Frontal sinus- anatomical variations, anatomy of fronto ethnoidal complex, frontal recess and onodi cells according to standard ent textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Excellent - I have comprehensive information and diagrams. Now I have everything needed to compose a detailed, well-structured answer. Let me compile it all:
Frontal Sinus: Anatomy, Anatomical Variations, Fronto-Ethmoidal Complex, Frontal Recess, and Onodi Cells
1. FRONTAL SINUS - BASIC ANATOMY AND DEVELOPMENT
Embryology and Development
The frontal sinus originates from an anterior ethmoidal cell. Pneumatization of the frontal bone begins during the 16th week of gestation. At birth, the frontal sinuses appear as only a small blind pocket, difficult to distinguish from anterior ethmoid air cells on imaging. With gradual pneumatization:
- Radiologically visible in most children by age 8 years
- Significant pneumatization occurs in early adolescence
- Development continues until 18 years of age
- Adult proportions are essentially reached by age 10-12 years
The connection between the frontal sinus and the anterior ethmoidal complex is not a tube or duct - it is an hourglass-shaped three-dimensional space called the frontal recess. Its narrowest part is conventionally called the "frontal ostium," though this is not a true two-dimensional opening. The term "frontal opening" has been recently proposed as more accurate.
(Cummings Otolaryngology, p. 871; Scott-Brown's Vol 1, p. block9)
2. ANATOMICAL VARIATIONS OF THE FRONTAL SINUS
The frontal sinus is the most variable paranasal sinus in terms of size and shape. Key variations include:
Size and Pneumatization Variants
| Variation | Description |
|---|---|
| Aplasia | Complete absence of one or both frontal sinuses (present in ~5% of individuals unilaterally or bilaterally) |
| Hypoplasia | Underdevelopment, sinus present but small |
| Asymmetry | Extremely common - the two sinuses almost never equal in size |
| Supraorbital extension | Extensive pneumatization extending far laterally over the orbit |
| Intersinus septum variations | Septum may be midline, deviated, or absent; may contain accessory septa dividing sinus into multiple compartments |
| Scalloped/multicompartmental | Irregular internal bony partitions dividing the sinus |
Mucociliary Flow Pattern (Messerklinger, 1955)
Mucus flows up the intersinus septum → across the frontal sinus roof laterally → medially along the floor → to the frontal ostium → down into the frontal recess. An estimated 40-60% of this mucus flows back up the medial frontal recess wall and recirculates. This explains why drilling a hole in the intersinus septum may not always improve drainage.
