Make a study guide of key points from Moore, clinically oriented anatomy, 7th edition, K.L. Moore, A.F. Dalley, A.M.R. Agur; pg.: 715-721; 689-693; 724, 726 – 728; 732, 736 – 737; 738, 741-744; 757-761, 763, 767 – 768 , 779-782, 790; with the relevant diagramsto visualise anatomical structures
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Note: Moore's Clinically Oriented Anatomy 7th ed. is not in the digital library, but the page ranges you listed (pp. 689-790) map precisely to Chapter 9: Head of that textbook - covering the face, parotid region, scalp, infratemporal fossa, temporomandibular joint, orbit, and related neurovascular structures. The study guide below draws on Gray's Anatomy for Students (which covers identical content) with the original diagrams from that database.
Study Guide: Head Anatomy
Based on Moore's Clinically Oriented Anatomy, 7th ed., pp. 689–790
(Content sourced from Gray's Anatomy for Students — identical anatomical coverage)
PART 1 - THE FACE (pp. 689–693)
Key Points
Definition: The face extends from the superciliary arches superiorly to the lower border of the mandible inferiorly, and laterally to the ears.
Muscles of Facial Expression
All muscles of the face:
- Develop from the 2nd pharyngeal arch
- Innervated by the facial nerve [VII]
- Located in the superficial fascia
- Origins from bone or fascia, insertions into skin
- Act as sphincters and dilators of orbital, nasal, and oral orifices
Diagram - Facial Muscles:
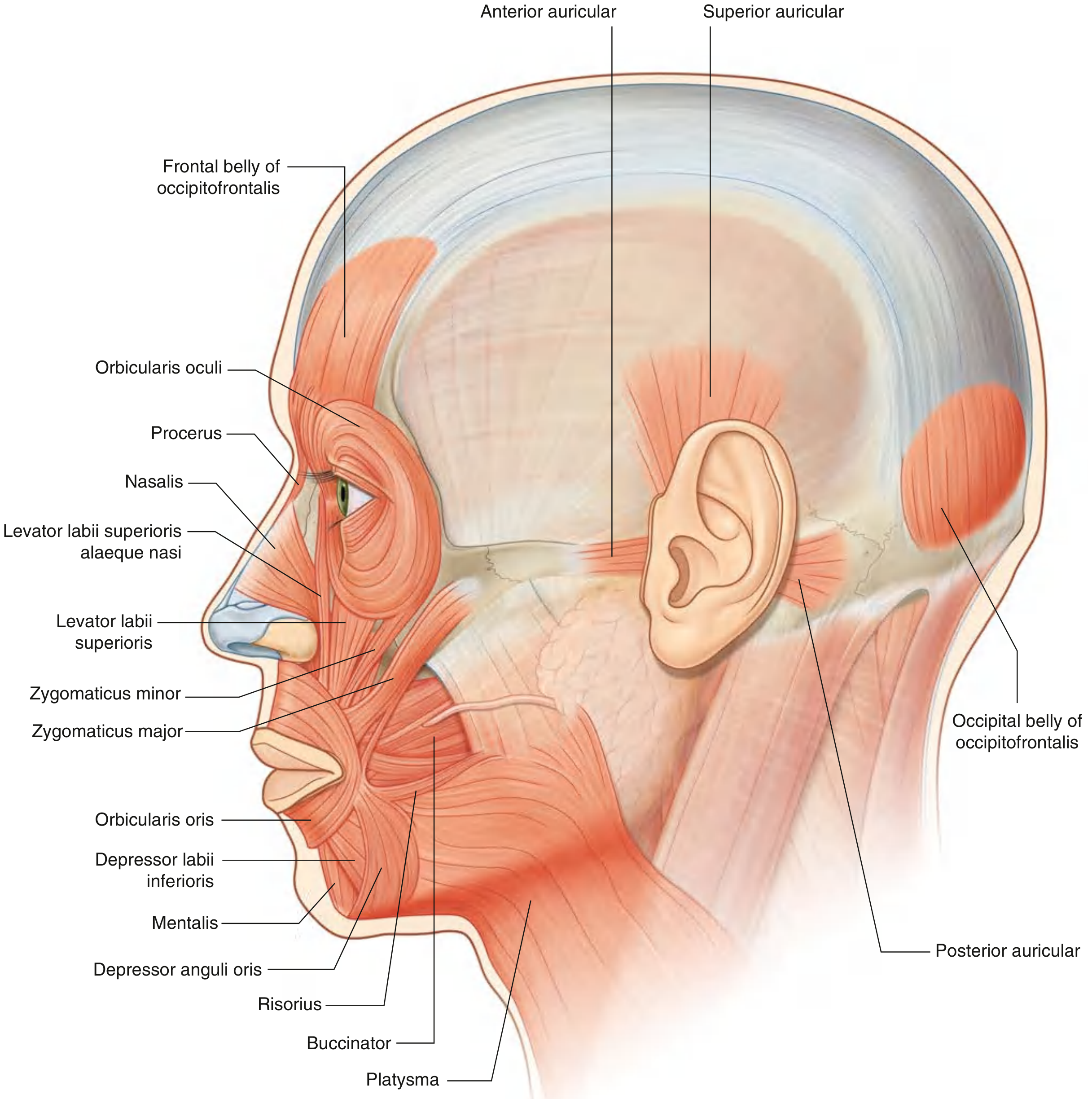
Functional Groups
| Group | Muscles | Key Function |
|---|---|---|
| Orbital | Orbicularis oculi (palpebral + orbital parts), Corrugator supercilii | Eyelid closure (gentle / forceful); brow drawing |
| Nasal | Procerus, Nasalis, Depressor septi | Nose movement/compression |
| Oral | Orbicularis oris, Zygomaticus major/minor, Levator labii superioris, Depressor labii, Mentalis, Buccinator, Risorius | Lip movements, smile, pouting, cheek compression |
| Scalp | Occipitofrontalis (frontal + occipital bellies via galea aponeurotica), Auricular muscles | Scalp movement, ear movement |
Neurovascular Supply of the Face
- Motor: All via facial nerve [VII] branches
- Sensory: Trigeminal nerve [V]:
- V1 (ophthalmic) - forehead, upper eyelid
- V2 (maxillary) - cheek, nose, upper lip (exits via infraorbital foramen)
- V3 (mandibular) - lower lip, chin (exits via mental foramen)
- Arterial: Facial artery (branch of external carotid), plus supraorbital, infraorbital, and mental arteries
- Venous: Facial vein (drains to internal jugular); communicates with cavernous sinus via ophthalmic veins
Clinical Pearl - Danger Zone
The area between the corners of the mouth and the bridge of the nose ("danger triangle") is dangerous for infections: the facial vein has no valves and communicates with the cavernous sinus, allowing spread of infection intracranially.
