Point souce epidemic for psm exam from park
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete exam-ready summary of Point Source Epidemic from Park's Textbook of Preventive and Social Medicine.
Point Source Epidemic - Park's PSM (Exam Notes)
Classification of Epidemics (Park)
Three major types:
A. Common-source epidemics
- (a) Single exposure / "Point-source" epidemics
- (b) Continuous or multiple exposure epidemics
B. Propagated epidemics
- (a) Person-to-person
- (b) Arthropod vector
- (c) Animal reservoir
C. Slow (modern) epidemics
Point-Source Epidemic - Definition
Also called common-source, single-exposure epidemic.
The exposure to the disease agent is brief and essentially simultaneous, and the resultant cases all develop within one incubation period of the disease.
Classic example: Food poisoning outbreak.
Epidemic Curve - Point Source
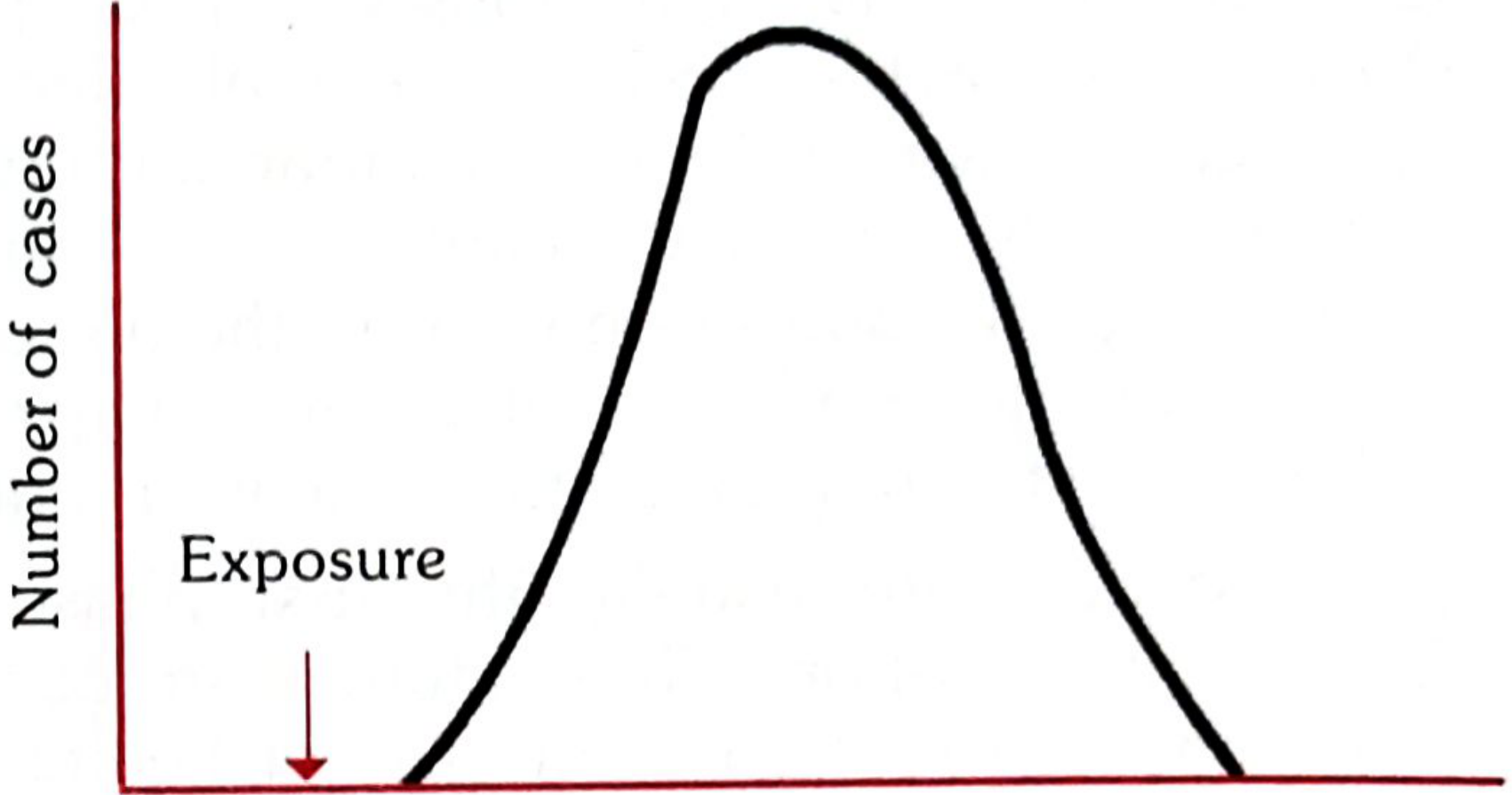
Fig. 4 from Park - Epidemic curve of a point-source epidemic
The curve has one peak and rises and falls within one incubation period.