(Cummings Otolaryngology, p. 871)
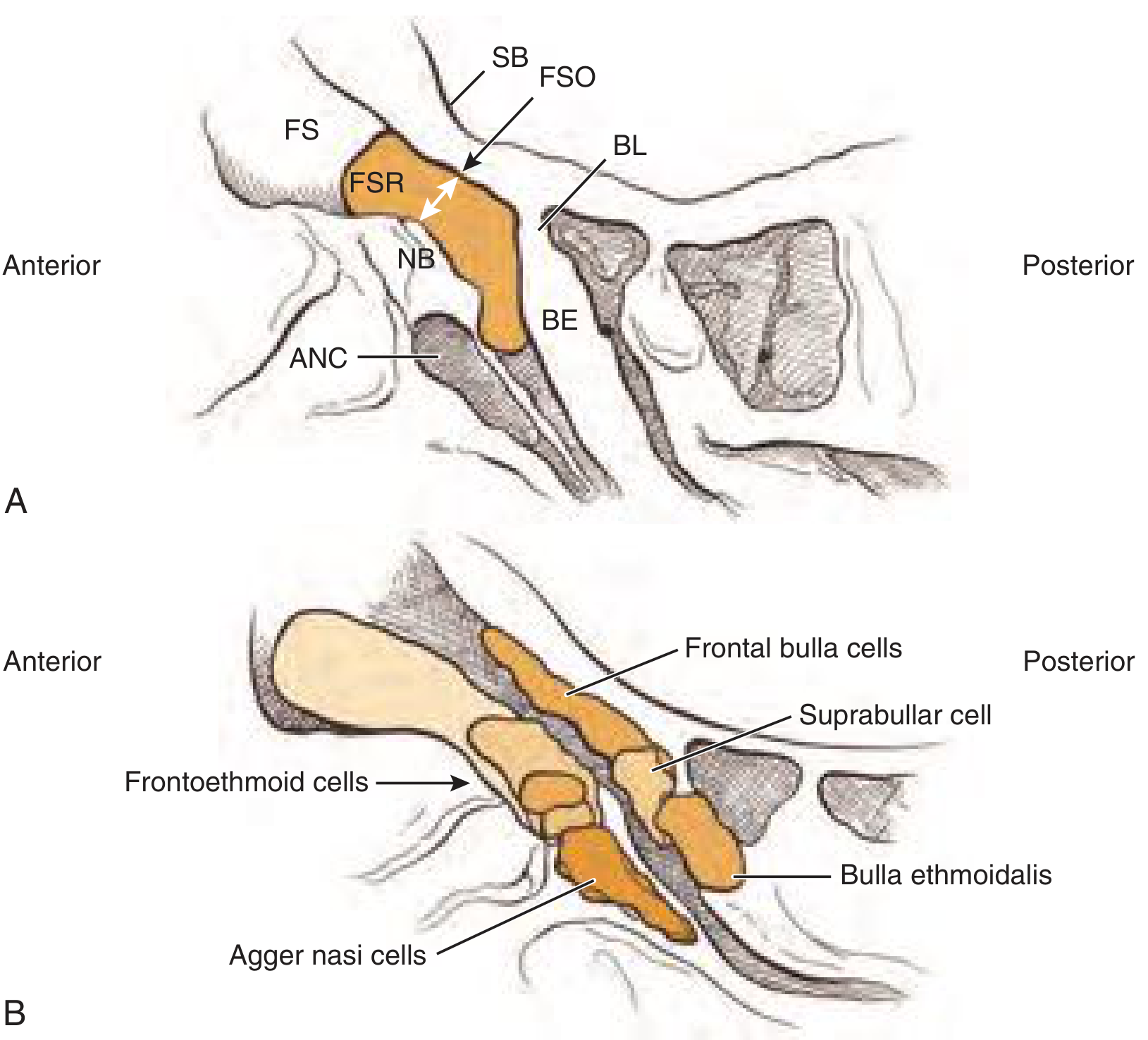
3. THE FRONTO-ETHMOIDAL COMPLEX
The fronto-ethmoidal complex refers to the anatomical region where the frontal sinus interfaces with the anterior ethmoid labyrinth. Understanding this region is the foundation of frontal sinus surgery.
Key Structural Components
Agger Nasi Cell (ANC)
- The most anterior ethmoidal air cell, present in over 90% of patients
- Its posterior wall forms the anterior boundary of the frontal recess
- The degree of agger nasi pneumatization directly influences the position of the superior uncinate process and the thickness of the nasofrontal beak
- Endoscopically appears as a bulge at the middle turbinate attachment
Uncinate Process
- Crescent-shaped bony structure whose superior attachment determines the direction of frontal sinus drainage
- Attachment patterns (Scott-Brown; multiple attachments in >50% of cases):
- Medial orbital wall (lamina papyracea): 85% of cases → frontal drainage is medial to the uncinate
- Skull base: 10% of cases → frontal drainage is lateral to the uncinate
- Middle turbinate: → frontal drainage is lateral to the uncinate
- Combination attachments: ~57% of cases
- The classic teaching of three distinct uncinate attachments is "neither surgically relevant nor accurate" (Wormald/Scott-Brown)
- Surgical rule: The frontal recess is medial to the remnant uncinate ("vertical bar") in 85% of cases
Bulla Ethmoidalis
- The largest and most constant anterior ethmoidal cell
- Forms the posterior boundary of the frontal recess when it extends to the skull base
- The bulla lamella is the posterior wall of the bulla; if absent superiorly, the suprabullar space communicates directly with the frontal recess (placing the anterior ethmoidal artery at risk during dissection)
Anterior Ethmoidal Artery
- Traverses the skull base from lateral-posterior to medial-anterior
- More likely to lie in a mesentery (suspended below the skull base) when olfactory fossa depth >4 mm (Keros II-III)
- From anterior to posterior, lies just behind the bulla ethmoidalis or any stacked cells above it
- On CT: "nipple sign" - pierces medial orbit just posterior to the globe where the superior oblique and medial rectus are closely adjacent
(KJ Lee's Essential Otolaryngology, p. 608; Scott-Brown's Vol 1, p. 1129)
4. THE FRONTAL RECESS
The frontal recess is the most anterior and superior aspect of the anterior ethmoid sinus that forms the connection with the frontal sinus. It is not the same as the frontal sinus drainage pathway - the frontal recess is the inferior part of the drainage pathway, lying inferior to the frontal ostium.
