Open bankart surgery images
Reading File
Searching Images
open Bankart surgery shoulder stabilization procedure
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here are intraoperative and perioperative images from the Open Anterior Labral (Bankart) Repair, sourced from Rockwood and Green's Fractures in Adults, 10th ed. (2025):
Fig. 35-34A — Surgical Incision Planning
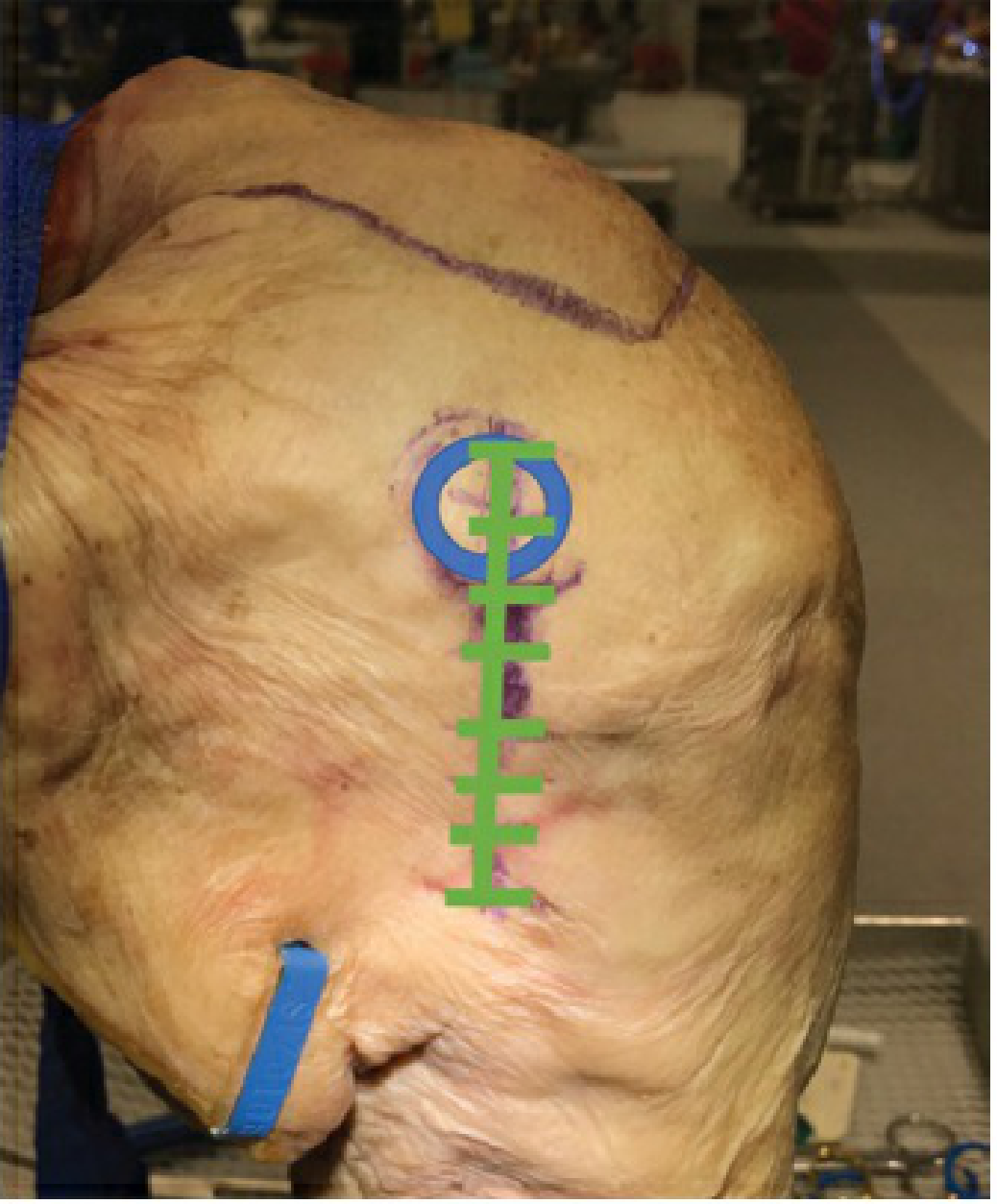
The green line marks the midaxillary crease incision, centered over the coracoid down to the axilla. The blue circle marks the coracoid process landmark.
