Regulation of thyroid hormone
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks plus the diagrams. Let me compile the full answer.
Regulation of Thyroid Hormone
1. Overview: The HPT Axis
Thyroid hormone regulation is governed by a three-tier hypothalamic-pituitary-thyroid (HPT) axis, with tight negative feedback at every level. The goal is to maintain a metabolic rate that is optimal for normal body function.
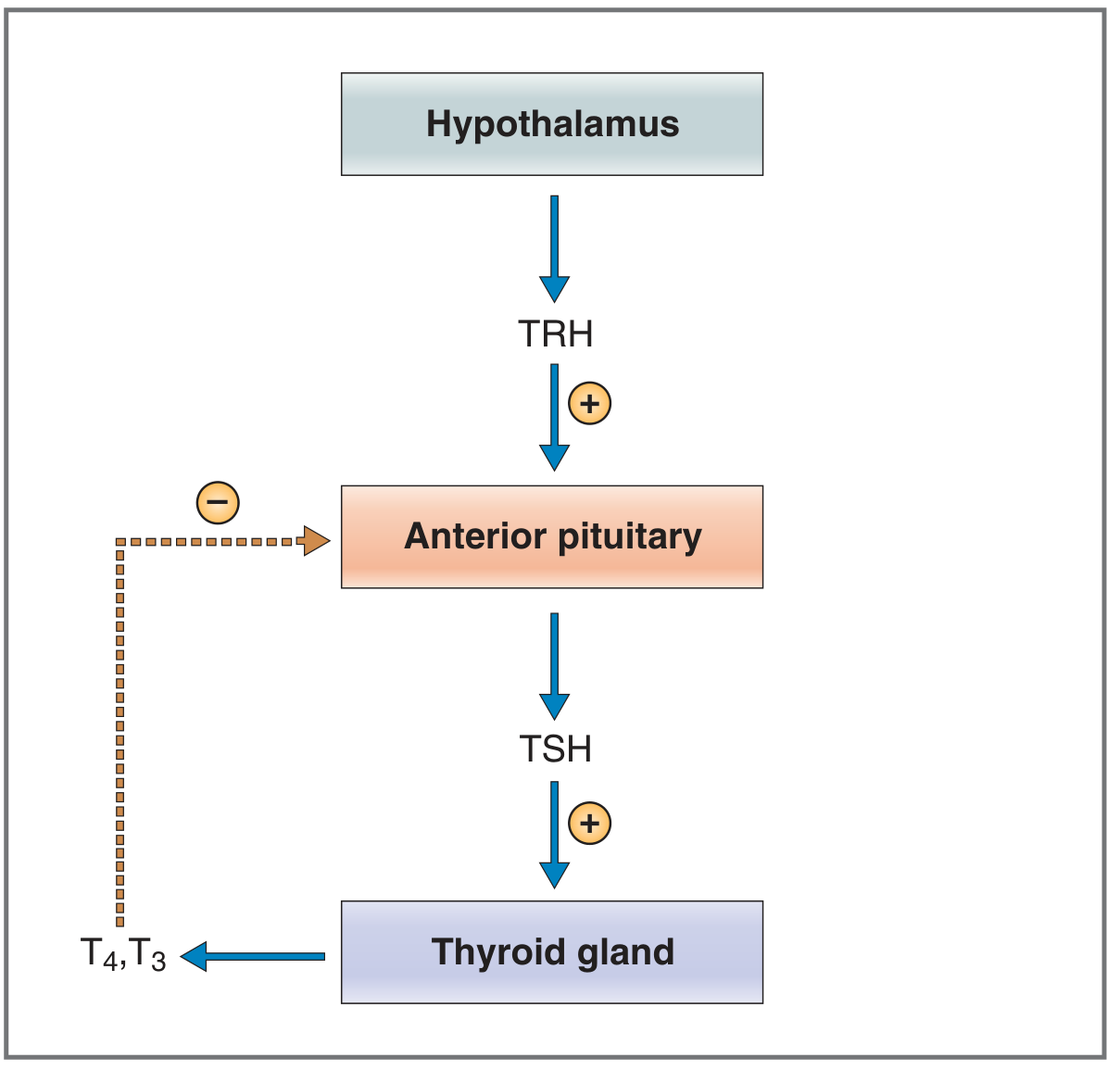
Fig. 9.19 - Regulation of thyroid hormone secretion (Costanzo Physiology, 7th Ed.)