Boundaries
| Wall | Structure |
|---|---|
| Anterior | Posterior-superior wall of agger nasi cell (when present); frontal process of maxilla and nasofrontal beak |
| Posterior | Anterior wall of the ethmoid bulla (if it extends to skull base); bulla lamella |
| Lateral | Lamina papyracea |
| Medial | Superior attachment of middle turbinate; lateral lamella of the cribriform plate |
| Superior | Communicates with the frontal sinus at the frontal ostium; posterior to this, roof is the fovea ethmoidalis |
The frontal recess has an hourglass configuration: it tapers as it approaches the frontal ostium superiorly, then widens again into the frontal sinus as the anterior and posterior tables diverge.
Drainage Pathway
The frontal sinus drains through the frontal recess into:
- The middle meatus (most common)
- The superior aspect of the infundibulum (less common)
Most commonly the recess opens just medial to the posterior aspect of the uncinate process.
(KJ Lee's Essential Otolaryngology, p. 608; Cummings, p. 871)
5. FRONTAL RECESS CELLS (FRONTOETHMOIDAL CELLS)
The frontal sinus drainage pathway is frequently filled with anterior ethmoidal cells called frontal recess cells. These cells pneumatize around the frontal recess and can narrow or obstruct drainage.
The Paranasal Surgical Box (Scott-Brown)
The vertical portion of the paranasal surgical box defines the anatomical limits of frontal recess dissection:
- Medially: Intersinus septum and middle turbinate
- Laterally: Lamina papyracea
- Anteriorly: Nasofrontal beak
- Posteriorly: Skull base
Classification Systems
A. Kuhn Classification (Classic) - with IFAC equivalents
ANTERIOR CELLS (anterior to the frontal recess):
| Type | Kuhn Name | IFAC Name | Description |
|---|---|---|---|
| Type 1 | Frontal cell type 1 | Agger nasi cell (ANC) | A single cell superior to the agger nasi cell, below frontal sinus floor |
| Type 2 | Frontal cell type 2 | Supra agger cell (SAC) | A tier of two or more cells above the agger nasi cell, below frontal sinus floor |
| Type 3 | Frontal cell type 3 | Supra agger frontal cell (SAFC) | A single cell extending from agger nasi into the frontal sinus, but less than 50% of sinus height |
| Type 4 | Frontal cell type 4 | Supra agger frontal cell (SAFC) | A cell extending into the frontal sinus for more than 50% of sinus height (Wormald modification); originally Kuhn described it as an isolated cell entirely within the frontal sinus |