Key Features (3 Points - High Yield)
| Feature | Detail |
|---|---|
| (i) Rapid rise and fall | Epidemic curve rises and falls rapidly, with no secondary waves |
| (ii) Explosive | Cases cluster within a narrow interval of time |
| (iii) Single incubation period | All cases develop within one incubation period of the disease |
Median Incubation Period
- Defined as the time required for 50% of cases to occur following exposure.
- This is a key point of interest in point-source epidemics - it helps identify the causative agent.
Important Note - Etiology
Common-source epidemics are frequently, but not always, due to infectious agents. They can also result from:
- Contamination of air, water, food, or soil by industrial chemicals or pollutants
- Examples: Bhopal gas tragedy (India), Minamata disease (Japan - methyl mercury in fish)
How Incubation Period Helps Identify Type (Exam Favourite)
From Park:
- Point source epidemic - all cases occur within one incubation period
- Propagated epidemic - cases occur later than the known incubation period (multiple waves/peaks)
What Happens if Epidemic Continues Beyond One Incubation Period?
There is either:
- Continuous or multiple exposure to a common source, OR
- A propagated spread from person to person
Comparison Table - Point Source vs Propagated (High Yield)
| Feature | Point Source | Propagated |
|---|---|---|
| Exposure | Brief, simultaneous | Person-to-person / vector |
| Epidemic curve | Rapid rise, rapid fall, single peak | Gradual rise, slow fall, multiple peaks |
| Duration | Within one incubation period | Extends over multiple incubation periods |
| Secondary waves | Absent | Present |
| Example | Food poisoning, Bhopal gas | Hepatitis A, Polio, COVID-19 |
Continuous/Repeated Exposure (Common-Source Subtype)
When exposure from the same source is prolonged, repeated, or intermittent:
- No explosive rise - more extended or irregular pattern
- Example: Contaminated water supply, nationally distributed food/vaccine
- Classic example: Legionnaire's disease outbreak, Philadelphia, 1976
A mixed pattern is also possible: epidemic starts as point-source (sharp peak) then tails off gradually as propagated - classic example is water-borne cholera.
One-Liner Definitions to Remember
- Point source epidemic = brief simultaneous exposure → all cases in ONE incubation period → single-peak explosive curve, no secondary waves
- Median incubation period = time for 50% of cases to occur after exposure
- Serial interval = time between onset of primary and secondary case (used to estimate incubation period)
Source: Park's Textbook of Preventive and Social Medicine, Chapter on Epidemiology, pp. 77-78
Give me important questions come from epidemiology section as short question
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive coverage of all major epidemiology topics from Park's. Let me compile the complete exam-ready short questions list.
Important Short Questions - Epidemiology (Park's PSM)
SECTION 1: DEFINITIONS & CONCEPTS
Q1. Define Epidemiology
"The study of the distribution and determinants of health-related states or events in specified populations, and the application of this study to the prevention and control of health problems." (John Last, IEA)
- Unit of study = defined population (vs. clinical medicine = individual case)
Q2. Aims of Epidemiology (IEA - 3 aims)
- Describe distribution and magnitude of health/disease in populations
- Identify aetiological factors (risk factors) in pathogenesis
- Provide data for planning, implementation and evaluation of health services
Q3. Epidemiological Triad
Agent + Host + Environment - the three interacting factors that determine disease occurrence. Time is the fourth factor added in the triangle of epidemiology.
