Facial nerve palsy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"facial nerve palsy" OR "Bell palsy"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I have rich content from multiple authoritative textbooks. Let me now compile the comprehensive answer.
Facial Nerve Palsy
Anatomy of the Facial Nerve (CN VII)
The facial nerve is one of the most anatomically complex cranial nerves. It originates from nuclei in the pons-medulla junction, enters the internal acoustic meatus, passes to the geniculate ganglion, and then courses through the Fallopian canal in the temporal bone. It exits the skull base via the stylomastoid foramen, enters the parotid gland, and fans out into five terminal branches (temporal, zygomatic, buccal, marginal mandibular, and cervical) supplying facial muscles. Along its intratemporal course, it gives rise to:
- Greater superficial petrosal nerve - carries parasympathetic fibers to the lacrimal gland
- Nerve to stapedius - stapedius reflex
- Chorda tympani - taste to anterior 2/3 of tongue; submandibular/sublingual salivary glands
Understanding where along this course a lesion sits determines the clinical picture. - Gray's Anatomy for Students
Upper vs. Lower Motor Neuron Lesion
| Feature | UMN (Supranuclear) | LMN (Nuclear/Infranuclear) |
|---|---|---|
| Forehead sparing | Yes (bilateral cortical input to upper face) | No - whole face involved |
| Side affected | Contralateral lower face | Ipsilateral entire face |
| Common causes | Stroke, tumors | Bell's palsy, Ramsay Hunt, trauma |
A primary brainstem lesion affecting the motor nucleus causes ipsilateral whole-face weakness. A lesion above the nucleus (e.g., cortical stroke) causes contralateral lower facial weakness with forehead sparing. - Gray's Anatomy for Students
Causes by Anatomical Level
Supranuclear (UMN)
- Stroke (most common in older adults)
- Brain tumor
- Multiple sclerosis
Nuclear / Fascicular (Brainstem)
- Demyelination (MS)
- Ischemia, hemorrhage
- Neoplasm
- Millard-Gubler syndrome (ipsilateral CN VI + VII palsy, contralateral hemiplegia)
Cerebellopontine Angle
- Acoustic schwannoma (hearing loss is usually the primary feature; facial weakness suggests facial schwannoma with a "labyrinthine tail" on MRI)
- Meningioma
- Facial nerve schwannoma
Intratemporal (Geniculate Ganglion and Below)
- Bell's palsy (idiopathic - most common cause of LMN facial palsy overall)
- Ramsay Hunt syndrome (herpes zoster oticus - VZV reactivation in geniculate ganglion)
- Acute otitis media / mastoiditis
- Temporal bone fracture
- Cholesteatoma, glomus tumor
- Lyme disease (Borrelia burgdorferi - can cause bilateral facial palsy)
- Sarcoidosis
Extracranial (Parotid, Face)
- Parotid gland tumors (malignant) - can track along the nerve perineural spread
- Trauma, surgery
- Parotiditis
Bell's Palsy
Bell's palsy is the most common cause of unilateral LMN facial palsy, accounting for approximately 60-75% of all cases. It is self-limited and typically monophasic.
Etiology: Reactivation of herpes simplex type 1 (HSV-1) in the geniculate ganglion causing inflammation, edema, and nerve compression within the tight bony Fallopian canal.
Clinical features:
- Acute-subacute onset, maximal within 72 hours
- Ipsilateral weakness of the entire face (forehead included)
- Pain in/around the ear (60% of patients)
- Impaired lacrimation (60%)
- Taste changes - anterior 2/3 tongue (30-50%)
- Hyperacusis (15-30%)
- Ipsilateral facial sensory symptoms (via trigeminal-facial nerve connection via greater superficial petrosal nerve)
- MRI may show enhancement of the facial nerve, most commonly at the geniculate ganglion
Prognosis: 85% of patients recover normal function spontaneously within 3 weeks. Residual deficits occur in ~12%, including persistent severe weakness (4%) and synkinesis (17%). Recurrence rate is ~13%; ipsilateral recurrence warrants suspicion for a tumor. - Bradley and Daroff's Neurology in Clinical Practice
Association with pregnancy: Bell's palsy occurs more frequently during pregnancy and is associated with a poorer recovery rate.