PART 2 - PAROTID REGION (pp. 715–721)
Parotid Gland - Overview
- Largest of the three paired salivary glands
- Location: anterior to and below the lower half of the ear; overlies the masseter and ramus of mandible
- Extends from the zygomatic arch superiorly to the lower border of the mandible inferiorly
- Enclosed in the split investing layer of deep cervical fascia
- Produces watery saliva and salivary amylase
Diagram - Parotid Gland (Lateral view and cross-section):
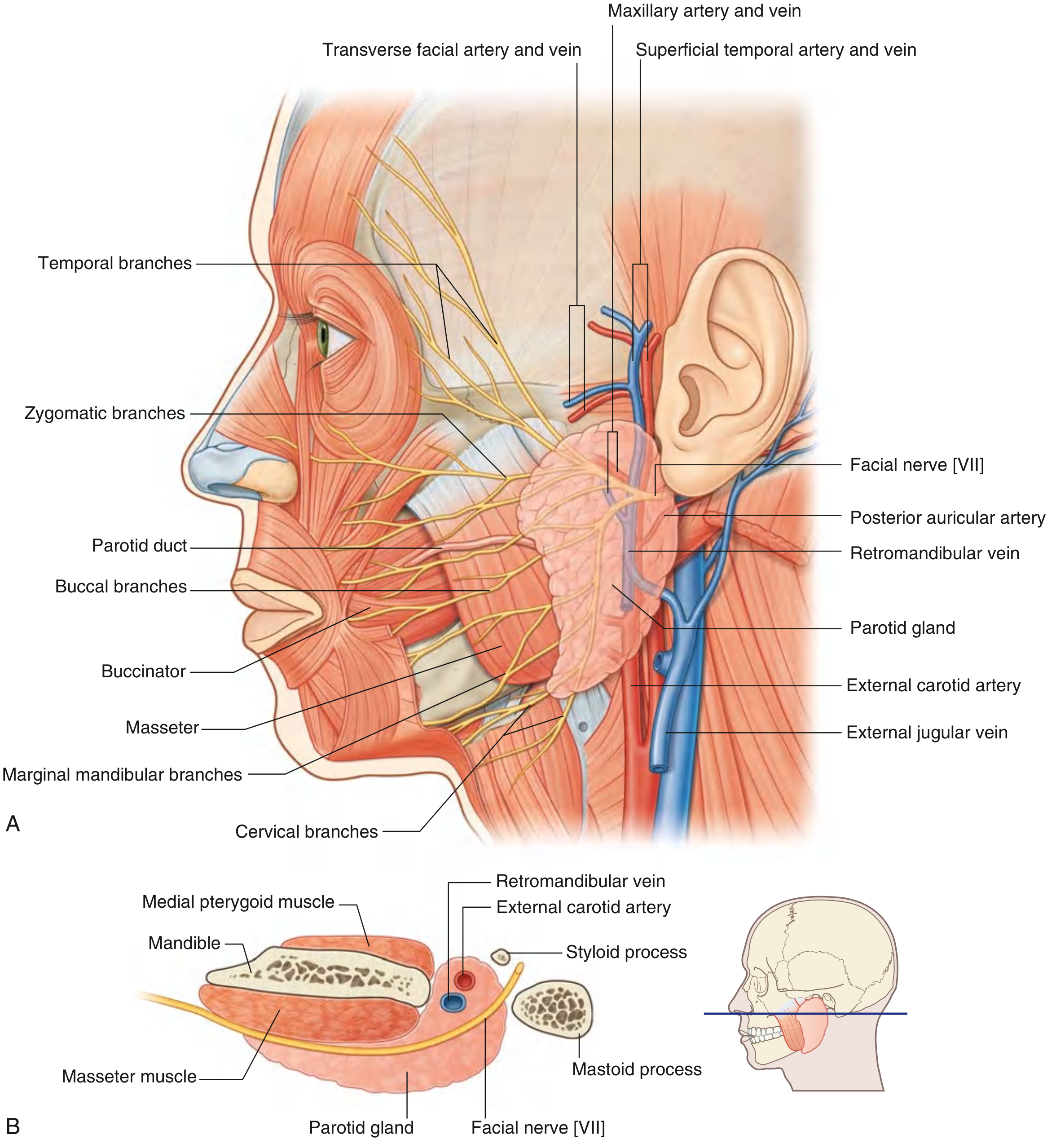
Parotid Duct (Stensen's Duct)
- Leaves the anterior edge of the gland midway between the zygomatic arch and corner of the mouth
- Crosses the face horizontally, crosses the medial border of the masseter, then turns deep into the buccal fat pad
- Pierces the buccinator muscle
- Opens into the oral cavity at the level of the upper 2nd molar tooth
Important Relationships Within the Parotid Gland
Three major structures pass through the gland (lateral to medial):
- Facial nerve [VII] - most superficial
- Retromandibular vein - intermediate
- External carotid artery - deepest
Facial Nerve [VII] in the Parotid
- Exits the skull via the stylomastoid foramen
- Enters the parotid gland and divides into upper and lower trunks
- Five terminal branches emerge from the borders of the gland:
- Temporal (upper border)
- Zygomatic (anterior border)
- Buccal (anterior border)
- Marginal mandibular (lower border)
- Cervical (lower border)
External Carotid Artery
- Enters/passes deep to the inferior border of the gland
- Gives off the posterior auricular artery within the gland
- Divides into two terminal branches near the lower ear:
- Maxillary artery - passes deep to the mandible
- Superficial temporal artery - exits upper border of gland (gives off transverse facial artery first)
Retromandibular Vein
- Formed within the parotid gland by the union of the superficial temporal vein and maxillary vein
- Divides below the gland into anterior and posterior branches
Innervation of the Parotid Gland
- Sensory + secretomotor: Auriculotemporal nerve (branch of V3)
- Secretomotor pathway:
- Preganglionic parasympathetics: from glossopharyngeal nerve [IX] via lesser petrosal nerve
- Synapse in the otic ganglion (just inferior to foramen ovale)
- Postganglionic parasympathetics travel with the auriculotemporal nerve
Clinical Pearls
- Parotid tumors (mostly benign: pleomorphic adenoma, Warthin's tumor): The relationship to the facial nerve must be defined pre-operatively. Damage to upper branches = inability to close the eye (risk of corneal damage). Damage to lower branches = facial asymmetry.
