Decompression sickness
Reading File
Finding Sources
Searching PubMed
"decompression sickness" treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Decompression Sickness (DCS)
Definition
Decompression sickness refers to a spectrum of clinical illnesses caused by the formation of inert gas bubbles (primarily nitrogen) in blood and tissues during or after ascent from a compressed-gas environment. It can affect divers breathing compressed air, caisson workers, high-altitude pilots, and astronauts during extravehicular activity. - Rosen's Emergency Medicine, p. 2812
Pathophysiology
When breathing at elevated ambient pressure, increased amounts of inert gas (nitrogen when breathing air) dissolve into blood and tissues. The rate of uptake and washout depends on tissue blood flow and the blood-tissue partition coefficient. During ascent, if the rate of gas washout does not match the rate of decline in ambient pressure, the sum of dissolved gas pressures in tissues exceeds ambient pressure - a state called supersaturation. This is the prerequisite for bubble formation. - Harrison's Principles of Internal Medicine 22E, p. 3810
Once formed, bubbles cause harm via two broad mechanisms:
- Mechanical obstruction - direct blockage of blood flow, ischemia, and disruption of pain-sensitive or functionally important structures
- Inflammatory/coagulation cascades - the air-blood and air-endothelial interfaces activate complement, cytokines, platelet aggregation, neutrophil adhesion, and endothelial permeability, leading to third spacing of fluids and hemoconcentration. Circulating microparticles (membranous vesicles extruded from vascular endothelial cells under decompression stress) are also implicated as injurious agents. - Tintinalli's Emergency Medicine, p. 3326
Nitrogen is highly fat-soluble, making the myelinated white matter of the CNS particularly vulnerable. Small, asymptomatic venous gas emboli after ascent are very common and are usually filtered in the pulmonary capillaries without harm. It is only when bubble load exceeds a threshold that symptoms appear. - Rosen's Emergency Medicine, p. 2812
Patent foramen ovale (PFO) - present in ~25% of adults - is a major risk factor. It allows venous bubbles to enter the arterial circulation, increasing risk of cerebral, spinal cord, inner ear, and cutaneous DCS. 65% of divers with serious DCS have a PFO. - Rosen's Emergency Medicine, p. 2812
Epidemiology & Risk Factors
- Incidence: approximately 1 in 5,000-10,000 recreational dives (some estimates as low as 1/1,000 to 1/20,000 depending on population studied)
- Risk is 2.5× greater in men than women
