Anatomy of female pelvic
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Excellent - a superb Netter-style superior view of the female pelvis. I now have comprehensive content from two authoritative textbooks plus three detailed anatomical images. Let me compile the complete answer.
Anatomy of the Female Pelvis
Sources: Campbell-Walsh-Wein Urology (surgical anatomy chapter) and THIEME Atlas of Anatomy: General Anatomy and Musculoskeletal System
1. Bony Pelvis
The foundation of female pelvic anatomy is the bony pelvis, divided into the true pelvis (lesser pelvis) and the false pelvis (greater pelvis), separated by the pelvic brim (linea terminalis).
The true pelvis contains four bones:
- Two innominate bones (each = ilium + ischium + pubis)
- Sacrum
- Coccyx
Female-specific features that distinguish it from the male pelvis:
- Larger and broader with sides wider apart
- Oval inlet (vs. heart-shaped in males) - wider but mechanically weaker
- Obtuse angle between the inferior pubic rami (subpubic angle >90°)
- Shorter, wider sacrum with a less prominent sacral promontory
- Ischial spines project less medially - key surgical landmark for apical suspension sutures
The ischial spine is an important landmark during vaginal prolapse surgery (identifying safe locations for fixation sutures). The pelvic inlet faces anteriorly in the standing position, directing intra-abdominal pressure onto the bony pelvis rather than muscles and fascia.