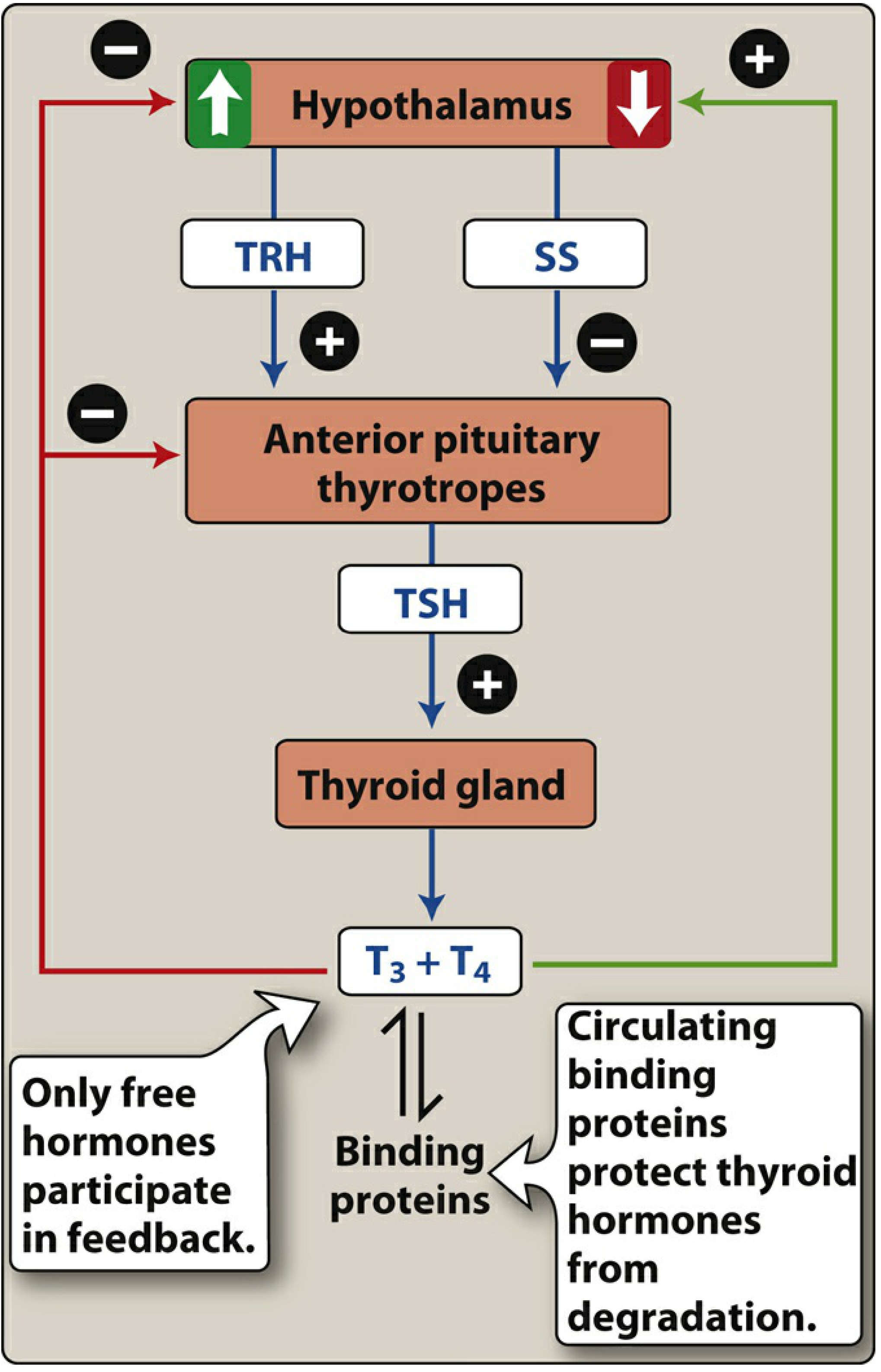
Fig. 23.8 - Feedback regulation of thyroid hormone release (Lippincott Illustrated Reviews: Pharmacology)
2. Hypothalamus: TRH
Thyrotropin-releasing hormone (TRH) is a tripeptide (pyroglutamyl-histidyl-proline-amide) secreted by neurons in the paraventricular nucleus (PVN) of the hypothalamus. It is released into the hypothalamic-hypophysial portal blood and travels to the anterior pituitary.