- Risk increases with: depth, duration, repetitive dives, age, obesity, dehydration, fatigue, fever, cold ambient temperatures after diving, flying soon after diving, high-altitude diving
- DCS can occur even when dive tables or computer limits are strictly followed
Timing of symptoms: ~40% occur within 1 hour of surfacing; 60% within 3 hours; 80% within 8 hours; 98% within 24 hours. Symptoms arising >24 hours post-dive are very unlikely to be DCS unless the diver subsequently ascended to altitude (e.g., air travel). - Rosen's Emergency Medicine, p. 2812
Classification
Type I - "Pain-only" DCS (Less Severe)
- Deep aching pain in joints and extremities, especially shoulders and elbows - unrelieved but not worsened with movement
- Skin changes: pruritus, mottling, color changes
- Lymphatic obstruction causing localized edema (takes days to resolve)
- Note: Cutis marmorata (patchy cyanotic marbling of the skin, shown below) was previously classified as Type I, but recent evidence suggests it reflects CNS-related changes in vasomotor regulation and is now considered more closely related to Type II DCS

Type II - Serious DCS (Neurological, Vestibular, Pulmonary)
Spinal cord (most common CNS site in compressed air diving):
- Limb weakness or paralysis, paresthesias, numbness
- Low back and abdominal pain; "girdle pain" (often portends spinal cord involvement)
- Distal prickly sensations advancing proximally
- Urinary retention, bladder/fecal incontinence, priapism
- Patchy or unequally distributed sensory/motor findings (unlike spinal cord trauma)
Cerebral:
- Headache, blurred vision, diplopia, dysarthria, unusual fatigue, inappropriate behavior, dizziness
- Loss of consciousness is rare in DCS (in contrast to arterial gas embolism)
Inner ear - "The Staggers":
- Vertigo, ataxia, nausea/vomiting, hearing loss, tinnitus
- ~1/3 of DCS patients report cochlear or vestibular symptoms
Pulmonary - "The Chokes" (serious):
- Progressive dyspnea, cough (may become paroxysmal), chest pain
- Cyanosis, hypotension, elevated CVP and pulmonary arterial pressure
- May progress to respiratory arrest
Cardiovascular:
- Hemoconcentration, coagulopathy, hypotension
The term Decompression Illness (DCI) is now commonly used to encompass Type I DCS, Type II DCS, and arterial gas embolism (AGE), since all require recompression treatment. - Rosen's Emergency Medicine, p. 2813
Symptom Frequency
From 2,346 recreational diving accidents (Divers Alert Network data):
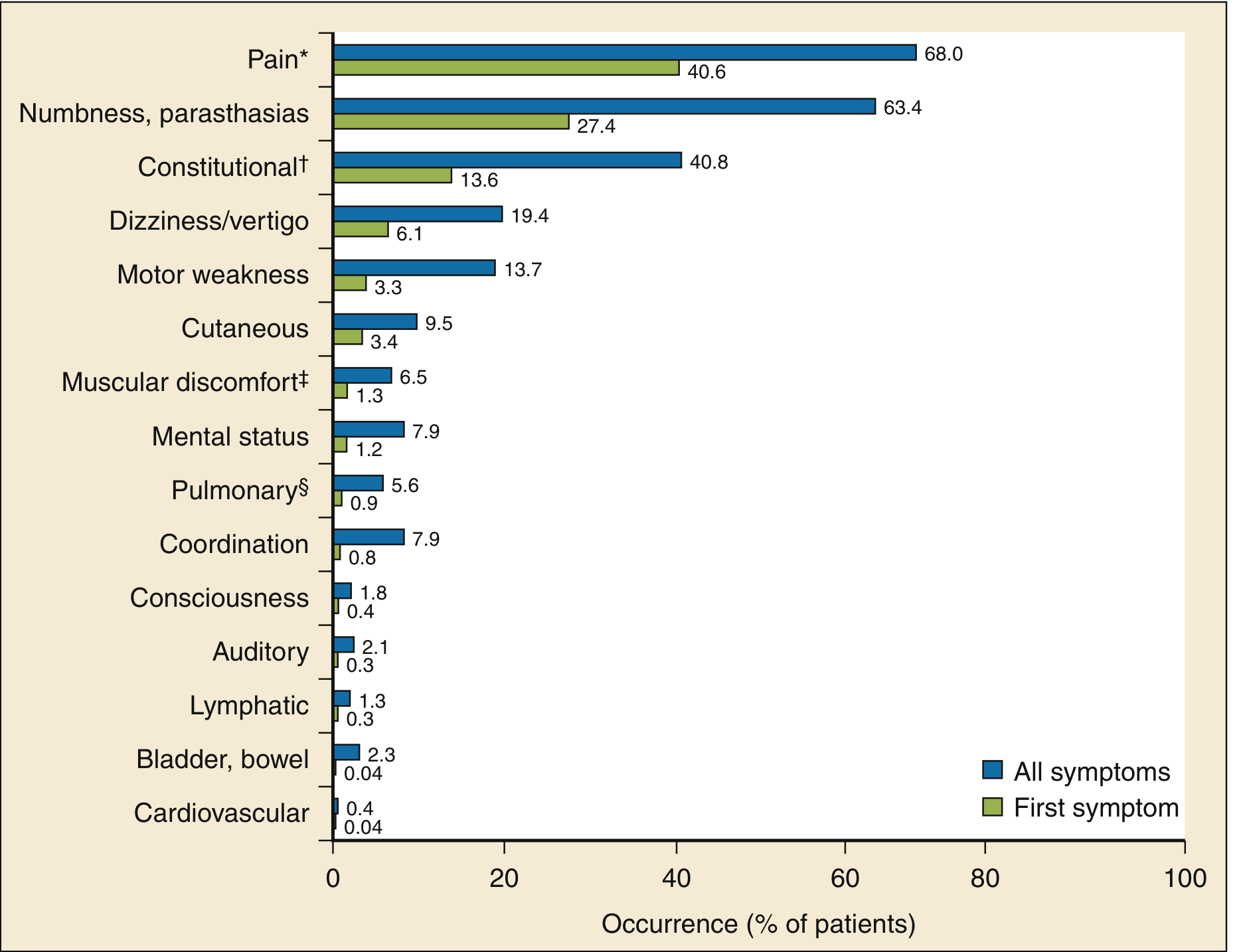
Fig. Classification of initial and all eventual DCS manifestations - Rosen's Emergency Medicine, Fig. 131.7
Pain (68%) and numbness/paresthesias (63.4%) are the dominant overall symptoms. Constitutional symptoms include headache, lightheadedness, fatigue, malaise, nausea, and anorexia.