Fig. 35-34B — Deltopectoral Approach with Retractors
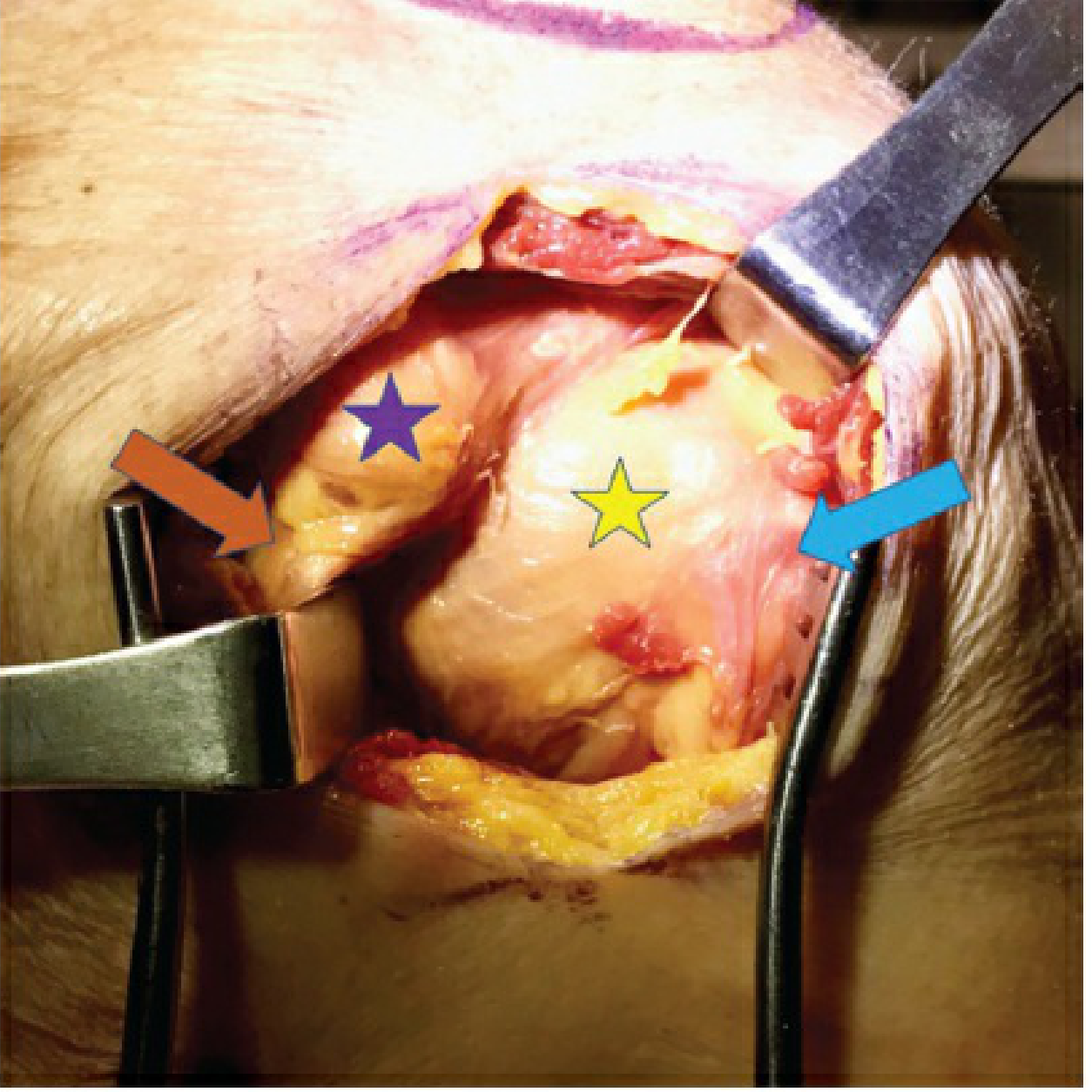
After the deltopectoral interval is opened: purple star = coracoid process; orange arrow = conjoint tendon; yellow star = lesser tuberosity; blue arrow = biceps tendon.
Fig. 35-34C — Subscapularis Tenotomy
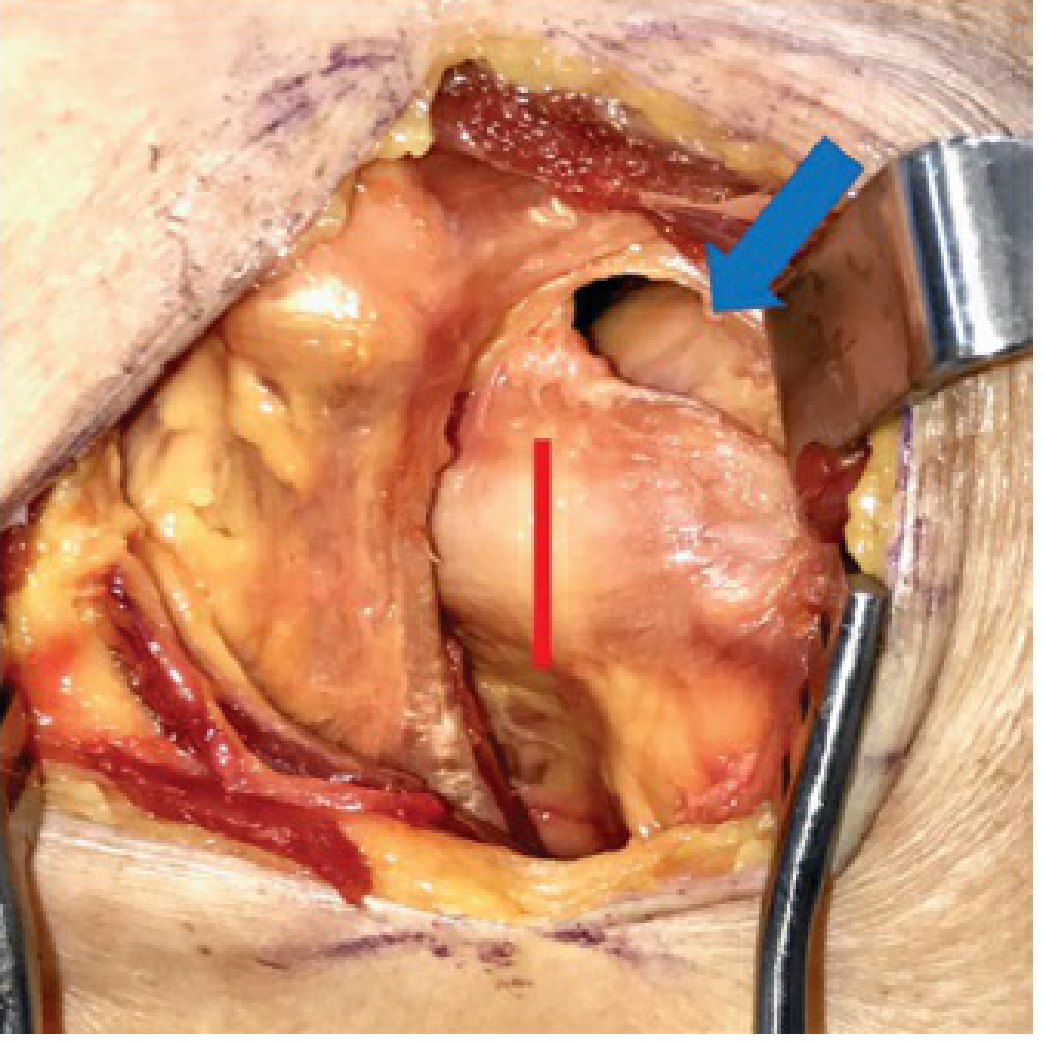
The rotator interval is split to identify the top of the subscapularis. The red