- Parotid stones: Intense pain on salivation; reproduced with lemon juice in clinic. Anterior duct stones may be removed by sphincterotomy; posterior stones may require parotidectomy.
- Frey's Syndrome: After parotid surgery, aberrant regeneration of auriculotemporal nerve parasympathetics to sweat glands causes sweating over the cheek during eating (gustatory sweating).
PART 3 - INFRATEMPORAL FOSSA (pp. 724, 726–728)
Boundaries of the Infratemporal Fossa
Diagram - Borders of the Infratemporal Fossa:
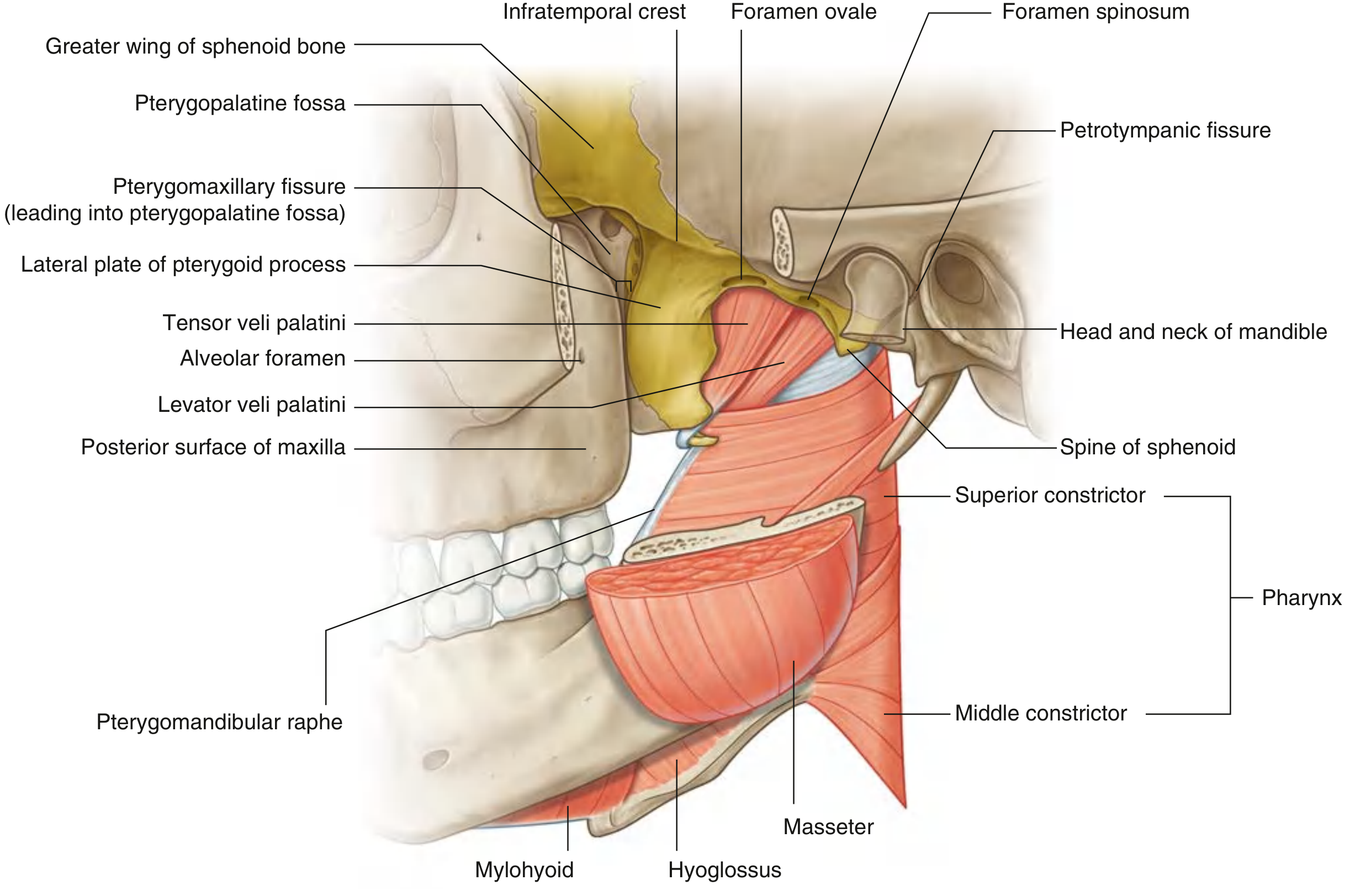
| Wall | Structure |
|---|---|
| Roof | Inferior surfaces of greater wing of sphenoid + temporal bone; contains foramen spinosum, foramen ovale, petrotympanic fissure |
| Lateral wall | Medial surface of the ramus of the mandible |
| Medial wall | Lateral plate of pterygoid process (anteriorly); pharynx + tensor/levator veli palatini (posteriorly); contains pterygomaxillary fissure |
| Anterior wall | Posterior surface of maxilla; contains alveolar foramen; upper part opens as inferior orbital fissure |
| Posterior | Open to the neck |
Contents of the Infratemporal Fossa
| Structure | Notes |
|---|---|