Diagnosis
There is no reliable confirmatory diagnostic test. Diagnosis rests on:
- A compatible dive profile (depth, duration, compliance with tables)
- Temporal relationship of symptoms to diving
- Clinical examination findings
The blood pressure cuff test (inflating a cuff to 150-200 mmHg over an affected joint relieves pain) can help confirm Type I DCS, but sensitivity is as low as 60%.
Distinguishing DCS from arterial gas embolism (CAGE) can be clinically difficult, but the distinction is largely unimportant because first aid and definitive management are identical. - Harrison's 22E, p. 3810
Treatment
First Aid (Immediate)
- Horizontal positioning (lateral decubitus if consciousness is impaired)
- 100% oxygen - accelerates inert gas washout and promotes bubble resolution
- IV fluids - preferably glucose-free isotonic saline (oral if patient is conscious and IV unavailable)
- Do NOT delay evacuation for recompression
Definitive Treatment - Hyperbaric Oxygen (HBO) Recompression
- Mechanism: Recompression reduces bubble volume (Boyle's law), while simultaneous 100% oxygen administration greatly increases the inert gas partial pressure gradient from bubble to tissue to blood, dramatically accelerating bubble resolution. Hyperbaric oxygen also oxygenates ischemic tissue and reduces proinflammatory effects.
- Recompression begins with oxygen at 2.8 ATA (maximum pressure with acceptable oxygen toxicity risk)
- Most widely used protocol: U.S. Navy Table 6 (shortest format: 4 hours 45 minutes), followed by stepwise decompression adjusted to symptom response
- Repeat daily sessions while symptoms persist and respond to treatment
- Adjuncts: IV fluids, supportive care as needed
Mild/Marginal DCS
- Some cases may be managed with first aid alone, particularly when recompression evacuation is extremely hazardous - but this decision requires experienced diving physicians
- Long-distance evacuations: prefer helicopter at low altitude or fixed-wing aircraft pressurized to 1 ATA; do not delay serious cases for this
Special Consideration: Pregnancy
- No safe dive tables exist for the fetus - the fetal circulation (foramen ovale, ductus arteriosus) bypasses the pulmonary filter, allowing venous bubbles to enter fetal arterial circulation
- Diving is associated with low birth weight, prematurity, congenital malformations, and stillbirth
- Pregnant women should be advised not to scuba dive - Rosen's Emergency Medicine, p. 2813
Recent Evidence
A 2026 systematic review on inner ear DCS found that hyperbaric oxygen therapy improves outcomes, supporting its use even in isolated inner ear presentations. Stokes et al., 2026 (PMID: 41875444) - no major contradictions to existing management guidelines.
Sources: Rosen's Emergency Medicine (9th ed.) | Tintinalli's Emergency Medicine (9th ed.) | Harrison's Principles of Internal Medicine 22E (2025) | Divers Alert Network data
This is a shared conversation. Sign in to Orris to start your own chat.