The pain is originating from the medial side of the armpit and running down all the way to the palm of my hand what could it be?
Reading File
Finding Sources
Finding Sources
Searching the Web
medial armpit pain radiating down arm to palm ulnar nerve thoracic outlet syndrome
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Here is a thorough breakdown of what your symptom pattern most likely represents:
Pain from Medial Armpit to Palm - What Could It Be?
The path you describe - medial (inner) side of the armpit running all the way down to the palm - follows the medial cord of the brachial plexus and the structures derived from spinal levels C8 and T1. This is a well-recognized anatomical territory. The brachial plexus diagram below illustrates exactly which structures are involved:
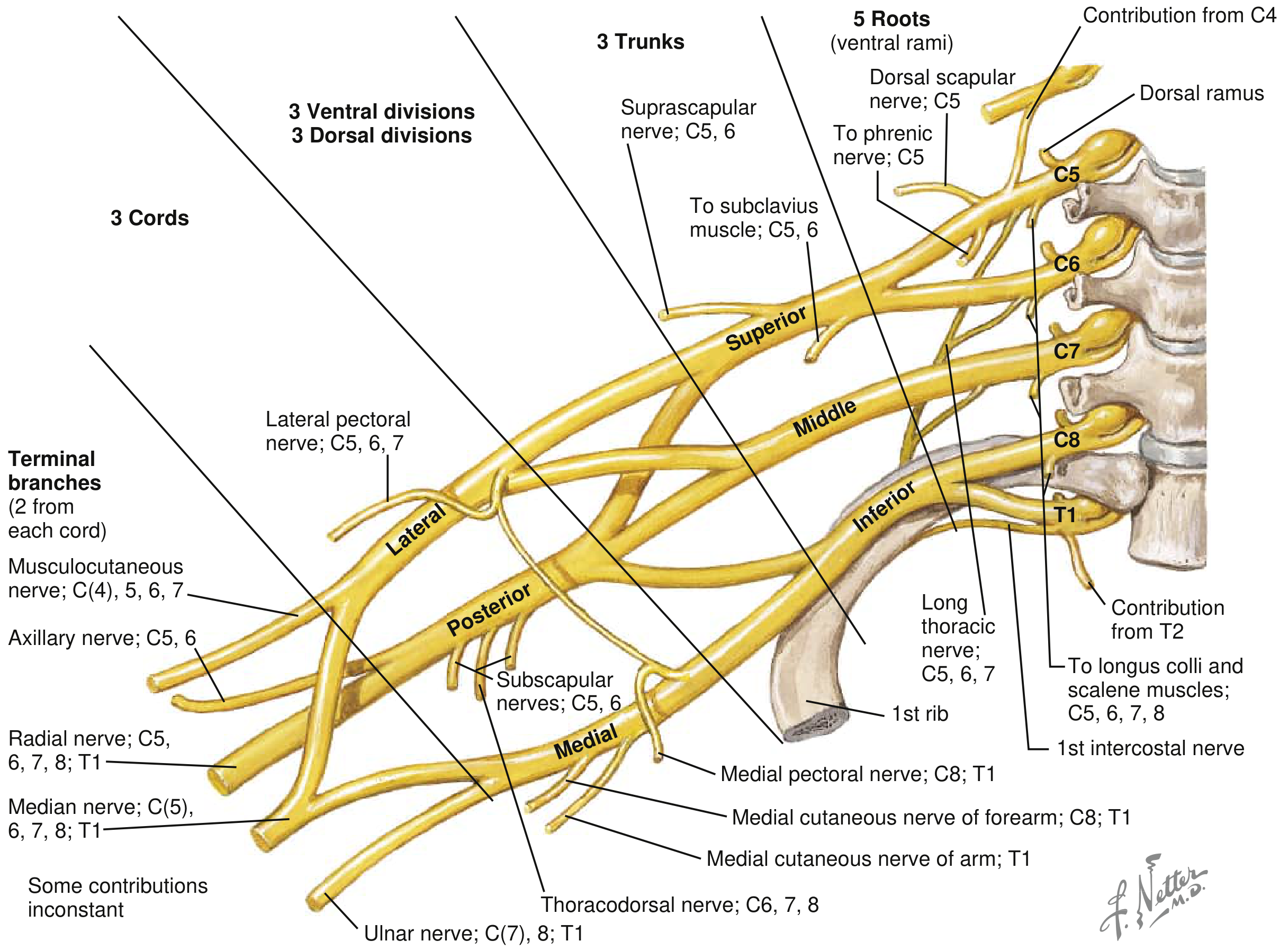
The medial cord gives off the medial cutaneous nerve of the arm (T1), the medial cutaneous nerve of the forearm (C8/T1), and continues as the ulnar nerve (C7/C8/T1) - all of which cover exactly the route you describe.