line marks the tenotomy site 1 cm from the bicipital groove, preserving a cuff of tissue for later repair. Blue arrow indicates the rotator interval opening.
Fig. 35-34D — Subscapularis Separated from Capsule
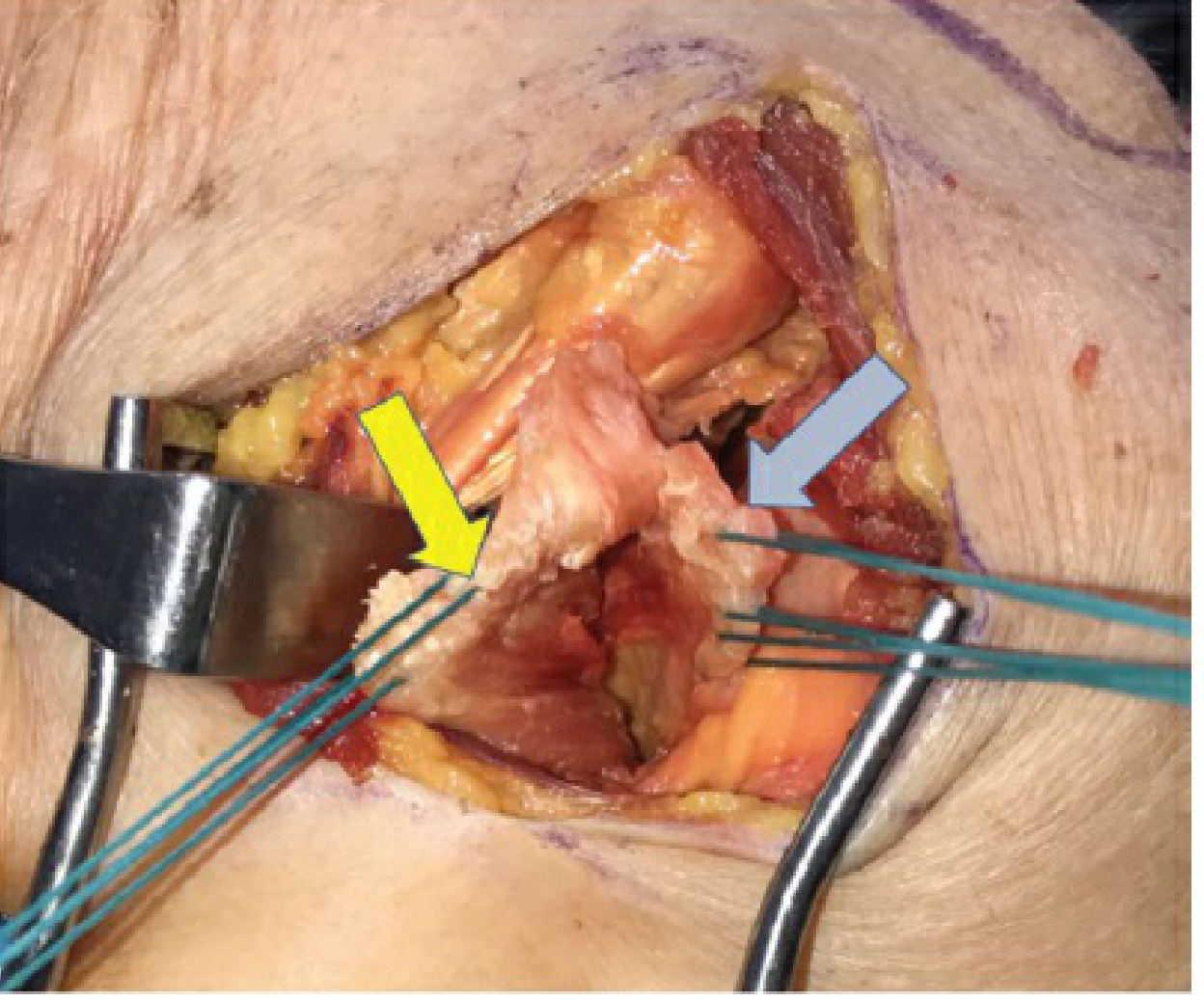
Yellow arrow = subscapularis muscle belly; gray/blue arrow = underlying joint capsule being separated bluntly. Sutures (teal) are placed for later subscapularis repair.