2. Fascia and Peritoneum
Pelvic fascia is organized into three strata:
| Stratum | Contents |
|---|---|
| Inner | Rectus fascia; covers anterior/lateral rectal wall, vessels, nerves; forms part of Denonvilliers fascia |
| Intermediate | Surrounds uterus and supporting vessels; source of most pelvic organ support via retroperitoneal connective tissue; includes pubovesical and pubocervical fascia |
| Outer | Transversalis fascia, continuous with endopelvic and lateral pelvic fascia; includes iliac fascia (covering iliacus + psoas), obturator fascia |
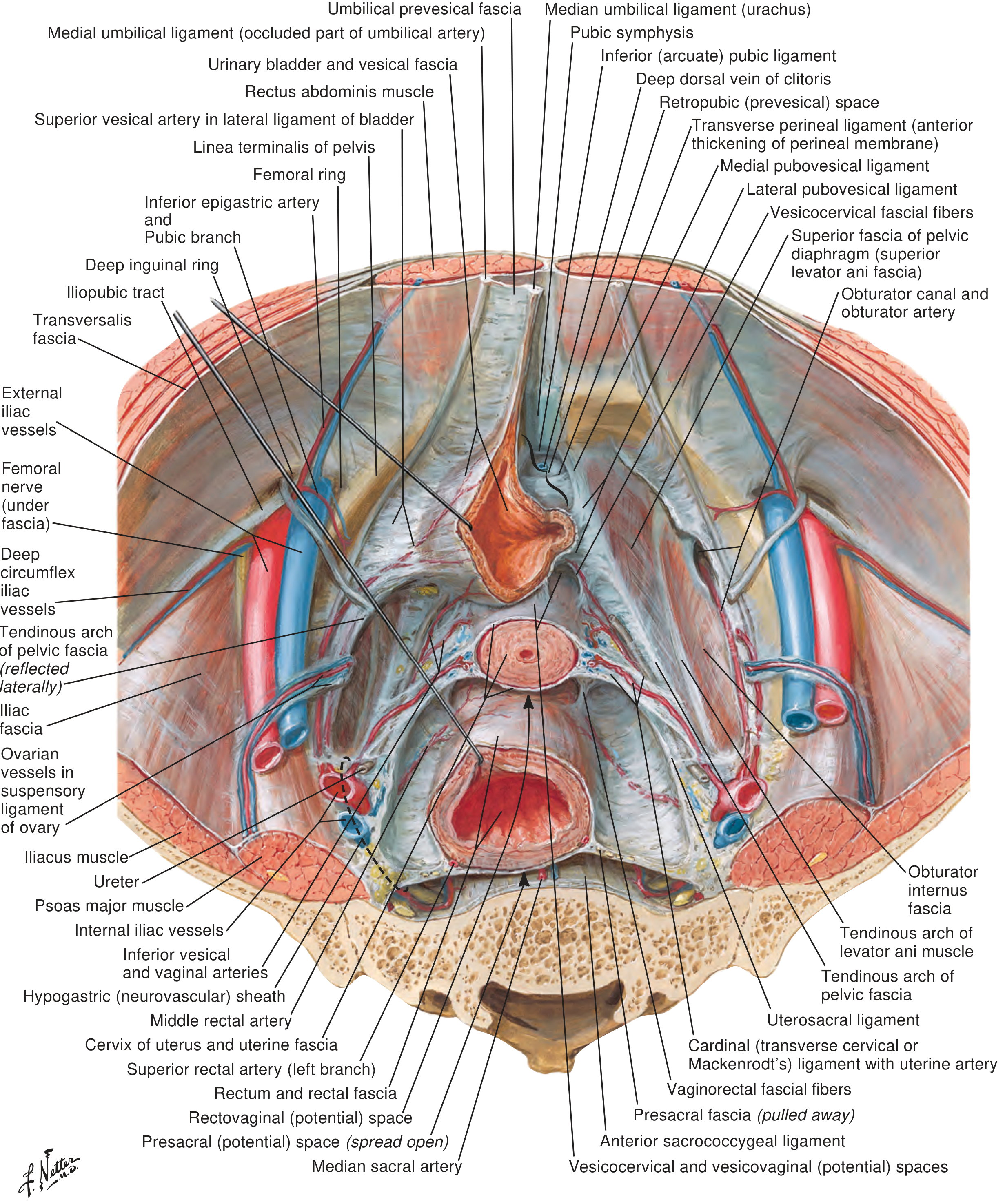
Key fascial structures:
- Arcus tendineus fasciae pelvis (ATFP): thickened band from ischial spine to pubic bone - main point for fascial attachment
- Arcus tendineus levator ani (ATLA): aponeurotic portion of obturator fascia where levator ani attaches
- Parametrium: fascia attached to the uterus
- Paracolpium: fascia surrounding the vagina
- Pubocervical fascia: extends pubic symphysis to cervix, supports bladder base
- Vesicopelvic ligament/fascia: formed by fusion of perivesical and endopelvic fascia; defects cause lateral cystocele
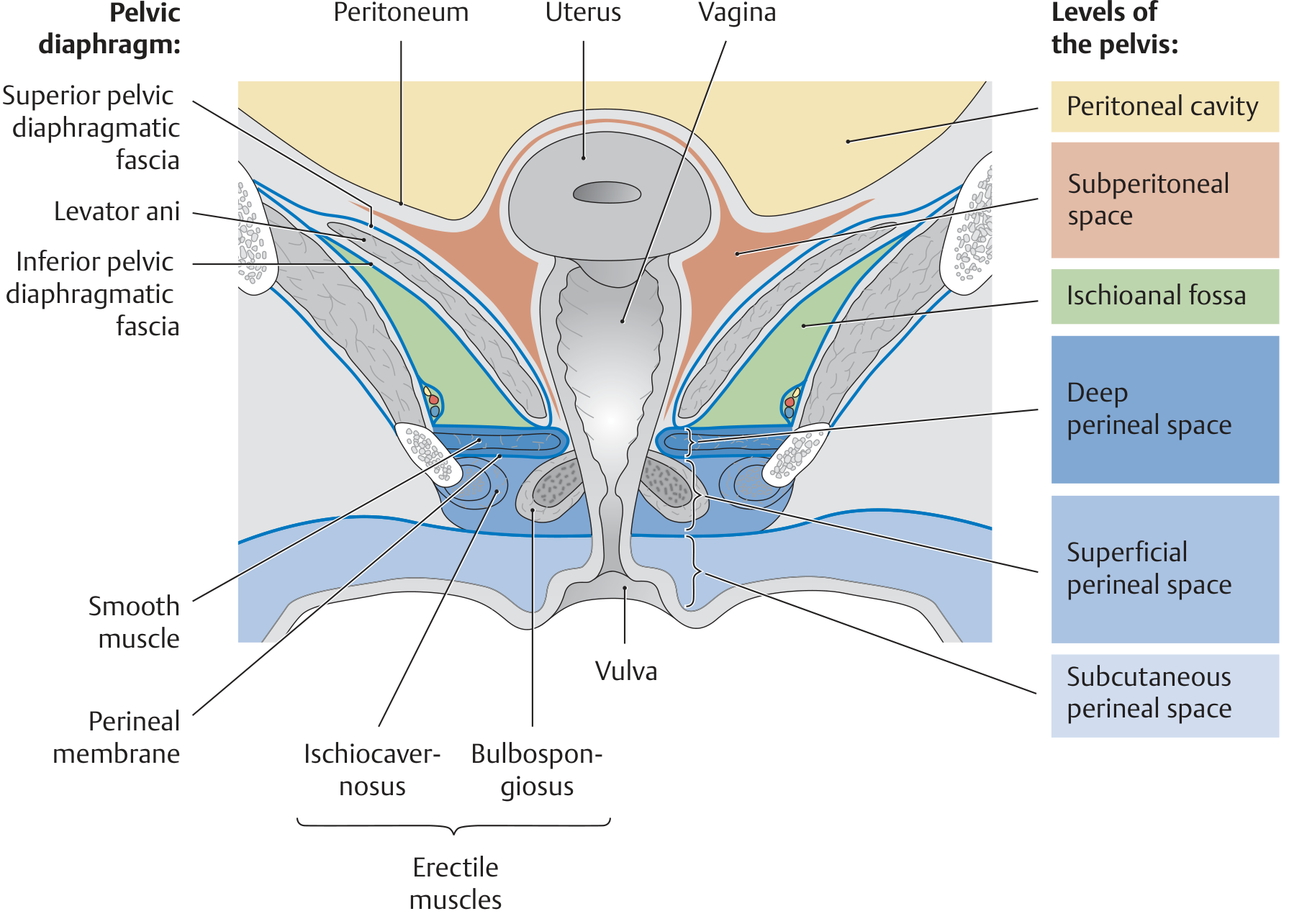
3. Pelvic Spaces
Six potential spaces exist among the female pelvic organs:
- Vesicovaginal space - between bladder adventitia (anterior) and vagina (posterior)
- Rectovaginal space - between rectum and vagina
- Prevesical (retropubic/Retzius) space - between bladder fascia and endopelvic fascia behind the pubis
- Retrorectal space - between rectal fascia and transversalis fascia over the sacrum
- Paravesical spaces (bilateral, lateral to bladder)
- Pararectal spaces (bilateral, lateral to rectum)
Peritoneal pouches:
- Pouch of Douglas (rectouterine pouch): bounded by uterus, posterior vaginal fornix, rectum, and uterosacral ligaments - the most dependent part of the peritoneal cavity
- Vesicouterine pouch: fold of peritoneum reflected from uterus onto bladder at the junction of uterine body and cervix
4. Ligaments of the Pelvis
Bony Ligaments
- Sacrospinous ligament (runs from sacrum/coccyx to ischial spine) - surgical anchor point
- Sacrotuberous ligament
- Short and long dorsal sacroiliac ligaments
- Iliolumbar ligament (L5 to ilium)
- Sacrococcygeal ligament
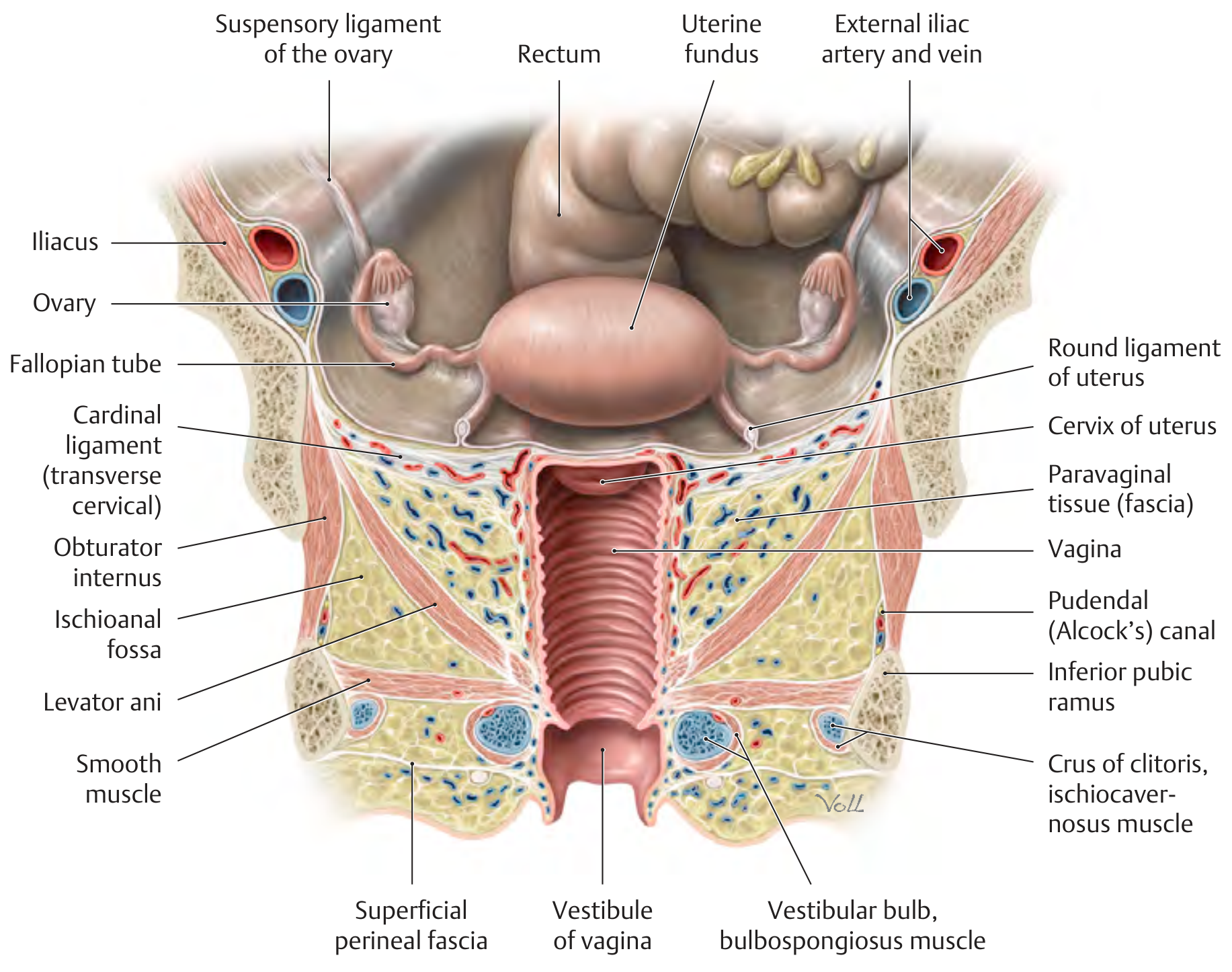
Organ-Supporting Ligaments
- Cardinal (Mackenrodt's / transverse cervical) ligament: provides main horizontal support to uterus and cervix; contains the uterine artery
- Uterosacral ligaments: condensation of endopelvic fascia running from cervix/upper vagina to sacrum; DeLancey Level I support