| Medial pterygoid muscle | Elevates mandible (closes jaw), protrusion and side-to-side movements |
| Lateral pterygoid muscle | Depresses/protrudes mandible; opens the mouth |
| Maxillary artery | Largest branch of external carotid; passes to pterygopalatine fossa |
| Mandibular nerve [V3] | Exits via foramen ovale; divides into anterior (mainly motor) + posterior (mainly sensory) trunks |
| Pterygoid plexus of veins | Communicates with facial vein and cavernous sinus |
| Sphenomandibular ligament | Extracapsular ligament of TMJ; from spine of sphenoid to lingula of mandible |
Pterygoid Muscles
Medial pterygoid:
- Deep head: from medial surface of lateral pterygoid plate + palatine bone
- Superficial head: from maxillary tuberosity
- Insertion: medial surface of ramus of mandible
- Forms a "pterygoid sling" with the masseter around the angle of the mandible
Lateral pterygoid:
- Upper head: from infratemporal surface of greater wing of sphenoid
- Lower head: from lateral surface of lateral pterygoid plate
- Insertion: pterygoid fovea of mandible + articular disc/capsule of TMJ
- Function: protrusion and depression (opens mouth); guides TMJ disc
Temporomandibular Joint (TMJ) (pp. 732, 736–737)
Diagram - TMJ Structure and Movement:
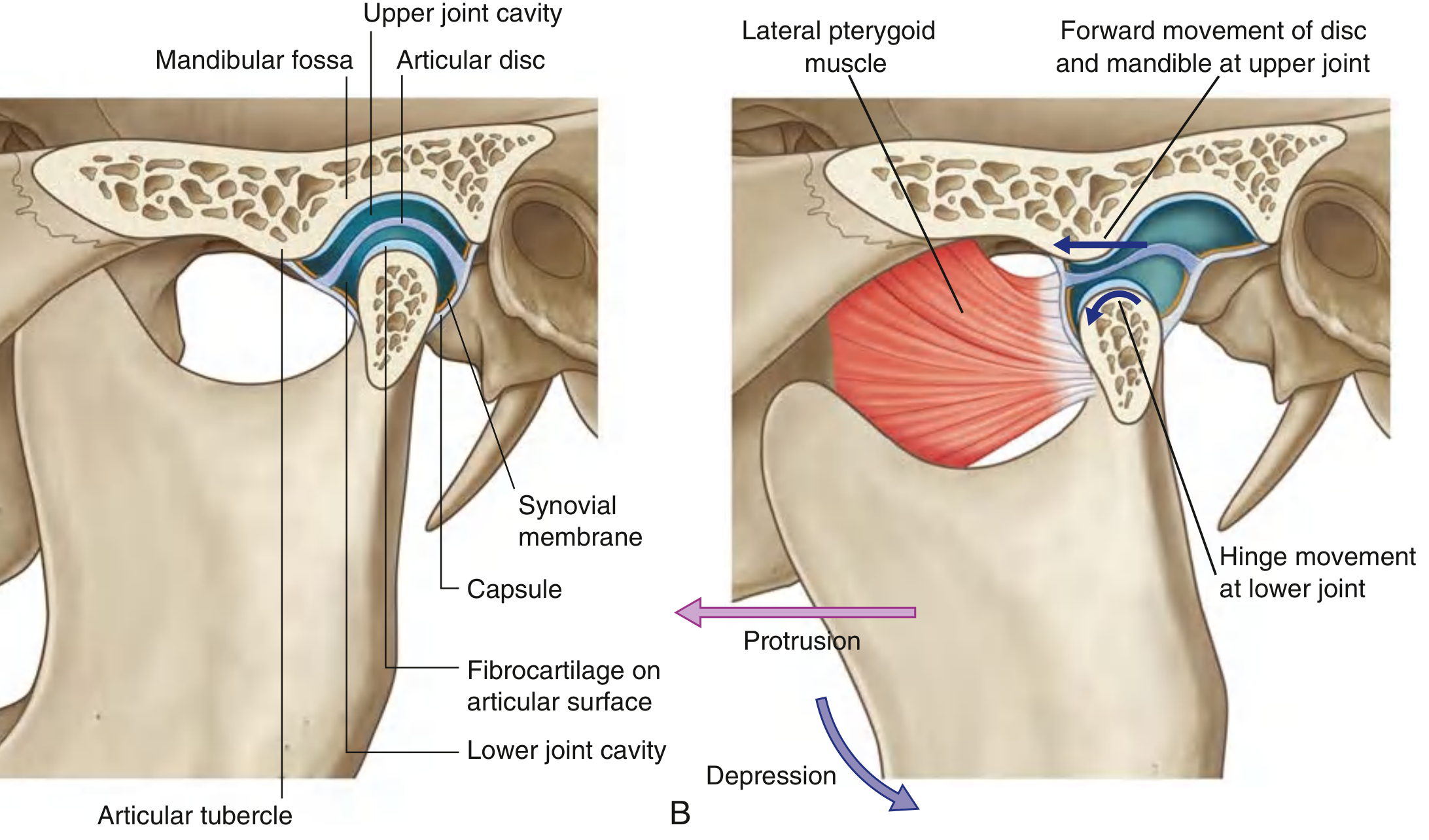
Key features:
- Synovial joint between the head of the mandible and articular fossa + tubercle of the temporal bone
- Articular surfaces covered by fibrocartilage (not hyaline cartilage - clinically important)
- Completely divided by a fibrous articular disc into two separate compartments:
- Lower compartment: hinge movement (depression/elevation of mandible)
- Upper compartment: translatory/gliding movement (protrusion/retraction)
- Opening the mouth requires both depression (lower joint) AND protrusion (upper joint)
Ligaments:
- Lateral ligament: just lateral to the capsule; from articular tubercle to neck of mandible; resists posterior dislocation
- Sphenomandibular ligament: from spine of sphenoid to lingula; guides mandibular movement
- Stylomandibular ligament: from styloid process to angle/posterior ramus; tightens during protrusion
Innervation: Auriculotemporal nerve and masseteric nerve (both branches of V3)
PART 4 - MANDIBULAR NERVE [V3] (pp. 738, 741–744)
Diagram - Mandibular Nerve [V3] Branches:
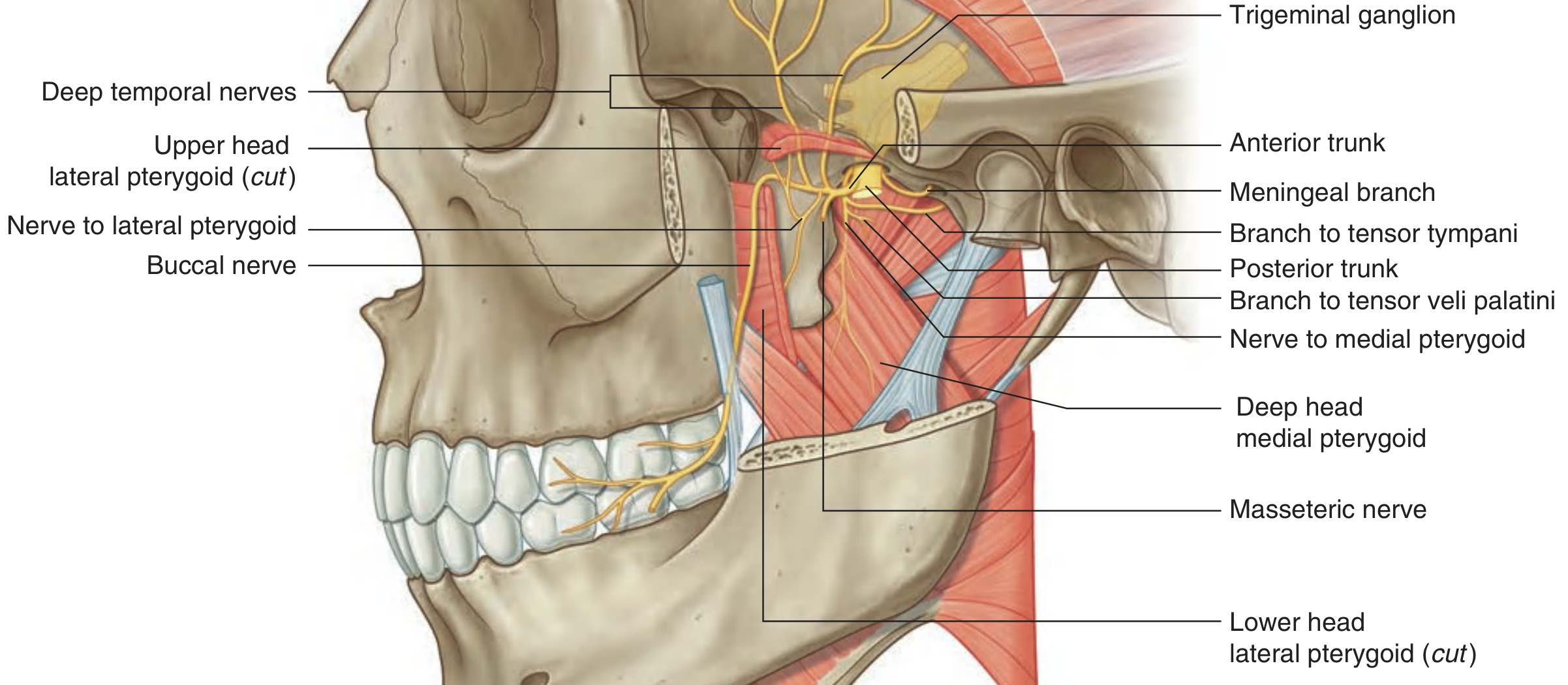
V3 - Division and Branches
V3 exits the skull through the foramen ovale.
