core-needle biopsy for confirmation in older women
- Options: observation (many regress spontaneously, especially <2 cm), cryoablation, ultrasound-guided vacuum-assisted biopsy, or surgical excision
- Lesions >3 cm are generally best excised
3. Breast Cysts
- Most common nonproliferative breast lesion; peak incidence 35-50 years
- Arise from TDLU when fluid accumulates due to distension and obstruction of efferent ductule
- Three types on ultrasound:
- Simple: anechoic, well-circumscribed, posterior acoustic enhancement - no malignant potential
- Complicated: homogeneous internal echoes, no solid component
- Complex: solid component or thick internal septations - may harbour malignancy; requires biopsy
Management:
- Fine-needle aspiration (21G needle, 10 mL syringe): typical cyst volume 5-75 mL
- If fluid is non-bloodstained and no residual mass: discard fluid (cytology not cost-effective)
- If fluid is bloodstained or residual mass remains: send for cytology; core biopsy; pneumocystogram may help assess cyst wall
- Aspiration now usually performed under ultrasound guidance
4. Sclerosing Adenosis
- Disorder of both proliferative and involutional phases
- Mimics carcinoma on clinical examination, mammography, and gross pathology
- Histologically: distorted, compressed lobular units with increased acini and dense fibrous stroma
- No increased cancer risk per Schwartz; RR 1.7-2.1 per Fischer's
- Management: excisional biopsy often necessary to exclude carcinoma
5. Duct Ectasia and Periductal Mastitis
- Duct ectasia: dilatation of the major subareolar ducts with periductal fibrosis; common in women >50 years; may cause thick, green/brown nipple discharge, nipple retraction
- Periductal mastitis: inflammation around ducts; associated with smoking (nicotine damages subareolar duct epithelium); more common in younger women
- May present as: subareolar mass/abscess, nipple discharge, nipple retraction, mammary duct fistula
- Periductal mastitis is not a puerperal (lactational) abscess - it occurs in non-lactating women and is more prone to recurrence and fistula formation
Management:
- Antibiotics covering anaerobes (polymicrobial); combination therapy
- Ultrasound-guided aspiration of abscess if present
- Surgery: for recurrent/non-resolving cases; total duct excision (Hadfield's procedure) is definitive; duct fistula requires fistulotomy or excision of fistulous tract
6. Intraductal Papilloma
- Benign papillary growth within a lactiferous duct; composed of fibrovascular core with epithelial and myoepithelial lining
- Solitary papilloma: usually in a major subareolar duct; presents with serosanguineous or bloodstained nipple discharge from a single duct orifice; RR 1.5-2.0 (some sources: 2.1)
- Papillomatosis: 5+ papillomas in multiple peripheral ducts; bilateral distribution; RR 3.0-3.5; surgical excision recommended
- Juvenile papillomatosis ("Swiss cheese disease"): multiple firm palpable nodules in young women; contains papillomas, apocrine cysts, ductal hyperplasia; positive family history of breast cancer increases lifetime cancer risk
- Management: microdochectomy (excision of the involved duct) for solitary papilloma; total duct excision for papillomatosis or multiple duct involvement
7. Radial Scar / Complex Sclerosing Lesion
- Radial scar: stellate lesion with a fibroelastic core and entrapped ducts/lobules; mimics carcinoma on mammography (spiculated mass)
- RR 1.8; upstaging to cancer on excision: 3-40%
- Complex sclerosing lesion (>1 cm): RR 2.6; surgical excision recommended
- Management: vacuum-assisted core biopsy or open surgical excision
8. Phyllodes Tumour
- Rare fibroepithelial tumour similar to fibroadenoma but with more cellular stroma
- Spectrum: benign - borderline - malignant
- Distinguished from fibroadenoma by stromal hypercellularity, mitotic activity, and leaf-like architecture on histology
- Benign phyllodes: no increased cancer risk but wide local excision is required (clear margins) due to risk of local recurrence; not amenable to observation alone
Risk Stratification and Surveillance Summary (Fischer's Mastery of Surgery)
| Category | Lesion | Relative Risk | Management | Surveillance |
|---|---|---|---|---|
| Nonproliferative | Usual duct hyperplasia, cysts, simple fibroadenoma, columnar cell lesion | 1.2-1.4 | Observation | Annual CBE + mammogram |
| Benign phyllodes, PASH, fat necrosis | 1.0 | Surgical consultation/excision | Annual CBE + mammogram | |
| Proliferative without atypia | Moderate/florid hyperplasia, sclerosing adenosis | 1.7-2.1 | Observation | Annual CBE + mammogram |
| Radial scar | 1.8 | Observation if adequate sample; excision if atypia | Annual CBE + mammogram | |
| Solitary papilloma | 2.1 | Surgical consultation if >10 mm | Annual CBE + mammogram | |
| Peripheral papillomatosis | 3.0-3.5 | Surgical consultation + excision | CBE q6-12 mo; annual mammogram + consider MRI/US | |
| Atypical | Flat epithelial atypia | 2.0 | Surgical consultation | CBE q6-12 mo; annual mammogram + consider MRI/US |
| ADH / ALH | 4-5× | Surgical consultation + excision | CBE q6-12 mo; annual mammogram + MRI | |
| High-risk | LCIS | 10× | Consider chemoprevention (tamoxifen/raloxifene) | Intensive surveillance or risk reduction surgery |
Triple Assessment
Any breast lump requires triple assessment to exclude malignancy:
- Clinical examination - character of lump, axillary nodes, skin changes
- Imaging - ultrasound (preferred <35 yrs); mammography (preferred ≥35 yrs); MRI for high-risk women
- Pathology - fine-needle aspiration cytology (FNAC) or core-needle biopsy (CNB) - CNB preferred as it gives histological architecture and receptor status
Only when all three components are concordantly benign can the patient be safely discharged or observed.
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | Schwartz's Principles of Surgery 11th Ed. | Fischer's Mastery of Surgery 8th Ed. | Mulholland and Greenfield's Surgery 7th Ed. | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.