Intraoperative — Mini-Bankart: Preserved Inferior Subscapularis
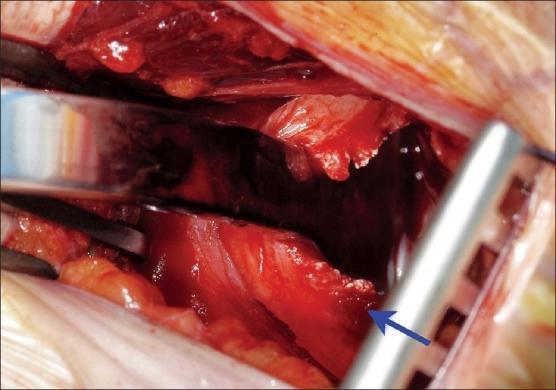
The blue arrow points to the preserved inferior third of the subscapularis tendon — a hallmark of the mini-Bankart approach that spares the lower fibers to maintain post-op stability.
Preoperative Skin Marking

Vertical line (~5 cm) lateral to the coracoid, extending toward the axillary fold, with the coracoid process circled as a palpable landmark.
Postoperative Scar

Well-approximated vertical scar ~5 cm in length, 2 cm lateral to the coracoid, in the early healing phase after open Bankart repair.
Source: Rockwood and Green's Fractures in Adults, 10th ed. 2025, Chapter 35 — Shoulder Stabilization Procedures.
Arthroscopic bankart repair images
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is the complete arthroscopic Bankart repair image series from Rockwood and Green's Fractures in Adults, 10th ed. (2025):
Arthroscopic Bankart Repair — Figure Series
Fig. 35-30A — Lateral Decubitus Positioning
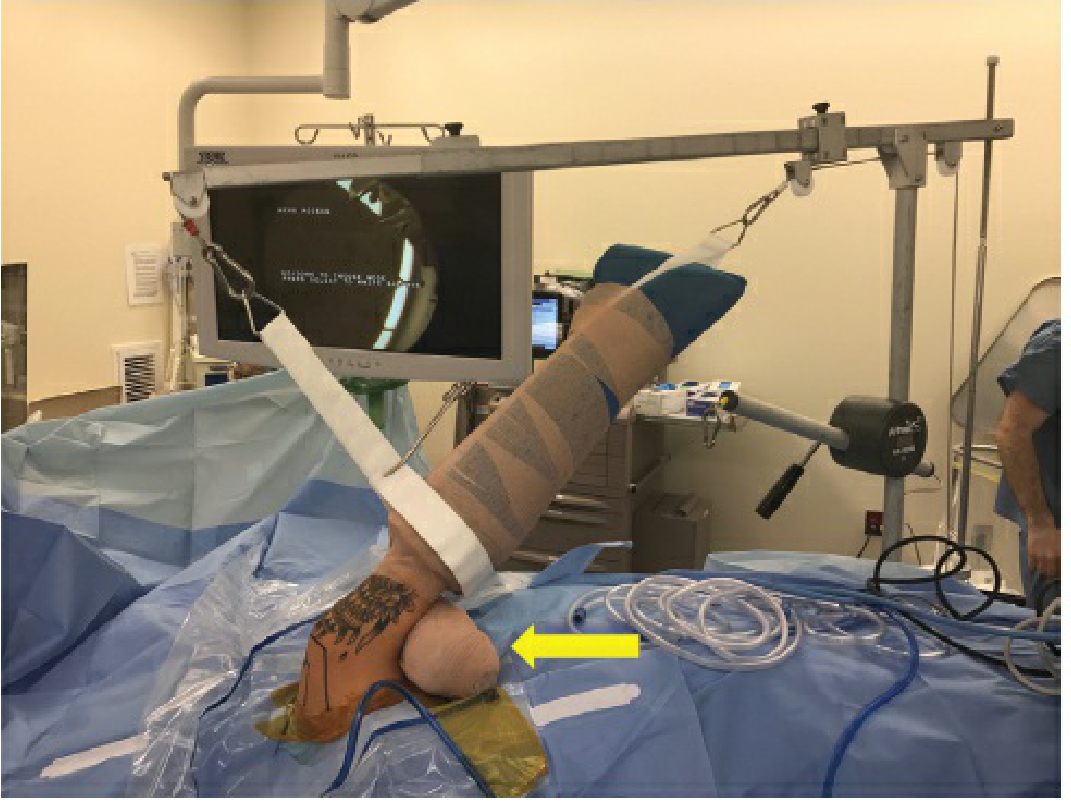
Patient in lateral decubitus with the operative arm in traction via a Coban-wrapped arm holder. Balanced traction (5–10 lb) applies both distraction and longitudinal pull. The yellow arrow points to the axillary bump placed to further distract the glenohumeral joint for improved visualization.