Ramsay Hunt Syndrome (Herpes Zoster Oticus)
Caused by VZV reactivation in the geniculate ganglion. More severe than Bell's palsy with worse prognosis.
- Triad: LMN facial palsy + herpetic vesicles in the ear (auricle/external auditory canal) + sensorineural hearing loss/vertigo
- Otalgia is often severe
- Treatment: prednisolone + acyclovir/valacyclovir (combination superior to steroids alone in this condition)
- Recovery rate is lower than Bell's palsy
Grading - House-Brackmann Scale
Endorsed by the American Academy of Otolaryngology - Head and Neck Surgery. Most widely used grading system.
| Grade | Description |
|---|---|
| I | Normal function |
| II | Slight dysfunction - mild weakness, complete eye closure with effort |
| III | Moderate dysfunction - obvious weakness, eye closure with effort, some forehead movement |
| IV | Moderately severe - disfiguring weakness, no forehead movement, incomplete eye closure |
| V | Severe dysfunction - barely perceptible movement |
| VI | Total paralysis - no movement |
Limitations: inter-observer disagreement 13-44% when a single global score is assigned; regional assessment (forehead, eye, nose, mouth separately) is more accurate. - Scott-Brown's Otorhinolaryngology
Key Clinical Red Flags
- Progressive palsy over >3 weeks - suspect underlying neoplasm
- Incomplete palsy not recovering after 3-6 weeks - suspect neoplasm
- Ipsilateral recurrence - 6 of 20 patients in one series had a tumor as the cause
- Bilateral concurrent palsy - think systemic: Guillain-Barré syndrome, sarcoidosis, Lyme disease, lymphoma, leukemia, Moebius syndrome
- Other cranial nerve signs (e.g., CN VI + VII = Gradenigo syndrome from petrous apex inflammation)
Investigations
| Suspected Cause | Investigation of Choice |
|---|---|
| Bell's palsy (typical) | Clinical diagnosis; MRI if atypical or progressive |
| Temporal bone fracture | HRCT temporal bone |
| Tumor (schwannoma, parotid malignancy) | MRI with gadolinium |
| Cholesteatoma / middle ear disease | HRCT temporal bone |
| Acute otitis media related | Clinical + CT if no response |
| Lyme disease | Serology |
| Sarcoidosis | ACE level, chest X-ray, MRI brain |
MRI notes: Contrast-enhanced T1-weighted MRI shows facial nerve enhancement (via the perineural arteriovenous plexus) - this can be normal at the geniculate ganglion and tympanic segments. In Bell's palsy, enhancement is most common at the geniculate ganglion. The intraparotid facial nerve is not identifiable on either CT or MRI directly. - Scott-Brown's Otorhinolaryngology
Electrodiagnostic testing: Electroneuronography (ENoG) - useful in complete paralysis cases to guide surgical decisions. Electromyographic presence of spontaneous fibrillation in facial muscles suggests significant axonal degeneration. - Bradley and Daroff's Neurology
Management
Bell's Palsy
Corticosteroids - mainstay of treatment
- First-line: Prednisolone (e.g., 50-60 mg/day x 10 days)
- Started within 72 hours of onset (ideally within 48 hours) for best outcomes