- Broad ligament: peritoneal fold enclosing fallopian tube and ovary; contains uterine artery, vein, and nerves; does NOT provide significant support
- Round ligament: connects uterine fundus to labia majora via inguinal canal; does NOT provide significant support
- Pubovesical (pubourethral) ligaments: from pubic bone to bladder neck; provide hammock-like support to mid-urethra
5. Pelvic Floor (Pelvic Diaphragm)
The pelvic floor closes the pelvic cavity inferiorly and is organized into three levels of muscle and connective tissue:
Upper Level - Pelvic Diaphragm
The funnel-shaped pelvic diaphragm is the main muscular support. It consists of:
| Muscle | Origin | Insertion | Function |
|---|---|---|---|
| Pubococcygeus | Pubic body | Coccyx / anococcygeal raphe | Supports pelvic viscera; resting tone maintains continence |
| Puborectalis | Pubic body | Forms U-loop around anorectal junction | Maintains anorectal angle; fecal continence |
| Iliococcygeus | ATLA / ischial spine | Coccyx / anococcygeal raphe | Supports pelvic floor |
| Coccygeus (ischiococcygeus) | Ischial spine | Lower sacrum / coccyx | Supports sacrum and pelvic floor |
Together, pubococcygeus + puborectalis + iliococcygeus = levator ani muscle (the most important pelvic floor muscle).
The sustained resting tone of levator ani supports pelvic viscera, resists increases in intra-abdominal pressure, and passively controls urinary and fecal continence.