Most Likely Causes (from most to least common)
1. Ulnar Nerve Entrapment (Cubital Tunnel Syndrome) - Most Common
The ulnar nerve runs along the medial side of the upper arm, passes through the "funny bone" groove at the elbow, and travels to the medial palm and the ring/little fingers. Entrapment here causes:
- Pain and numbness radiating from the inner elbow area down to the palm
- Tingling in the ring and little fingers
- Symptoms worse when sleeping with the elbow bent or resting the elbow on hard surfaces
- Tapping the nerve at the elbow produces a "electric" tingling (positive Tinel sign)
As stated in Bradley and Daroff's Neurology in Clinical Practice: "Ulnar nerve entrapment triggers numbness or pain radiating down the medial aspect of the arm to the little and ring fingers. Symptoms are often worse at night when the patient sleeps with a flexed elbow."
2. Thoracic Outlet Syndrome (TOS)
This occurs when nerves and/or blood vessels are compressed between the collarbone and first rib, right at the axilla (armpit) level. According to Localization in Clinical Neurology, 8e: "Usually, the lower trunk or medial cord of the brachial plexus is involved. Pain is the most common sensory symptom, is often intermittent, and is referred to the ulnar border of the hand and the medial forearm and arm."
Key features:
- Pain in the posterior shoulder and pectoral region, radiating down the inner arm to the hand
- Paresthesias primarily in the ring and little fingers (ulnar distribution - over 90% of neurogenic TOS cases)
- Symptoms worsen with overhead arm movements, carrying heavy bags, or prolonged arm elevation
- Can also cause coldness, color changes, or swelling in the hand (if blood vessels involved)
- More common in young-to-middle-aged women, often with a droopy/sloping shoulder posture
Causes include cervical ribs, tight scalene muscles, and fibrous bands near the first rib.
3. C8 Nerve Root Compression (Cervical Radiculopathy at C7-T1)
A herniated disc between C7 and T1 vertebrae compresses the C8 nerve root and closely mimics ulnar nerve palsy. Per Adams and Victor's Principles of Neurology: "Compression of the eighth cervical root (by a C7-T1 disc) may mimic ulnar nerve palsy. The pain is along the medial side of the forearm and the sensory loss is in the distribution of the medial cutaneous nerve of the forearm and of the ulnar nerve in the hand."
Key distinguishing features:
- Often accompanied by neck pain that radiates into the arm
- Pain may worsen with neck movements (especially extension/rotation to the affected side)
- Weakness of intrinsic hand muscles
4. Pancoast Tumor (Apical Lung Tumor)
Less common but important - a tumor at the top of the lung can compress the lower brachial plexus (C8/T1) from below, causing severe medial arm and hand pain, often with:
- Weakness and wasting of small hand muscles
- Drooping eyelid on the same side (Horner syndrome: ptosis + miosis + anhidrosis)
- This is a red flag that requires urgent evaluation
How to Tell Them Apart
| Feature | Ulnar Entrapment | TOS | C8 Radiculopathy |
|---|---|---|---|
| Pain origin | Elbow area | Armpit/collarbone area | Neck |
| Triggers | Elbow flexion, resting on elbow | Arm elevation, carrying loads | Neck movement, coughing |
| Neck pain | No | No | Yes |
| Fingers affected | Ring + little | Ring + little | Ring + little |
| Tinel at elbow | Positive | Negative | Negative |
Red Flags - See a Doctor Urgently if You Have:
- Progressive weakness of hand muscles
- Muscle wasting (the fleshy mound at base of thumb or little finger shrinking)
- Drooping eyelid on the same side
- Unexplained weight loss or persistent cough (could suggest a Pancoast tumor)
- Swelling, discoloration, or coldness of the hand
What to Do Next
A proper evaluation should include:
- Physical exam - testing grip strength, finger spread, Tinel sign at the elbow and wrist
- Nerve conduction studies (NCS) / EMG - to localize exactly where the nerve is compressed
- Cervical spine MRI if radiculopathy is suspected
- Chest X-ray if TOS or Pancoast tumor is suspected
This pattern of pain is very recognizable clinically and is usually treatable once the source is found. The most common culprit by far is ulnar nerve entrapment at the elbow - simple measures like avoiding elbow-bending at night and using elbow pads often bring significant relief.
Disclaimer: This is educational information, not a diagnosis. Please see a physician or neurologist for a proper evaluation - especially if you have weakness, muscle wasting, or the red flags listed above.
This is a shared conversation. Sign in to Orris to start your own chat.