- Meta-analyses show 17% better chance of complete recovery compared to placebo; recovery rates 49-97% with steroids vs 23-64% untreated
- Evidence is less clear in children
Antiviral agents (acyclovir/valacyclovir)
- Combined with steroids for severe Bell's palsy
- A Cochrane review found combination therapy (antivirals + steroids) reduces synkinesis and excessive tearing compared to steroids alone
- However, the AAN guideline (2012) concluded antivirals alone add at most a 7% improvement in recovery; benefit, if any, is modest
- Benefit is clearer in Ramsay Hunt syndrome
Eye care - critical to prevent corneal exposure
- Lubricating eye drops/ointment
- Taping the eye closed at night
- Moisture chamber spectacles
- Tarsorrhaphy if permanent lagophthalmos (gold weight upper lid insertion for paralytic ectropion/facial nerve palsy is another option)
Surgical decompression
- Transmastoid decompression of tympanic/mastoid segments: abandoned (randomized trials showed no benefit; lesion is in the proximal labyrinthine segment, which this approach cannot reach)
- Decompression of the meatal foramen and labyrinthine segment (middle fossa approach): remains controversial; limited high-quality evidence
- In AOM-related palsy: ventilation tube insertion + IV antibiotics resolves ~80% of cases; cortical mastoidectomy for the remainder
Traumatic Facial Palsy
- Immediate palsy after trauma (complete, no chance of recovery without intervention): consider early exploration and decompression
- Delayed palsy: generally favorable prognosis; managed conservatively initially
- Facial nerve injury is usually at/just distal to the geniculate ganglion in longitudinal temporal bone fractures, and just proximal to the geniculate ganglion in transverse fractures
Sequelae and Aberrant Regeneration
- Synkinesis: involuntary co-contraction (e.g., eye closure when smiling) - affects ~17% after Bell's palsy; can worsen for up to 1 year
- "Crocodile tears" (gustatory lacrimation): aberrant regeneration of salivary fibers into lacrimal gland - tearing occurs during eating
- Hemifacial spasm: involuntary episodic contractions, often caused by vascular compression at the brainstem exit of CN VII; treat with botulinum toxin or microvascular decompression
- Contracture: hypertonia and shortening of the affected side, causing the nasolabial fold to deepen and palpebral fissure to narrow (paradoxically looks "normal" compared to the unaffected side at rest)
Recent Evidence (2024-2026)
Recent systematic reviews have examined adjunct therapies:
- Laser therapy for Bell's palsy (2024) found some evidence for low-level laser therapy in randomized trials, though quality of evidence remains limited [PMID: 39546047]
- Physical therapy for idiopathic facial paralysis (2025) supports neuromuscular retraining, mime therapy, and facial exercise in recovery [PMID: 39647183]
- Traumatic facial palsy management (2025) systematic review confirms outcomes vary by mechanism and timing of intervention [PMID: 40287586]