Fig. 35-30B — Posterior Portal & Posterolateral Accessory Portal

- Blue arrow = posterior viewing portal (~2 cm below, 1 cm medial to posterolateral acromion)
- Blue circle = posterolateral accessory portal for drilling/anchor placement in posterior labral repair — must be in line with the spine of the scapula to avoid glenoid penetration
Fig. 35-30C — Anterior Portals

- Blue arrow = anteroinferior (5:30) portal — suture passage and anchor drilling portal; requires 8-mm cannula for the curved metal passer
- Blue circle = anterosuperolateral portal — suture management and shuttling; placed just under the lateral acromion edge
Fig. 35-31 — Labral Mobilization and Anchor Placement (4-panel arthroscopic views)
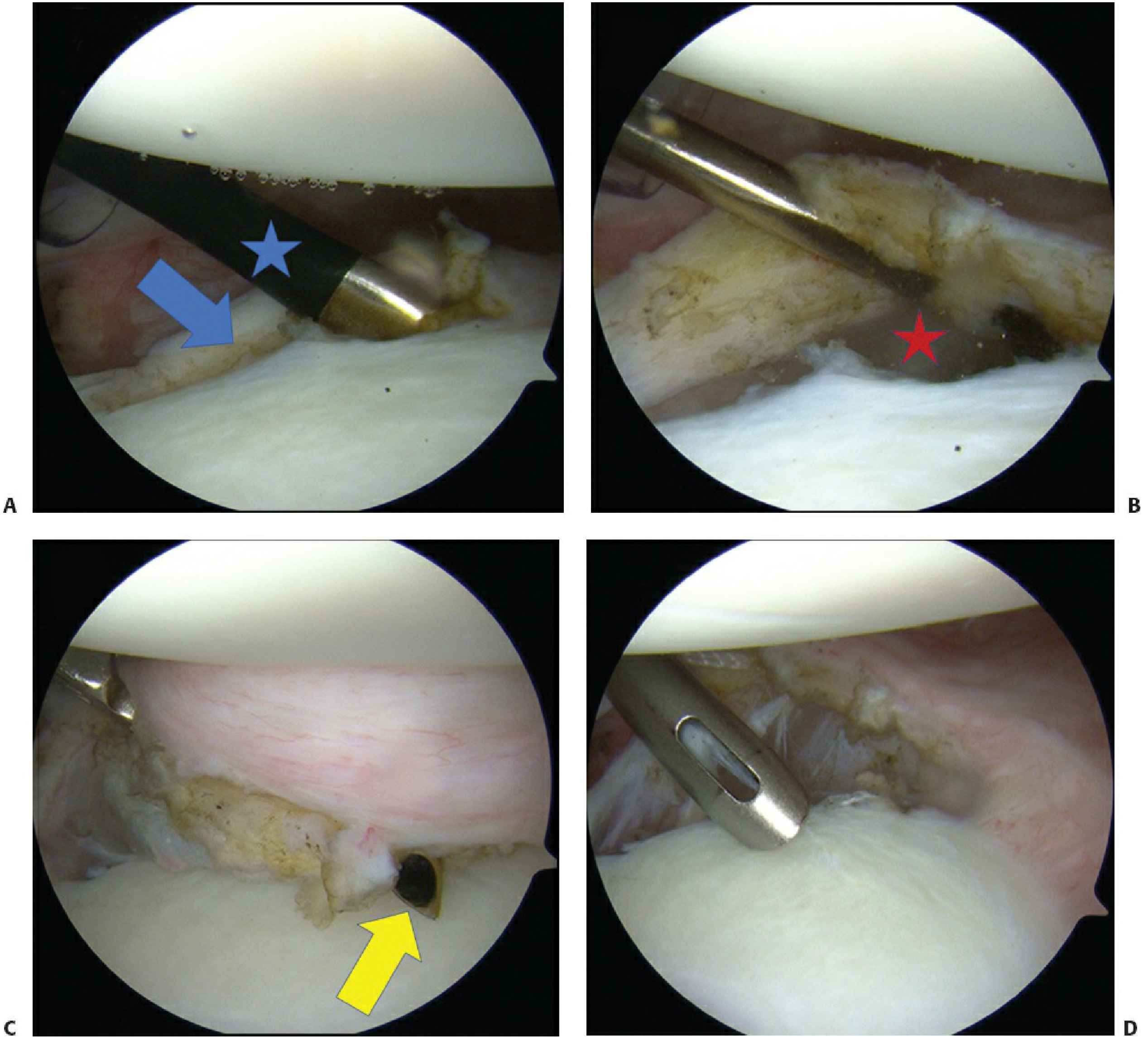