Immediately after exiting, gives:
- Meningeal branch (re-enters via foramen spinosum with middle meningeal artery)
- Nerve to medial pterygoid (with small branches to tensor tympani and tensor veli palatini)
Anterior trunk (mainly MOTOR):
| Branch | Target | Function |
|---|---|---|
| Masseteric nerve | Masseter | Motor (closes jaw) |
| Deep temporal nerves (anterior + posterior) | Temporalis | Motor (elevates, retracts mandible) |
| Nerve to lateral pterygoid | Lateral pterygoid | Motor (opens, protrudes jaw) |
| Buccal nerve | Cheek skin/mucosa, buccal gingivae of lower molars | Sensory |
Posterior trunk (mainly SENSORY):
| Branch | Target | Function |
|---|---|---|
| Auriculotemporal nerve | Skin of temporal region, auricle, external auditory meatus, TMJ; carries parotid secretomotor fibers | Sensory + secretomotor |
| Lingual nerve | Anterior 2/3 of tongue (general sensation + taste via chorda tympani) | Sensory (joins chorda tympani from CN VII) |
| Inferior alveolar nerve | Lower teeth, gingiva, chin, lower lip (mental nerve) | Sensory; branch to mylohyoid (motor) |
Clinical Pearl - Inferior Alveolar Nerve Block
To anesthetize for dental procedures: needle placed lateral to the anterior arch of the fauces (palatoglossal arch), advanced along the medial border of the ramus to deposit anesthetic near the mandibular foramen.
PART 5 - MAXILLARY ARTERY (pp. 757–761, 763)
Overview
- Largest branch of the external carotid artery
- Major supply for the nasal cavity, oral cavity, all teeth, and dura mater
- Originates within the parotid gland, passes through the infratemporal fossa, and enters the pterygopalatine fossa via the pterygomaxillary fissure
Three Parts and Their Branches
Part 1 - Between neck of mandible and sphenomandibular ligament:
| Branch | Destination |
|---|---|
| Deep auricular artery | External acoustic meatus |
| Anterior tympanic artery | Tympanic membrane |
| Middle meningeal artery | Passes through foramen spinosum; largest meningeal vessel; supplies dura, bone, bone marrow of cranial walls |
| Inferior alveolar artery | Travels with inferior alveolar nerve through mandibular canal; supplies lower teeth; mental branch exits mental foramen |
| Accessory meningeal artery | Small; enters foramen ovale |
Part 2 - Related to lateral pterygoid muscle:
| Branch | Destination |
|---|---|
| Deep temporal arteries | Temporalis muscle |
| Masseteric artery | Masseter muscle |
| Buccal artery | Buccinator and cheek |
| Pterygoid branches | Pterygoid muscles |
Part 3 - In the pterygopalatine fossa:
Major terminal branches supplying nasal cavity, palate, pharynx, and orbit.
Clinical Pearl - Middle Meningeal Artery