SECTION 2: MEASUREMENTS IN EPIDEMIOLOGY
Q4. Rate vs Ratio vs Proportion
| Tool | Definition |
|---|---|
| Rate | Occurrence of an event in a defined population over a given time period. Has a time dimension. e.g., death rate |
| Ratio | Relationship between two quantities, numerator not necessarily included in denominator |
| Proportion | Ratio where numerator IS included in denominator; expressed as % |
Q5. Attack Rate
- Incidence rate expressed as %, used only during epidemics
- Formula: (New cases / Total population at risk) × 100
- Reflects the extent of the epidemic
Q6. Secondary Attack Rate (SAR)
- Number of exposed persons developing disease within the incubation period following exposure to a primary case
- Used to measure the transmissibility of a disease within households/closed groups
Q7. Incidence vs Prevalence
| Incidence | Prevalence | |
|---|---|---|
| Definition | New cases in a population in a time period | All current cases (old + new) at a point/period in time |
| Type | True rate | Really a ratio |
| Analogy | Film (continuous record) | Photograph (instantaneous) |
| Types | - | Point prevalence, Period prevalence |
Q8. Relationship Between Prevalence and Incidence
P = I × D (Prevalence = Incidence × mean Duration of illness)
- Long duration disease → high prevalence relative to incidence (e.g., TB, diabetes)
- Short/rapidly fatal disease → low prevalence (e.g., food poisoning, homicide)
SECTION 3: CONCEPT OF CAUSATION
Q9. Germ Theory of Disease
- Louis Pasteur era: one-to-one relationship (single agent → disease)
- Model: Disease agent → Man → Disease
- Limitation: doesn't explain why not everyone exposed develops disease
Q10. Web of Causation
- Concept by Brian MacMahon
- For multifactorial diseases (e.g., CHD), multiple causes form a complex web
- No single cause is necessary or sufficient
- Useful for chronic non-communicable diseases
Q11. Bradford Hill's Criteria for Causation (6 key criteria)
- Temporal association - Cause must precede effect (most essential)
- Strength of association - Higher RR = stronger causal link
- Specificity - One cause → one effect
- Consistency - Same finding in different studies/populations
- Biological plausibility - Makes biological sense
- Coherence - Does not conflict with known biology/natural history
From "Smoking and Health" - US Surgeon General's Report 1964
Q12. Types of Association
- Spurious association - Arises from bias (selection bias, information bias)
- Indirect association - Due to a confounding variable (e.g., altitude → iodine deficiency → goitre; altitude and goitre are indirectly associated)
- Direct (causal) association - True cause-effect relationship
SECTION 4: NATURAL HISTORY & ICEBERG
Q13. Natural History of Disease
- Stages: Susceptibility → Sub-clinical disease → Clinical disease → Disability/Death
- Basis for Levels of Prevention (Leavell & Clark)
Q14. Iceberg Phenomenon
- Visible tip = clinical cases seen by physician
- Submerged portion = latent, inapparent, presymptomatic, undiagnosed cases + carriers
- Waterline = border between apparent and inapparent disease
- Examples with large submerged portion: hypertension, diabetes, anaemia, mental illness
- Importance: Hidden cases = undiagnosed reservoir of infection
SECTION 5: EPIDEMIOLOGICAL STUDIES
Q15. Types of Epidemiological Studies
| Type | Examples |
|---|---|
| Descriptive | Case reports, cross-sectional, ecological |
| Analytical | Case-control, Cohort |
| Experimental | RCT, Field trials, Community trials |
Q16. Descriptive Epidemiology
- Studies distribution of disease by Person, Place, Time
- Generates hypotheses (does NOT test them)
- Answers: Who? Where? When?