POSTERIOR CELLS (posterior to the frontal recess):
| Cell | IFAC Name | Description | Clinical Significance |
|---|---|---|---|
| Suprabullar cell | Suprabullar cell | Cell superior to the ethmoid bulla, not pneumatizing into frontal sinus | May contain anterior ethmoid artery |
| Frontal bulla cell | Supra bulla frontal cell (SBFC) | Cell superior to the bulla pneumatizing into the posterior frontal table (skull base); "crawls" along skull base | Pushes drainage pathway anteriorly |
| Supraorbital ethmoidal cell (SOE) | - | Pneumatizes superior to the orbital roof; posterior wall is the skull base | Can be mistaken for the frontal sinus; anterior ethmoid artery often in mesentery here |
MEDIAL CELLS:
| Cell | IFAC Name | Description |
|---|---|---|
| Intersinus cell / Frontal septal cell | Frontal septal cell | Pneumatizes the intersinus septum; drains into one frontal sinus, medial to the frontal ostium |
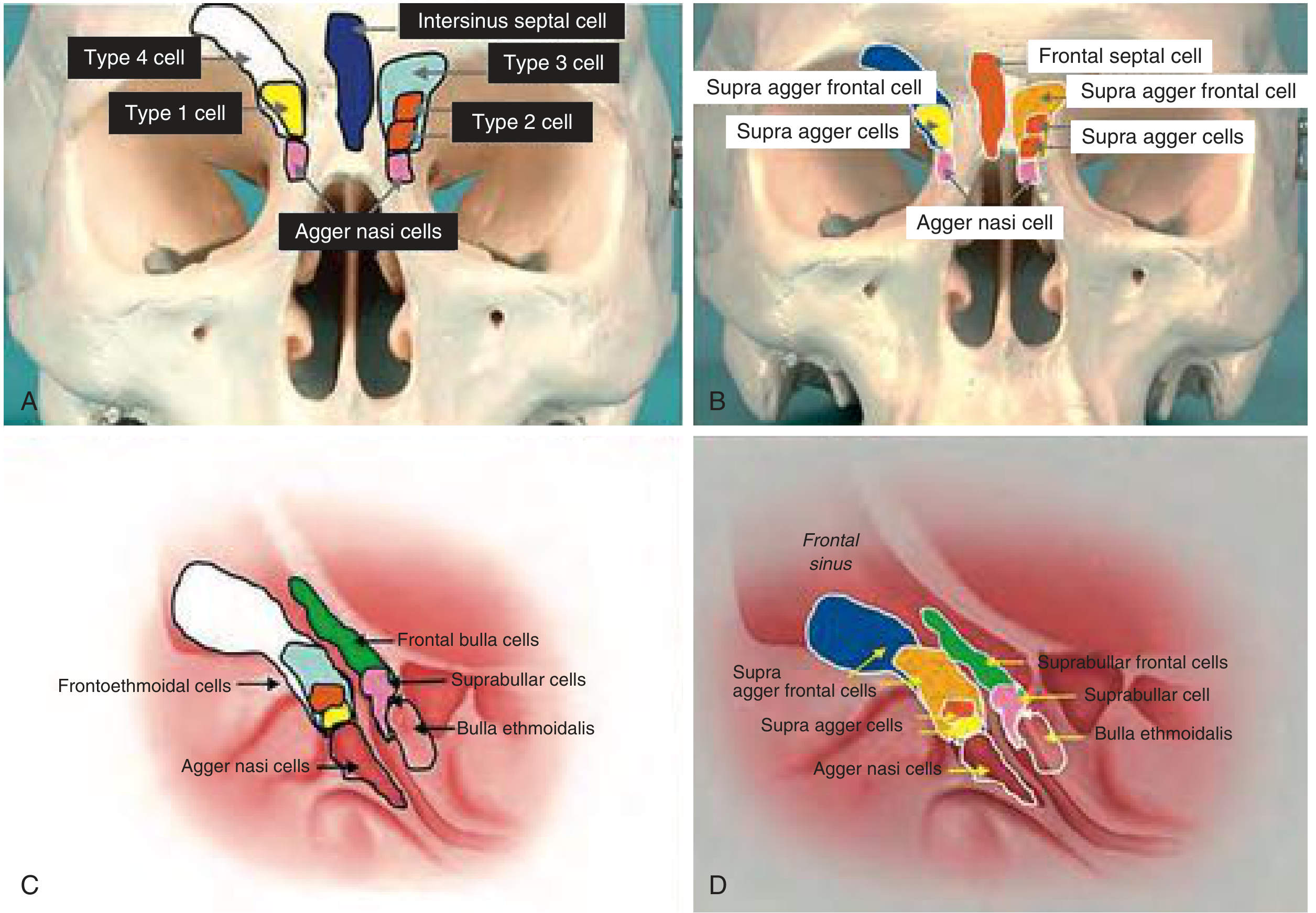
B. IFAC (International Frontal Sinus Anatomy Classification, 2016)
A simplified international consensus that classifies cells primarily by their location and relationship to the agger nasi and ethmoid bulla:
- Anterior cells: Supra agger cells (SAC) and Supra agger frontal cells (SAFC)
- Posterior cells: Supra bulla cells and Supra bulla frontal cells (SBFC)
- Medial cells: Frontal septal cell
Effect on drainage pathway:
- Anterior cells (frontal ethmoidal/Kuhn type cells) → push the drainage pathway posteriorly and/or medially
- Posterior cells (frontal bulla cells) → push the drainage pathway anteriorly
- Medial cells (intersinus septal cells) → push the drainage pathway laterally
(Cummings Otolaryngology, Box 44.1, p. 872; Scott-Brown's Table 99.1)
6. ONODI CELLS (SPHENOETHMOIDAL CELLS)
Definition
An Onodi cell (also called a sphenoethmoidal cell, SEC) is a posterior ethmoidal air cell that pneumatizes posteriorly over the superolateral aspect of the sphenoid sinus. The sphenoid sinus is pushed inferomedially and is usually smaller when an Onodi cell is present.
Key Facts
| Feature | Detail |
|---|---|
| Location | Posterior to and superior-lateral to the sphenoid sinus (sphenoid sinus is inferomedial) |
| Incidence | Approximately 30% of individuals |
| CT identification | Coronal CT: appears as a horizontal septation within the sphenoid sinus, posterior to the bony choanal arch |