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2 | Bradley and Daroff's Neurology in Clinical Practice | Cummings Otolaryngology Head and Neck Surgery | Gray's Anatomy for Students | Kanski's Clinical Ophthalmology
Demyelination means
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough explanation drawn from multiple authoritative neurology and pathology textbooks.
Demyelination
Definition
Demyelination is the focal destruction or loss of the myelin sheath surrounding a nerve axon, while the axon itself is initially preserved (at least in the early stages). The word literally means "removal of myelin."
Myelin is a lipid-rich, multi-layered membrane wrapped around axons by:
- Oligodendrocytes - in the CNS (each oligodendrocyte myelinates multiple axons)
- Schwann cells - in the PNS (each Schwann cell myelinates one internode of one axon)
Its primary function is to act as an electrical insulator, enabling saltatory conduction - the rapid "jumping" of electrical impulses from one node of Ranvier to the next. - Bradley and Daroff's Neurology in Clinical Practice
The Normal Myelin System
In a myelinated nerve:
- The axon is wrapped in segments called internodes (between consecutive nodes of Ranvier)
- Voltage-gated Na⁺ channels are concentrated at the nodes of Ranvier, not in the internodal membrane
- An action potential at one node generates ionic current that flows under the myelin to the next node and fires it - this is saltatory conduction
- K⁺ channels help terminate the current and repolarize the axon
- Safety factor for transmission is normally 5-7 times above threshold - highly reliable
What Happens When Myelin is Lost
When myelin is stripped away from an internode, the crucial electrical insulation is gone:
- Current leaks out through the now-exposed internodal axon membrane instead of jumping to the next node
- Conduction slows dramatically or fails altogether (conduction block)
- The widening of nodes of Ranvier is the earliest change, causing initial slowing of conduction velocity
- More severe demyelination causes conduction block - complete failure of impulse transmission across the affected segment
- Asynchronous conduction in different fibers within the same nerve bundle can abolish functions that depend on synchronized firing (e.g., deep tendon reflexes, vibration sense), causing paresthesias
"The main physiologic effect of demyelination is to impede saltatory electrical conduction of nerve impulses from one node of Ranvier... to the next node." - Adams and Victor's Principles of Neurology
The Key Diagram: Three Types of Nerve Pathology
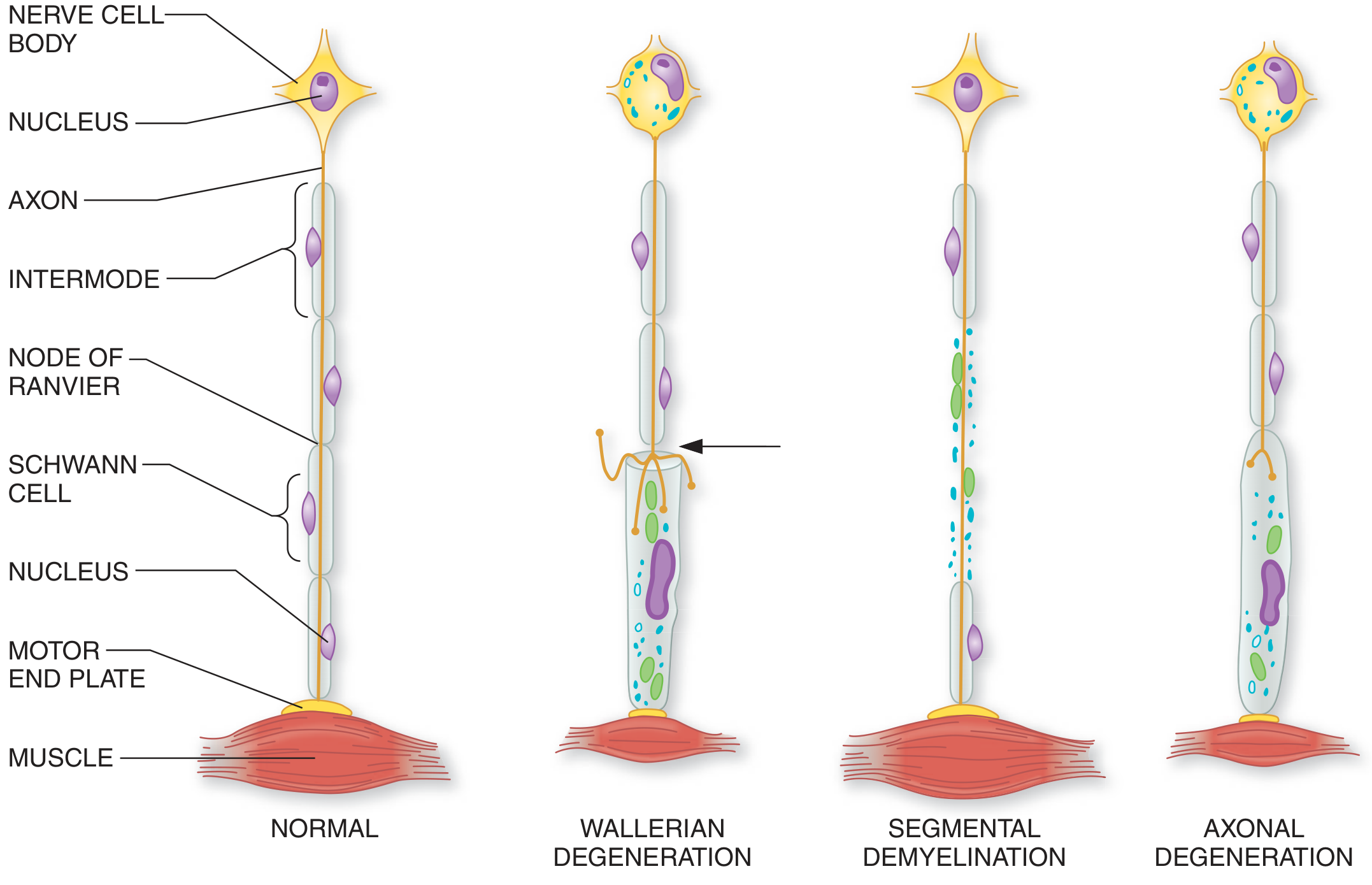
From Adams and Victor's Principles of Neurology - showing Normal, Wallerian Degeneration, Segmental Demyelination, and Axonal Degeneration side by side
Segmental Demyelination (Classic Form)
The characteristic pattern in most demyelinating diseases:
-
The myelin sheath disappears over segments of variable length, bounded on each end by a node of Ranvier
-
The axon is spared - this is what distinguishes it from Wallerian degeneration
-