Runs in a groove on the inner surface of the temporal bone. Damage to the temporal bone in trauma (e.g., pterion fracture) can rupture this artery, causing an extradural (epidural) haematoma. Classic presentation: loss of consciousness → lucid interval → rapid deterioration as the haematoma expands and herniates the uncus.
PART 6 - SCALP (pp. 767–768)
Layers of the Scalp - the "SCALP" mnemonic
Diagram - Scalp Layers:
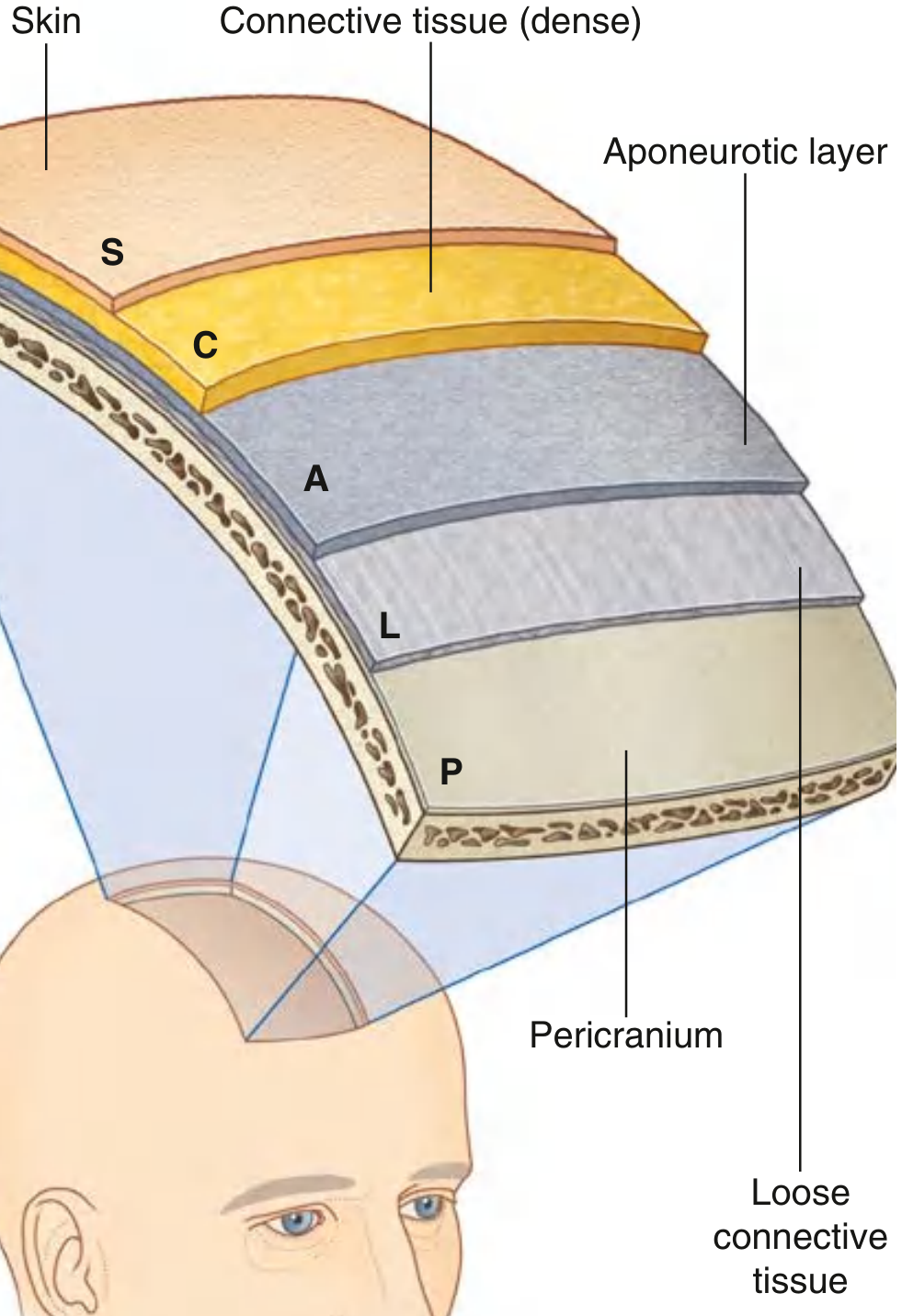
| Layer | Key Features |
|---|---|
| S - Skin | Thickest on the body; hair-bearing |
| C - dense Connective tissue | Anchors skin to galea; contains all vessels and nerves; vessels held open by connective tissue sheaths → profuse bleeding when cut |
| A - Aponeurotic layer (galea aponeurotica) | Epicranial aponeurosis connects frontal belly (occipitofrontalis) anteriorly to occipital belly posteriorly; the "scalp proper" (S+C+A) is what is torn in scalping injuries |
| L - Loose connective tissue | "Danger space" - allows scalp proper to move freely over the skull; infections/blood spread freely here; emissary veins traverse this layer connecting superficial veins to intracranial dural venous sinuses |
| P - Pericranium | Periosteum of the skull; tightly adherent to bone; continuous at sutures with the endosteum |
Neurovascular Supply of the Scalp
Arterial supply (all anastomose freely):
- Anterior: supratrochlear + supraorbital arteries (from ophthalmic a., branch of internal carotid)
- Lateral: superficial temporal artery (branch of external carotid)
- Posterior: posterior auricular + occipital arteries (branches of external carotid)
Venous drainage: corresponding veins → drain to external jugular vein and via emissary veins to dural venous sinuses
Sensory innervation:
- Anterior: supratrochlear + supraorbital nerves (V1)
- Lateral: zygomaticotemporal nerve (V2) and auriculotemporal nerve (V3)
- Posterior: greater occipital nerve (C2 posterior ramus), lesser occipital nerve (C2)
Clinical Pearls
- Scalp lacerations bleed profusely because vessel walls are tethered open by the dense connective tissue
- Subgaleal hematoma (blood in the L-layer) can spread widely over the whole vault
- Emissary veins in the loose layer lack valves → potential route for intracranial spread of infection from scalp
PART 7 - THE ORBIT (pp. 779–782, 790)
Bony Orbit - Overview
The orbits are bilateral pyramid-shaped bony cavities in the upper face.
Diagram - Bones of the Orbit:
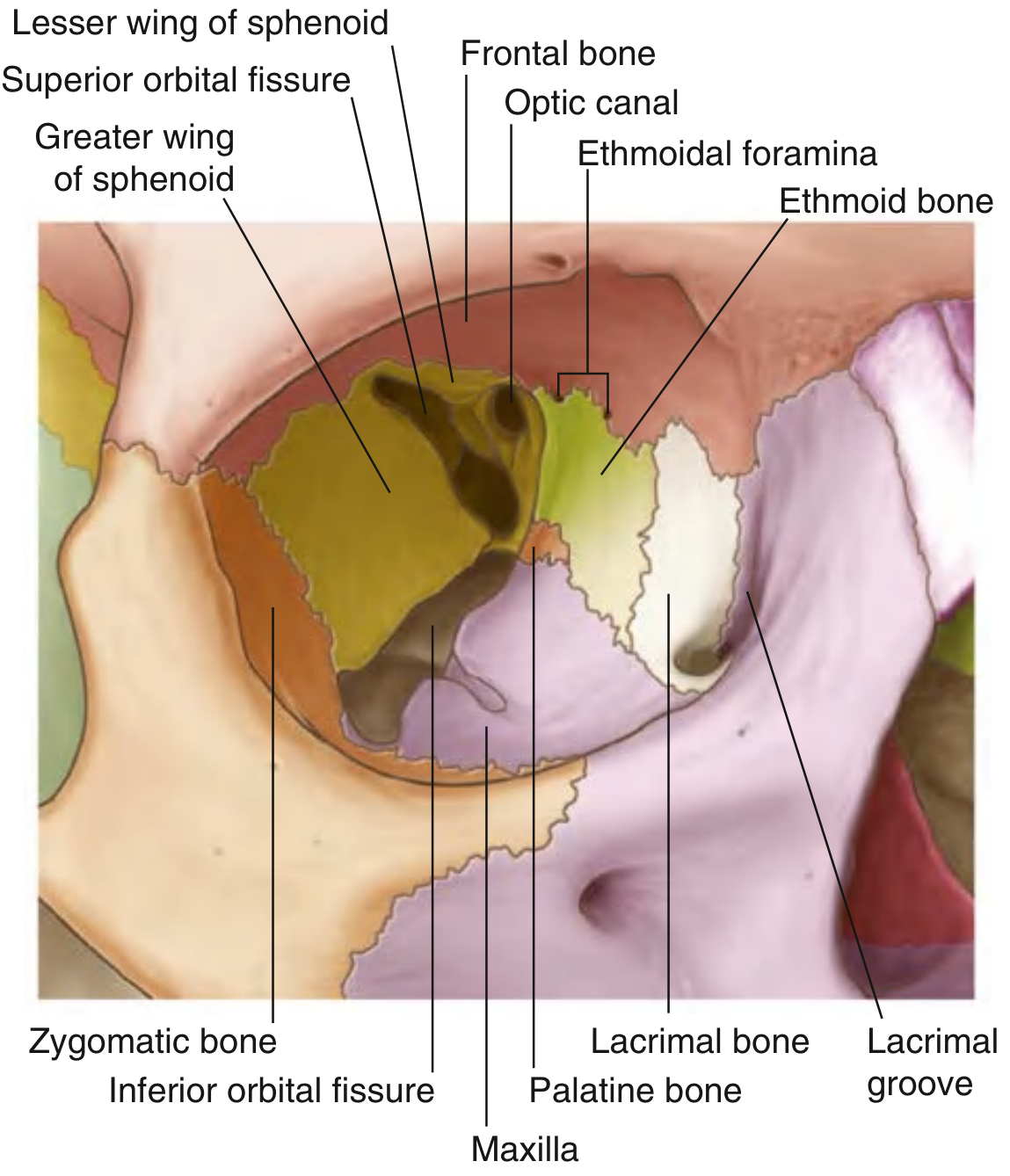
Seven bones: Maxilla, Zygomatic, Frontal, Ethmoid, Lacrimal, Sphenoid, Palatine
(Mnemonic: "My Zipper Flies Even Less Sexy, Partner")
Shape: Pyramid, base opening anteriorly on the face, apex directed posteromedially toward the optic foramen.