- A: Anteroinferior labral tear identified (blue arrow); CoVator (blue star) mobilizes the labrum off the glenoid neck
- B: Subscapularis muscle belly (red star) visualized below — confirms adequate capsulolabral shift will be achieved
- C: Curved metal-tipped passer (yellow arrow) penetrates capsule ~1 cm distal/away from glenoid rim to shift the capsulolabral complex
- D: First suture anchor placed low on the anteroinferior glenoid rim (critical position)
Fig. 35-32 — Knotless Labral Tape Fixation (4-panel)
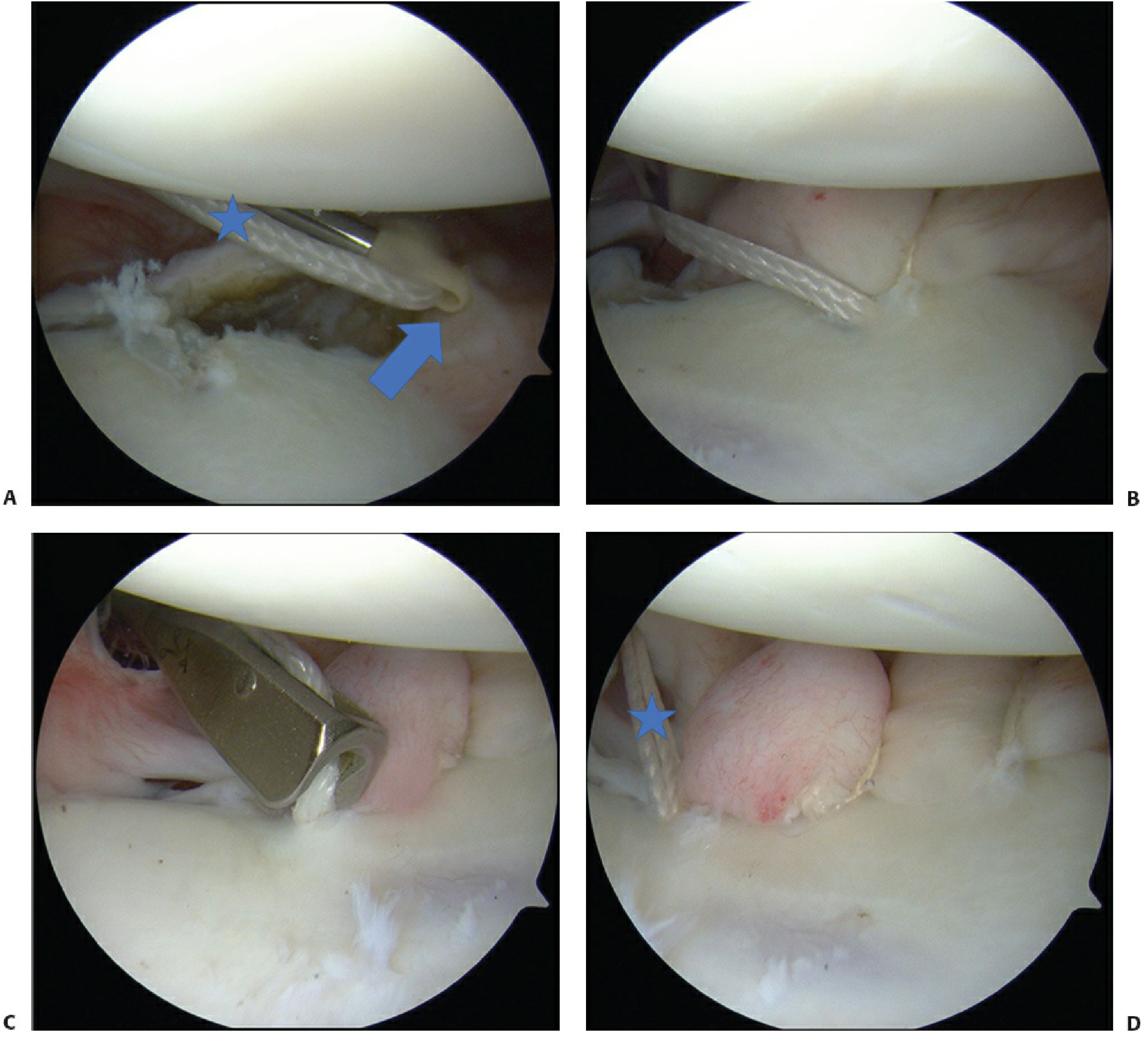
- A: Labral tape (star) shuttled across labrum and loaded onto 2.9-mm PushLock anchor (arrow)
- B: Anchor impacted into drill hole
- C: Labral tape cutter trims suture flush to glenoid rim