Q17. Case-Control Study (Retrospective)
- Starts with cases (disease present) and controls (disease absent)
- Looks BACKWARDS for exposure
- Direction: Effect → Cause
- Measure of association: Odds Ratio (OR)
- Best for: rare diseases, chronic diseases (e.g., cancer)
- Advantage: Quick, cheap, small sample size
- Disadvantage: Recall bias, cannot calculate incidence/RR directly
Q18. Cohort Study (Prospective)
- Starts with exposed and non-exposed groups (disease-free)
- Follows forward and looks for disease development
- Direction: Cause → Effect
- Measure of association: Relative Risk (RR)
- Best for: common diseases, studying multiple outcomes of one exposure
- Advantage: True RR, temporal sequence established
- Disadvantage: Time-consuming, expensive, loss to follow-up
Q19. Relative Risk (RR)
- RR = Incidence in exposed / Incidence in non-exposed
- RR = 1: No association; RR >1: Positive association; RR <1: Protective
- Used in cohort studies
Q20. Attributable Risk (AR)
- AR = Incidence (exposed) - Incidence (non-exposed)
- Expressed as %: AR% = [(IE - IN) / IE] × 100
- Indicates how much disease is attributable to the exposure and could be prevented by eliminating it
Q21. Odds Ratio (OR)
- Used in case-control studies (incidence not known, so RR cannot be calculated directly)
- OR = (a × d) / (b × c) from the 2×2 table
- When disease is rare, OR ≈ RR
Q22. Randomized Controlled Trial (RCT)
- Gold standard of experimental epidemiology
- Features: Randomization, Control group, Blinding
- Eliminates confounding by randomization
- Measures: Efficacy (can it work?) and Effectiveness (does it work in practice?)
SECTION 6: TYPES OF EPIDEMICS
Q23. Types of Epidemics
A. Common-source:
- Point source (single exposure) - explosive, one peak, all cases within ONE incubation period
- Continuous/repeated exposure - more prolonged, irregular curve
B. Propagated - person-to-person; gradual rise, multiple peaks, secondary waves
C. Slow (modern) epidemics - e.g., obesity, cardiovascular disease
Q24. Point Source vs Propagated Epidemic
| Feature | Point Source | Propagated |
|---|---|---|
| Exposure | Brief, simultaneous | Ongoing transmission |
| Curve | Single rapid peak, no secondary waves | Multiple peaks, gradual |
| Duration | Within 1 incubation period | Over multiple incubation periods |
| Example | Food poisoning | Hepatitis A, COVID-19 |
Q25. Epidemic Curve
- Graphical display of cases over time
- Suggests: (1) Time relation to exposure, (2) Seasonal pattern, (3) Common-source vs propagated spread
- Median incubation period = time for 50% of cases to occur after exposure
SECTION 7: SURVEILLANCE & SCREENING
Q26. Surveillance (Epidemiological)
"Continuous scrutiny of the factors that determine the occurrence and distribution of disease and other conditions of ill-health" (Langmuir)
- Types: Passive, Active, Sentinel surveillance
- Sentinel surveillance = monitoring a sample of carefully selected reporting sites/populations to get early warning signals
Q27. Uses of Incubation Period (4 uses - Park)
- Tracing source of infection (short IP → easier to trace)
- Period of surveillance/quarantine = maximum incubation period
- Immunization - passive immunoglobulins within IP can prevent clinical illness
- Identifying point source vs propagated epidemic
- Prognosis - shorter IP → worse prognosis (tetanus, rabies)
ONE-LINE ANSWERS (Quick Recall)
| Question | Answer |
|---|---|
| Formula P = I × D | Prevalence = Incidence × Duration |
| Measure in case-control study | Odds Ratio |
| Measure in cohort study | Relative Risk |
| Gold standard of experimental epidemiology | RCT |
| Iceberg tip = | Clinical cases |
| Bradford Hill's most important criterion | Temporal association |
| Point source epidemic duration | Within ONE incubation period |
| Median incubation period | Time for 50% of cases after exposure |
| Confounding variable example | Altitude-Iodine deficiency-Goitre |
| Web of causation - author | Brian MacMahon |
| Aims of epidemiology body | IEA (International Epidemiological Association) |
Source: Park's Textbook of Preventive and Social Medicine, Epidemiology chapters (Blocks 1 & 2)
Difference between epidemic, endemic and outbreak
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
All definitions sourced directly from Park's. Here's the complete answer:
Epidemic vs Endemic vs Outbreak (+ Related Terms)
From Park's Textbook of Preventive and Social Medicine
Definitions (Word Origins Included - Asked in Exams)
1. EPIDEMIC
Etymology: Epi (upon) + demos (people)
"The occurrence in a community or region of cases of an illness, specific health-related behaviour, or other health-related events clearly in excess of normal expectancy."