TRH acts on thyrotrophs of the anterior pituitary via a Gq/phospholipase C mechanism, generating IP3/DAG and releasing intracellular Ca²+, which leads to TSH secretion. TRH also stimulates transcription of the TSH gene.
Factors that increase TRH secretion:
- Exposure to cold (via hypothalamic thermoregulatory centers - a well-known stimulus, capable of raising BMR by 15-20%)
- Leptin (via POMC neurons in the arcuate nucleus)
Factors that decrease TRH secretion:
- Prolonged fasting - reduced leptin reduces POMC activity and directly inhibits TRH neurons
- High thyroid hormone levels (long-loop negative feedback)
- Somatostatin (SS) - inhibits both TRH output and TSH release at the pituitary
- Emotional stress/sympathetic activation (excitement, anxiety) - acutely decreases TSH output
(Guyton & Hall, Medical Physiology; Lippincott Pharmacology)
3. Anterior Pituitary: TSH (Thyrotropin)
TSH is a glycoprotein (~28,000 Da) secreted by thyrotrophs of the anterior pituitary. It is the central regulator of thyroid gland activity.
TSH's actions on the thyroid gland (via cAMP second messenger):
TSH binds to Gs protein-coupled TSH receptors on the basolateral membrane of thyroid follicular cells → activates adenylyl cyclase → ↑ cAMP → protein kinase activation → multiple phosphorylations:
- Increased proteolysis of stored thyroglobulin → immediate release of T3/T4 into blood (within 30 minutes)