- D: Final repair — at least 3 knotless anchors used; a "bumper" is created at the end of the repair (star)
Fig. 35-33A — Hill-Sachs Lesion (Arthroscopic Evaluation)
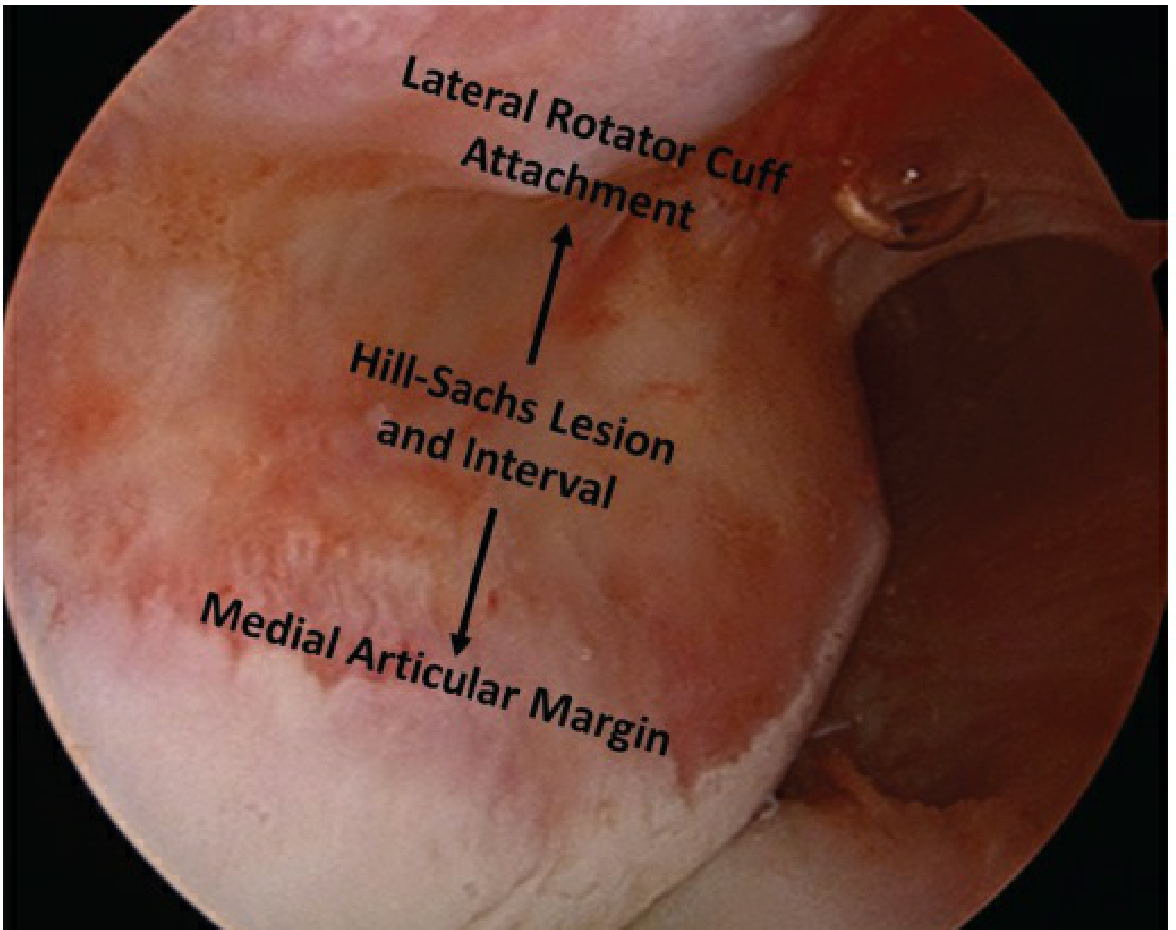
Arthroscopic view from the anterolateral portal showing the posterosuperior Hill-Sachs compression fracture. Landmarks labeled: lateral rotator cuff attachment (superior), Hill-Sachs lesion and interval (middle), medial articular margin (inferior).
Fig. 35-33B — Engaging Hill-Sachs Lesion
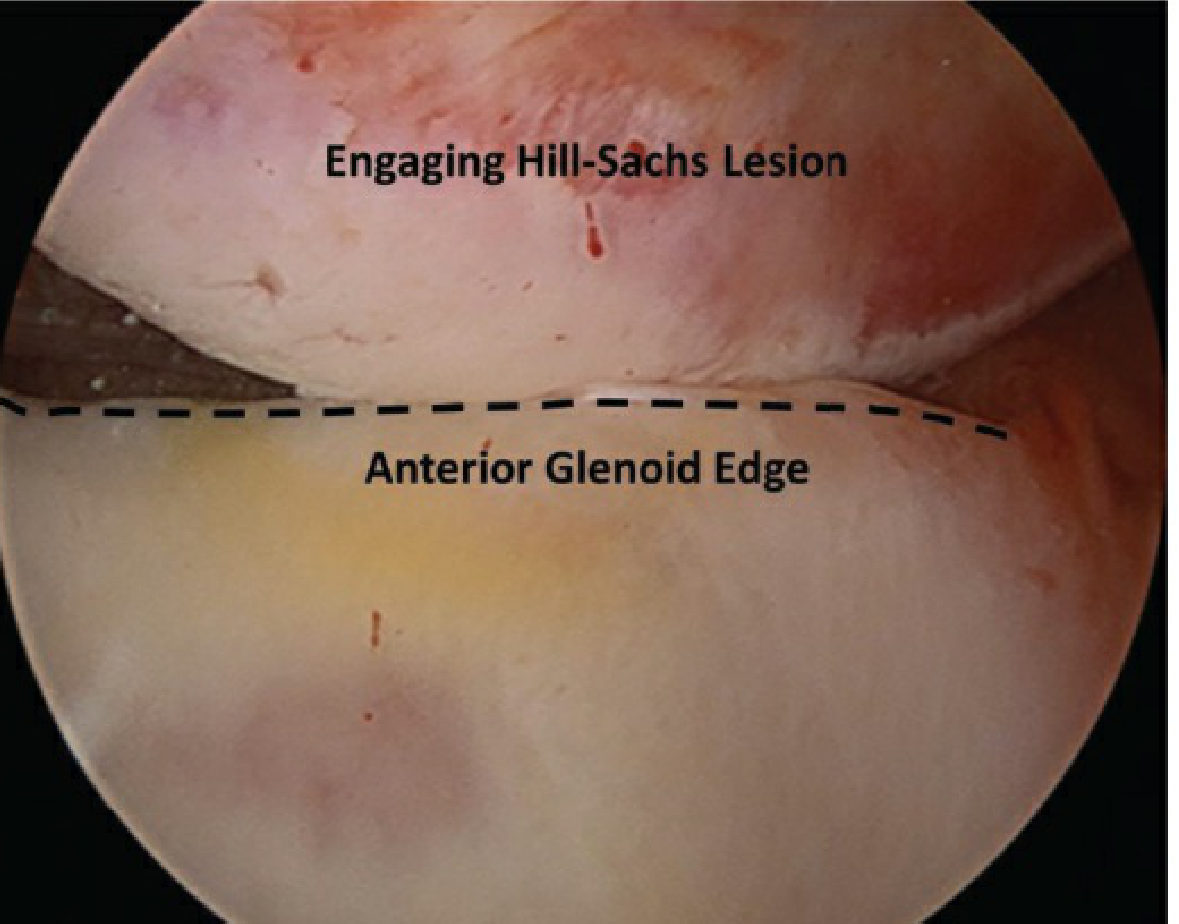
The Hill-Sachs defect is shown engaging the anterior glenoid edge (dashed line) — the "on-track/off-track" concept. When the lesion engages the glenoid rim in abduction/external rotation, remplissage is indicated alongside the Bankart repair.