Middle Level - Deep Urogenital Muscles (Deep Perineal Pouch)
- Deep transverse perineal muscle (note: becomes heavily replaced by connective tissue with aging and after vaginal deliveries)
- External urethral sphincter
Lower Level - Sphincters and Erectile Muscles (Superficial Perineal Pouch)
- Bulbospongiosus
- Ischiocavernosus
- Superficial transverse perineal
- External anal sphincter
6. Pelvic Organs
Uterus
- Pear-shaped muscular organ; ~7.5 cm long
- Divided into fundus, body, isthmus (internal os), and cervix
- Anteverted and anteflexed in most women
- Surrounded by parametrium; supported by cardinal and uterosacral ligaments
Fallopian Tubes
- 10-12 cm long; four parts: interstitial, isthmus, ampulla, infundibulum
- Contained within the broad ligament
Ovaries
- Almond-shaped; ~3 cm x 2 cm x 1 cm
- Attached to broad ligament by mesovarium, to uterus by ovarian ligament, to pelvic wall by suspensory (infundibulopelvic) ligament which carries ovarian vessels
Vagina
- Fibromuscular tube, ~9 cm long in adults
- Upper two-thirds: autonomic innervation from uterovaginal plexus (not sensitive to pain)
- Lower one-fourth: somatic innervation from pudendal nerve (sensitive to touch/temperature)
- Supported at three DeLancey levels (see below)
Bladder
- Extraperitoneal; superior surface covered by peritoneum
- Detrusor muscle under parasympathetic (pelvic splanchnic nerves, S2-S4) control
Urethra
- ~4 cm long, 6 mm diameter in adult females
- Runs anteroinferiorly behind pubic symphysis, embedded in the anterior vaginal wall
- Internal sphincter: smooth muscle, involuntary
- External sphincter (rhabdosphincter): skeletal muscle, under voluntary control
Rectum
- Supported posteriorly by presacral fascia (Waldeyer's fascia)
- The rectovaginal space separates it from the vagina
7. DeLancey's Three Levels of Vaginal Support
A clinically essential framework:
| Level | Structure | What it supports |
|---|---|---|
| Level I | Cardinal + uterosacral ligaments (vertically oriented) | Uterus and vaginal apex |
| Level II | Paravaginal attachments to ATFP (horizontally oriented) | Anterior and posterior vaginal walls |
| Level III | Distal vagina fused to urethra, levator ani, perineal body | Urethra; disruption → urethral hypermobility |
8. Vascular Supply
- Internal iliac (hypogastric) artery - main supply to pelvic organs
- Anterior division: uterine artery, vaginal artery, inferior vesical artery, obturator artery, internal pudendal artery, middle rectal artery
- Posterior division: iliolumbar, lateral sacral, superior gluteal arteries
- Uterine artery: runs in the cardinal ligament; crosses the ureter ("water under the bridge") about 1.5 cm lateral to the cervix - surgically critical
- Ovarian artery: arises from the aorta (at L1-L2); runs in the suspensory ligament
- Venous drainage parallels the arteries into the internal iliac veins
9. Nerve Supply
| Nerve | Type | Structures supplied |
|---|---|---|
| Pudendal nerve (S2-S4) | Somatic | Perineum, external sphincters, lower vagina, clitoris, labia |
| Pelvic splanchnic nerves (S2-S4) | Parasympathetic | Bladder (detrusor contraction), uterus, vagina, erectile tissue |
| Hypogastric nerve (L1-L2) | Sympathetic | Bladder neck/sphincter contraction, uterus, vagina |
| Sacral plexus (L4-S3) | Mixed | Levator ani, pelvic floor muscles |
The ischial spine and sacrospinous ligament are key landmarks during vault suspension to avoid injury to the sacral plexus and pudendal nerve.
10. Key Anatomical Images
Coronal view - pelvic spaces and floor levels (THIEME Atlas):
Anterior view - pelvic organs, ligaments, and neurovascular structures (THIEME Atlas):
Superior view - female pelvis with fascia, ligaments, and vessels removed (Netter-style, Campbell-Walsh-Wein):
Clinical Highlights
- The ureter runs beneath the uterine artery ("water under the bridge") near the cervix - most common site of ureteral injury during hysterectomy
- Pudendal nerve block: administered at the ischial spine (transvaginally or transperineally)
- Pelvic organ prolapse results from levator ani injury/weakness and fascial defects - classified by DeLancey levels
- Stress urinary incontinence is caused by urethral hypermobility (Level III failure) or intrinsic sphincter deficiency
- MRI is the gold standard imaging for female pelvic anatomy; translabial ultrasound is used for dynamic assessment of bladder neck mobility and prolapse
Sources: Campbell-Walsh-Wein Urology, 3-Volume Set - Surgical, Radiographic, and Endoscopic Anatomy of the Female Pelvis (Chapter 108); THIEME Atlas of Anatomy: General Anatomy and Musculoskeletal System - Pelvic Floor and Perineum sections
This is a shared conversation. Sign in to Orris to start your own chat.