- Activation of the iodide pump (Na⁺/I⁻ symporter) → increased iodide trapping (intracellular:extracellular I⁻ ratio up to 8× normal)
- Increased iodination of tyrosine residues
- Increased size and secretory activity of thyroid follicular cells
- Increased number of thyroid cells (hypertrophy and hyperplasia); cuboidal → columnar morphology with increased infolding of the epithelium
(Guyton & Hall, Medical Physiology, p. 937)
4. Thyroid Gland: Hormone Synthesis
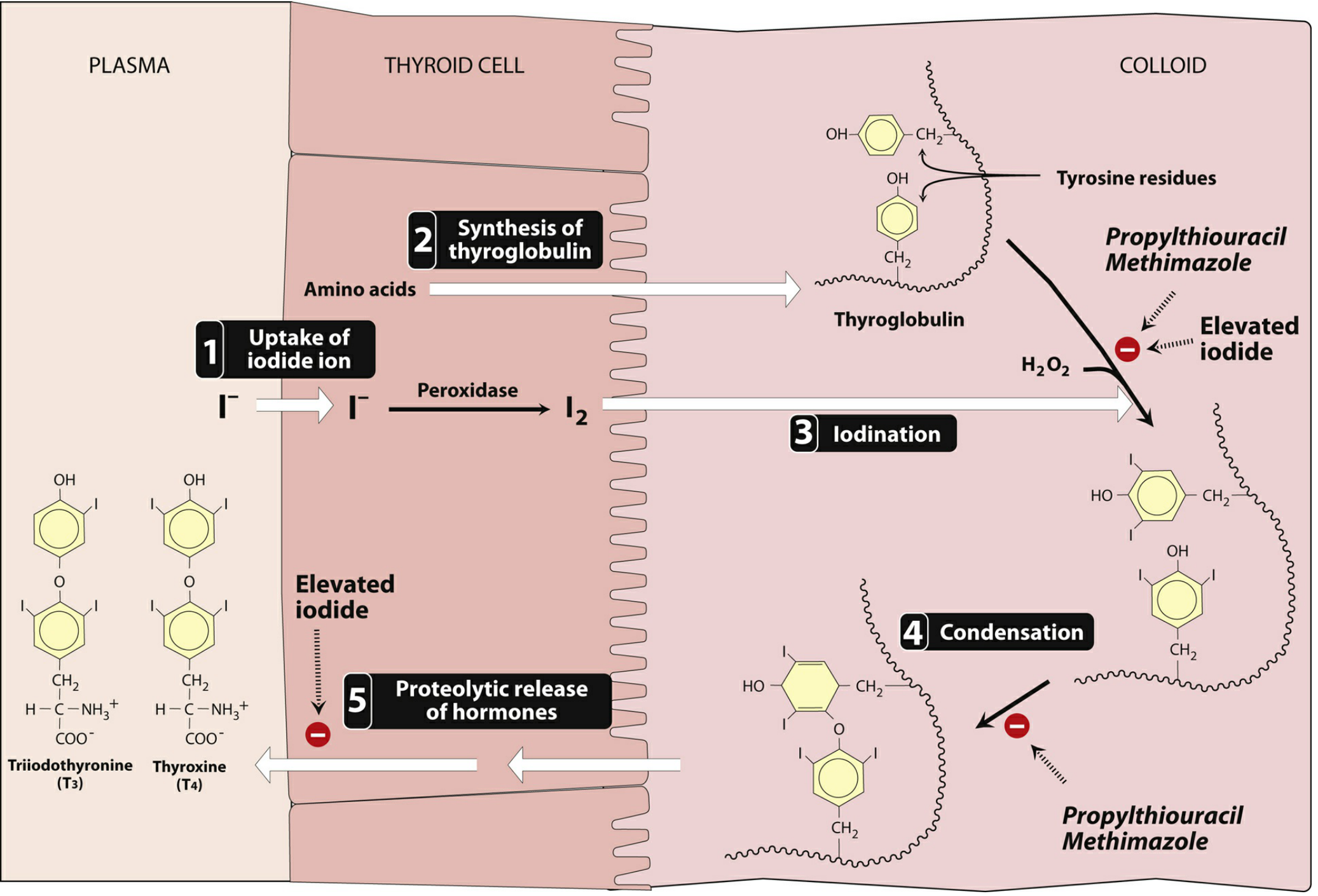
Fig. 23.9 - Biosynthesis of thyroid hormones (Lippincott Illustrated Reviews: Pharmacology)
The 5 key steps in thyroid hormone synthesis:
| Step | Process |
|---|---|
| 1 | Iodide uptake - Na⁺/I⁻ symporter on basolateral membrane traps I⁻ from plasma |
| 2 | Thyroglobulin synthesis - large glycoprotein (~660 kDa) assembled in follicular cells, secreted into colloid |
| 3 | Iodination (organification) - thyroid peroxidase (TPO) oxidizes I⁻ → I₂; iodination of tyrosine residues on thyroglobulin forms MIT (monoiodotyrosine) and DIT (diiodotyrosine) |
| 4 | Condensation (coupling) - TPO couples two DIT → T4; one MIT + one DIT → T3 |
| 5 | Proteolytic release - follicular cells endocytose colloid; lysosomes cleave thyroglobulin, releasing T3 and T4 into the blood |
5. Peripheral Conversion: T4 → T3
The major secretory product is T4 (thyroxine), which is the less active form. In target tissues, the enzyme 5'-iodinase (type I deiodinase) removes one iodine atom from the outer ring of T4, converting it to the active T3.