| Optic nerve | The optic nerve can travel within or along the superolateral wall of the Onodi cell (rather than the sphenoid sinus) |
| ICA | The internal carotid artery can occasionally be exposed within the cell |
Clinical Significance
- Risk of optic nerve injury - The optic nerve projects along the superolateral wall of the Onodi cell, placing it at increased risk of iatrogenic injury during posterior ethmoid/sphenoid surgery
- Risk of mistaken identity - Onodi cells can be mistaken for the true sphenoid sinus, leading to incomplete surgery
- Pyramidal shape on CT - The most posterior ethmoidal cell has a pyramidal shape with the apex pointing posteriorly, laterally, and superiorly toward the optic nerve
- Surgical identification: When an Onodi cell is present, the sphenoid sinus ostium lies inferiorly and medially; applying the maxillary sinus roof/orbital floor landmark identifies the correct level of the sphenoid ostium
- When the Onodi cell is opened during surgery, the partition between it and the sphenoid sinus must be removed; the bony prominences of the optic and carotid canals should be clearly identified
(Cummings, p. 869; Scott-Brown's Box 87.16; KJ Lee's, p. 609)
Summary Table: Key Cell Relationships
| Cell | Position | Effect on Frontal Drainage | Danger |
|---|---|---|---|
| Agger nasi | Anterior-most ethmoid cell | Determines uncinate attachment, anterior boundary of frontal recess | None directly |
| Kuhn Type 1-2 (SAC) | Anterior to frontal recess, below sinus floor | Pushes drainage posteriorly | - |
| Kuhn Type 3-4 (SAFC) | Anterior, extends into sinus | May obstruct sinus; Type 4 may need trephination | Mistaken for sinus |
| Suprabullar cell | Posterior to frontal recess | - | Contains AEA |
| Frontal bulla / SBFC | Posterior, "crawls" along skull base | Pushes drainage anteriorly | AEA at risk |
| SOE cell | Posterior, above orbital roof | Can mimic frontal sinus | AEA in mesentery |
| Intersinus / Frontal septal | Medial | Pushes drainage laterally | - |
| Onodi cell (SEC) | Posterior ethmoid, lateral/superior to sphenoid | N/A (posterior ethmoid) | Optic nerve, ICA |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapter 44
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1, Chapters 87, 99
- KJ Lee's Essential Otolaryngology, Chapter on Rhinology
This is a shared conversation. Sign in to Orris to start your own chat.