Walls of the Orbit
| Wall | Bones | Key Features |
|---|---|---|
| Roof (superior) | Frontal bone (mainly) + lesser wing of sphenoid posteriorly | Trochlear fovea (anteromedial); lacrimal fossa (anterolateral); separates orbit from anterior cranial fossa |
| Medial wall | Maxilla, lacrimal, ethmoid (largest contributor), sphenoid | Thinnest wall; ethmoidal air cells visible in dried skull; anterior + posterior ethmoidal foramina for nerves/vessels; lacrimal groove anteriorly for nasolacrimal duct |
| Floor (inferior) | Maxilla (mainly), zygomatic, palatine | Infraorbital groove → canal → foramen for infraorbital nerve; blowout fractures common here |
| Lateral wall | Zygomatic (anterior) + greater wing of sphenoid (posterior) | Thickest, strongest wall |
Orbital Openings
| Opening | Location | Contents |
|---|---|---|
| Optic canal | Apex (lesser wing of sphenoid) | Optic nerve [II]; ophthalmic artery |
| Superior orbital fissure | Between lesser + greater wings of sphenoid | CN III, IV, V1 (via nasociliary, frontal, lacrimal branches), VI; superior ophthalmic vein |
| Inferior orbital fissure | Between greater wing of sphenoid + maxilla | CN V2 (infraorbital nerve); inferior ophthalmic vein; zygomatic nerve |
| Anterior + posterior ethmoidal foramina | Medial wall at fronto-ethmoidal suture | Anterior + posterior ethmoidal nerves and arteries |
| Nasolacrimal canal | Anteromedial floor | Nasolacrimal duct |
Contents of the Orbit
- Eyeball and optic nerve [II]
- Extraocular muscles (superior/inferior/medial/lateral rectus; superior/inferior oblique; levator palpebrae superioris)
- Lacrimal gland and apparatus
- Orbital fat (cushions the eyeball)
- Ophthalmic artery (branch of internal carotid)
- Ophthalmic veins
- Ciliary ganglion (parasympathetic)
- Nerves: II, III, IV, V1, VI
Clinical Pearls
- Orbital blowout fracture: Direct blow to the eye increases intraorbital pressure, which causes the weakest wall (the floor, over the maxillary sinus) to fracture. The inferior rectus muscle can herniate into the maxillary sinus → diplopia on upward gaze (entrapment test). Check for infraorbital nerve numbness.
- Orbital cellulitis: Infection can spread from ethmoidal sinuses through the paper-thin medial wall (lamina papyracea) of the ethmoid. Presents with proptosis, painful ophthalmoplegia, and visual loss if untreated.
- Cavernous sinus thrombosis: Via the superior ophthalmic vein. Presents with proptosis, chemosis, painful ophthalmoplegia, and fever.
Quick Reference Summary Table
| Region | Key Structure | Key Nerve | Key Artery | Clinical Importance |
|---|---|---|---|---|
| Face | Muscles of expression | Facial nerve [VII] (motor), V1/V2/V3 (sensory) | Facial artery | Facial palsy; cavernous sinus thrombosis via danger triangle |
| Parotid | Gland with embedded facial nerve | CN VII, auriculotemporal (V3) | External carotid → superficial temporal + maxillary | Parotid tumors risk CN VII; Frey's syndrome post-op |
| Infratemporal fossa | Pterygoid muscles, maxillary artery, V3 | Mandibular nerve [V3] | Maxillary artery | Dental blocks; trismus; pterygomaxillary spread of tumors |
| TMJ | Articular disc; fibrocartilage surfaces | Auriculotemporal nerve (V3) | Superficial temporal artery | TMJ dislocation; arthritis; disc displacement |
| Scalp | 5 SCALP layers; galea aponeurotica | V1, V2, V3, C2, C2-C3 | Supraorbital, superficial temporal, occipital, posterior auricular | Scalp lacerations bleed heavily; subgaleal hematoma; emissary vein infection spread |
| Orbit | 7-bone pyramid; superior orbital fissure | CN II, III, IV, V1, VI | Ophthalmic artery (from ICA) | Blowout fracture (floor); orbital cellulitis (medial wall); cavernous sinus thrombosis |
Sources: Gray's Anatomy for Students (Elsevier, 9780323934237), corresponding to content in Moore's Clinically Oriented Anatomy 7th ed., Chapter 9 (Head). Diagrams from Gray's Anatomy for Students digital edition.
This is a shared conversation. Sign in to Orris to start your own chat.