A portion of T4 is instead converted to reverse T3 (rT3) by removing iodine from the inner ring - rT3 is metabolically inactive.
Important modulator - starvation:
- Fasting inhibits 5'-iodinase in peripheral tissues (e.g., skeletal muscle) → less T3 produced → reduced O₂ consumption and BMR (energy conservation)
- Brain 5'-iodinase is isoform-distinct and is NOT inhibited by starvation, protecting cerebral T3 levels
(Costanzo Physiology, 7th Ed., p. 426)
6. Negative Feedback
This is the master control mechanism:
- T3 and T4 (free forms) feed back to suppress TSH secretion from the anterior pituitary
- T3 acts via nuclear thyroid hormone receptors (TRβ2 isoform) in thyrotrophs → suppresses the TSH-β gene
- When thyroid hormone output rises to ~1.75× normal, TSH secretion falls to near zero
- This feedback operates directly at the pituitary - it persists even after pituitary-hypothalamus disconnection
- Only free (unbound) hormones participate in feedback - protein-bound hormone is biologically inert
(Guyton & Hall; Ganong's Review, 26th Ed.)
7. Plasma Binding Proteins
Most circulating T3 and T4 is protein-bound. Binding proteins protect hormones from degradation and maintain a large reservoir.
| Protein | Plasma Concentration | % T4 Bound | % T3 Bound |
|---|---|---|---|
| Thyroxine-binding globulin (TBG) | 2 mg/dL | 67% | 46% |
| Transthyretin (TBPA) | 15 mg/dL | 20% | ~0% |
| Albumin | ~4,000 mg/dL | 13% | ~54% |
Key facts:
- 99.98% of plasma T4 is bound; free T4 ≈ 2 ng/dL
- T4 half-life: ~6-7 days (prolonged due to protein binding)
- T3 is less tightly bound, more rapidly dissociates → faster onset of action
- Clinical: only free T4 and free T3 are physiologically active and clinically meaningful to measure
(Ganong's Review of Medical Physiology, 26th Ed.)
8. Summary: Factors Affecting Thyroid Hormone Output
| Stimulatory | Inhibitory |
|---|---|
| TSH | Iodide deficiency |
| Thyroid-stimulating immunoglobulins (TSI, in Graves' disease) | Excessive iodide intake (Wolff-Chaikoff effect) |
| Cold exposure | Perchlorate, thiocyanate (block Na⁺/I⁻ cotransporter) |
| Increased TBG levels (e.g., pregnancy) | Propylthiouracil / methimazole (inhibit TPO) |
| Leptin / adequate nutrition | Fasting / low leptin |
| Somatostatin | |
| Decreased TBG (e.g., liver disease) |
(Costanzo Physiology, 7th Ed., Table 9.8)
9. Wolff-Chaikoff Effect (Special Regulatory Mechanism)
Acutely high plasma iodide paradoxically inhibits thyroid hormone synthesis. The mechanism involves high intracellular I⁻ suppressing TPO activity. This effect is transient - the thyroid normally "escapes" by downregulating the Na⁺/I⁻ symporter. This phenomenon is exploited clinically (e.g., Lugol's iodine pre-operatively in Graves' disease, or potassium iodide in radiation emergencies).
Sources:
- Costanzo Physiology, 7th Edition, pp. 424-426
- Guyton and Hall Textbook of Medical Physiology, pp. 936-939
- Ganong's Review of Medical Physiology, 26th Edition, Chapter 20
- Lippincott Illustrated Reviews: Pharmacology, Chapter 23
This is a shared conversation. Sign in to Orris to start your own chat.