- The community/region and time period must be specified precisely
- Epidemicity is relative - compared to the usual frequency of the disease in the same area, same season, same population
- Even 2 cases of a disease long absent from a population may constitute an epidemic
- Epidemic threshold for common diseases (e.g., influenza) = 2 standard errors above endemic level
2. ENDEMIC
Etymology: En (in) + demos (people)
"The constant presence of a disease or infectious agent within a given geographic area or population group, without importation from outside; may also refer to the 'usual' or expected frequency of the disease within such area."
- Example: Common cold is endemic - somebody always has one
- An endemic disease when conditions are favourable may burst into an epidemic (e.g., hepatitis A, typhoid fever)
Sub-types of endemic (High Yield):
| Term | Meaning |
|---|---|
| Hyperendemic | Constantly present at high incidence/prevalence, affects all age groups equally |
| Holoendemic | High infection beginning early in life, affects mostly children; adults show less disease - e.g., malaria |
3. OUTBREAK
"A sudden increase in occurrence of a disease in a particular time and place."
- A single case of a communicable disease long absent from a population may also constitute an outbreak
- Or emergence of a previously unknown disease may also constitute an outbreak
- Term is often used interchangeably with epidemic but implies a more localised event
Warning signs of an impending outbreak:
- Clustering of cases/deaths in time and/or space
- Unusual increase in number of cases or deaths
- Even a single case of measles, AFP, cholera, plague, dengue or JE
- Acute febrile illness of unknown aetiology
- Shifting in age distribution of cases
- Sudden increase/high vector density
- Natural disasters
4. PANDEMIC
"An epidemic occurring over a very wide area, crossing international boundaries, and usually affecting a large number of people."
- Requirements for a pandemic:
- Agent must be able to infect humans
- Agent must be able to cause disease in humans
- Agent must spread easily from human to human
- Examples: Influenza pandemics, cholera pandemics, COVID-19
5. SPORADIC
"Cases occur irregularly, haphazardly from time to time, and generally infrequently."
- Cases are widely separated in space and time
- Little or no connection with each other
- No recognizable common source
- Examples: Tetanus, Herpes zoster, Meningococcal meningitis
- May be the starting point of an epidemic when conditions become favourable
6. EXOTIC
Diseases imported into a country in which they do not otherwise occur.
7. ENZOOTIC
An endemic occurring in animals - e.g., anthrax, rabies, brucellosis, bovine tuberculosis, endemic typhus, tick typhus.
Comparison Table (Exam Summary)
| Feature | Epidemic | Endemic | Outbreak | Pandemic | Sporadic |
|---|---|---|---|---|---|
| Frequency | Excess of normal expectancy | Constant/usual level | Sudden local increase | Massive, widespread | Irregular, infrequent |
| Geographic spread | Community/region | Given area/population | Localised | International, crosses borders | Scattered |
| Time | Specified period | Continuously present | Sudden | Large-scale, prolonged | No pattern |
| Importation | May be imported | Without importation | Local | Cross-border spread | No defined source |
| Example | Cholera outbreak in a city | Common cold | Food poisoning in a school | COVID-19, Influenza 1918 | Tetanus, Herpes zoster |
Key One-Liners for MCQs
- Epidemic = excess over normal expectancy in a defined area and time
- Endemic = constant presence without importation
- Pandemic = epidemic + international boundaries
- Outbreak = epidemic but more localised in time and place
- Sporadic = irregular, no connection between cases
- Hyperendemic = high prevalence, all age groups equally
- Holoendemic = children most affected, adults relatively spared - e.g., malaria
- Epidemic threshold = 2 SD above endemic level (influenza)
Source: Park's Textbook of Preventive and Social Medicine, Infectious Disease Epidemiology section, pp. 112-115
This is a shared conversation. Sign in to Orris to start your own chat.