Schwann cells (or oligodendrocytes) survive and can attempt remyelination, but new myelin sheaths are thinner and shorter - yielding permanently slower conduction velocity even after "recovery"
-
Adams and Victor's Principles of Neurology
Demyelination vs. Other Nerve Pathology
| Feature | Segmental Demyelination | Wallerian Degeneration | Axonal Degeneration |
|---|---|---|---|
| What is lost | Myelin only (axon spared) | Axon + myelin distal to injury ("dying forward") | Axon + myelin from distal tip inward ("dying back") |
| Axon integrity | Preserved | Destroyed | Destroyed |
| Cause example | MS, GBS, compression | Nerve transection, trauma | Toxic/metabolic neuropathy |
| Recovery | Possible via remyelination | Requires axonal regrowth (slow, ~1mm/day) | Variable |
| Muscle atrophy | Not initially | Yes | Yes |
Physiological Consequences
- Uhthoff phenomenon (classic in MS): temporary worsening of symptoms with increased body temperature or exercise, because a partially demyelinated axon's safety margin drops below threshold when temperature rises slightly
- Evoked potential delays: demyelination of the optic nerve causes prolonged visual evoked potential latencies - a key diagnostic finding in MS
- Recovery after acute demyelination: in the short term (days), recovery reflects subsidence of edema and inflammation, not true remyelination. Remyelination is a slower, partial process
Causes of Demyelination
CNS Demyelination
| Disease | Mechanism |
|---|---|
| Multiple sclerosis (MS) | Autoimmune T-cell mediated attack on oligodendrocytes/myelin |
| Neuromyelitis optica (NMO) | Anti-AQP4 antibodies (astrocyte injury → secondary demyelination) |
| Acute disseminated encephalomyelitis (ADEM) | Post-infectious/post-vaccine monophasic immune attack |
| Progressive multifocal leukoencephalopathy (PML) | JC virus destroying oligodendrocytes |
| Osmotic demyelination syndrome (central pontine myelinolysis) | Rapid correction of hyponatremia |
| Leukodystrophies | Genetic enzyme defects affecting myelin synthesis |
PNS Demyelination
| Disease | Mechanism |
|---|---|
| Guillain-Barré syndrome (GBS) | Autoimmune attack on PNS myelin (often post-infectious) |
| Chronic inflammatory demyelinating polyneuropathy (CIDP) | Chronic autoimmune PNS demyelination |
| Charcot-Marie-Tooth disease (type 1) | Genetic PMP22 duplication - abnormal myelin production |
| Diphtheria | Exotoxin cleaves myelin proteins |
| Compression neuropathy | Mechanical distortion of myelin at the node of Ranvier |
Key Difference: Demyelination vs. Axonal Loss
This distinction matters clinically and on nerve conduction studies (NCS):
- Demyelination → Slowed conduction velocity + prolonged distal latency + conduction block on NCS; muscle bulk and power relatively preserved early; good recovery potential
- Axonal loss → Reduced amplitude of compound muscle/sensory action potentials on NCS; muscle wasting and weakness more prominent; poorer recovery
Sources: Adams and Victor's Principles of Neurology 12th Ed | Bradley and Daroff's Neurology in Clinical Practice | Basic Medical Biochemistry 6e | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.