Fig. 35-33D — Completed Remplissage (Infraspinatus Capsulotenodesis)
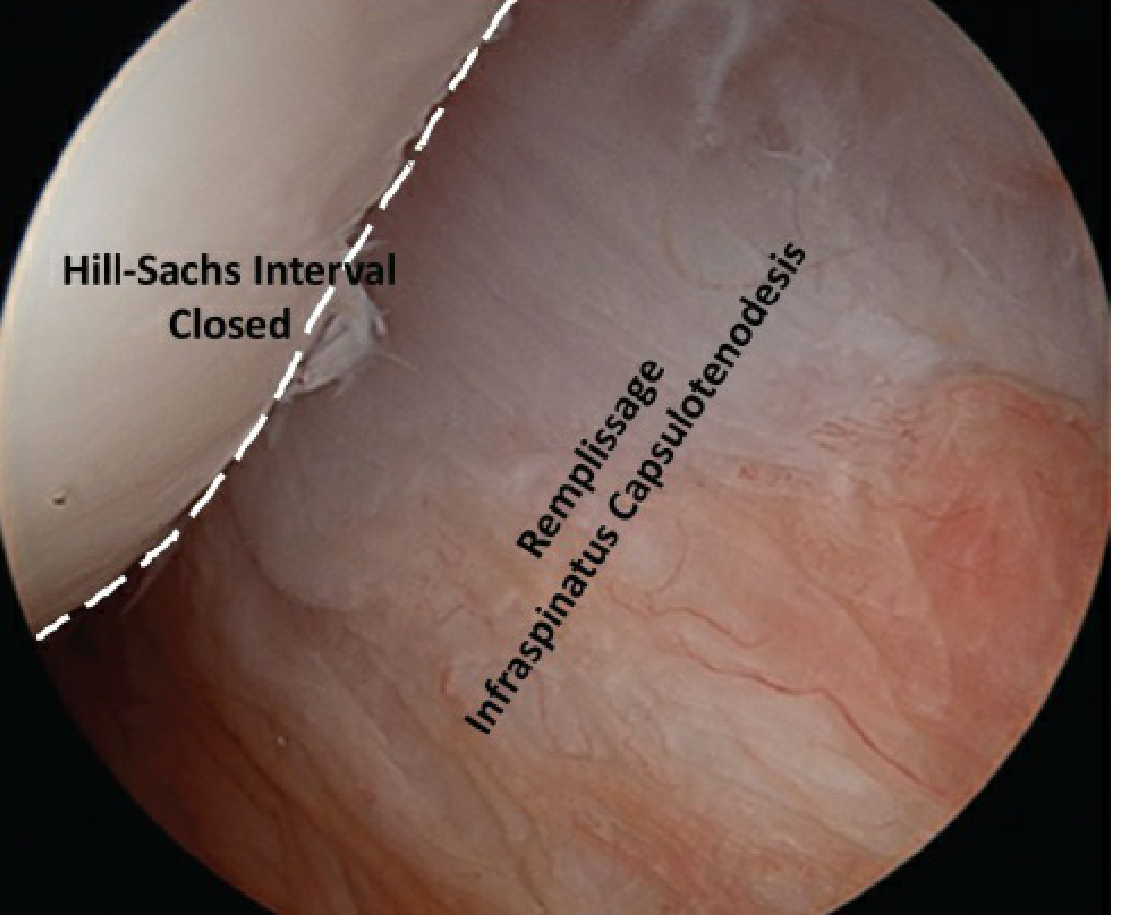
Final tensioning of the remplissage viewed from the anterolateral portal. The infraspinatus is tenodised into the Hill-Sachs defect, closing the interval and preventing engagement with the anterior glenoid. The result is labeled "Remplissage Infraspinatus Capsulotenodesis."
Source: Rockwood and Green's Fractures in Adults, 10th ed. 2025, Chapter 35 — Arthroscopic Anterior Labral (Bankart) Repair, Figs. 35-30 through 35-33.
This is a shared conversation. Sign in to Orris to start your own chat.