Proper systemic anatomy of branchial apparatus in detail. I want to write in a note so give accordingly according to standard ent textbook.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the core content needed. Let me compile the comprehensive note.
BRANCHIAL APPARATUS - Systematic Anatomy
Source: Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Scott-Brown's Vol. 2
1. INTRODUCTION AND TERMINOLOGY
The term "branchial" is derived from the Greek word "bragchia" meaning gills. The branchial apparatus refers to the embryonic structures that give the neck region of the early human embryo the appearance of a series of slit-like grooves, resembling the gill apparatus of fish. This is an expression of the principle that "ontogeny recapitulates phylogeny" - in mammals, a phase is reached during early embryonic life that reflects earlier vertebrate (fish) forms.
2. EMBRYOLOGICAL DEVELOPMENT - TIMELINE
| Stage | Timing | Event |
|---|---|---|
| Pre-embryonic | 0-21 days | Blastocyst implantation |
| Embryonic | Day 21-56 | Rapid organogenesis - all major systems form |
| Foetal | Day 56 - birth | Growth, size, orientation changes - no new tissues |
- 4th week of gestation: Six branchial arches begin to emerge as neural crest cells migrate cranially into the mesenchyme surrounding the primitive foregut and pharynx
- 5th week: All six arches are apparent; the 5th arch obliterates soon after becoming apparent (thus functionally 5 arches: 1, 2, 3, 4, 6)
- 3rd to 8th week: Development of the branchial apparatus extends through this period
3. COMPONENTS OF THE BRANCHIAL APPARATUS
The branchial apparatus consists of three paired structures arranged between each arch:
A. Branchial Arches (Mesoderm + Neural Crest)
- Five to six parallel thickenings of mesenchyme that surround the pharynx
- Numbered 1 to 5 (or 6) from head to tail (cranial to caudal)
- Formed anterior to the 40-43 paired somites
- Each arch contains:
- A bar of cartilage (skeletal element)
- A group of muscles
- An associated artery (aortic arch artery)
- A cranial nerve (post-trematic nerve) - supplying structures of that arch and its derivatives
- A pretrematic nerve - from the arch below, supplying the endodermal (inner) surface of the arch above
B. Branchial Clefts / Grooves (Ectoderm - External)
- Ectodermal grooves on the external surface between adjacent arches
- Also called pharyngeal grooves
- In fish these break down to form gill clefts; in humans they normally regress
C. Pharyngeal Pouches (Endoderm - Internal)
- Endodermal outpouchings on the inner pharyngeal surface
- Each pouch lies opposite its corresponding cleft
- In early development, the endoderm and ectoderm come into contact momentarily; mesoderm then rapidly intervenes
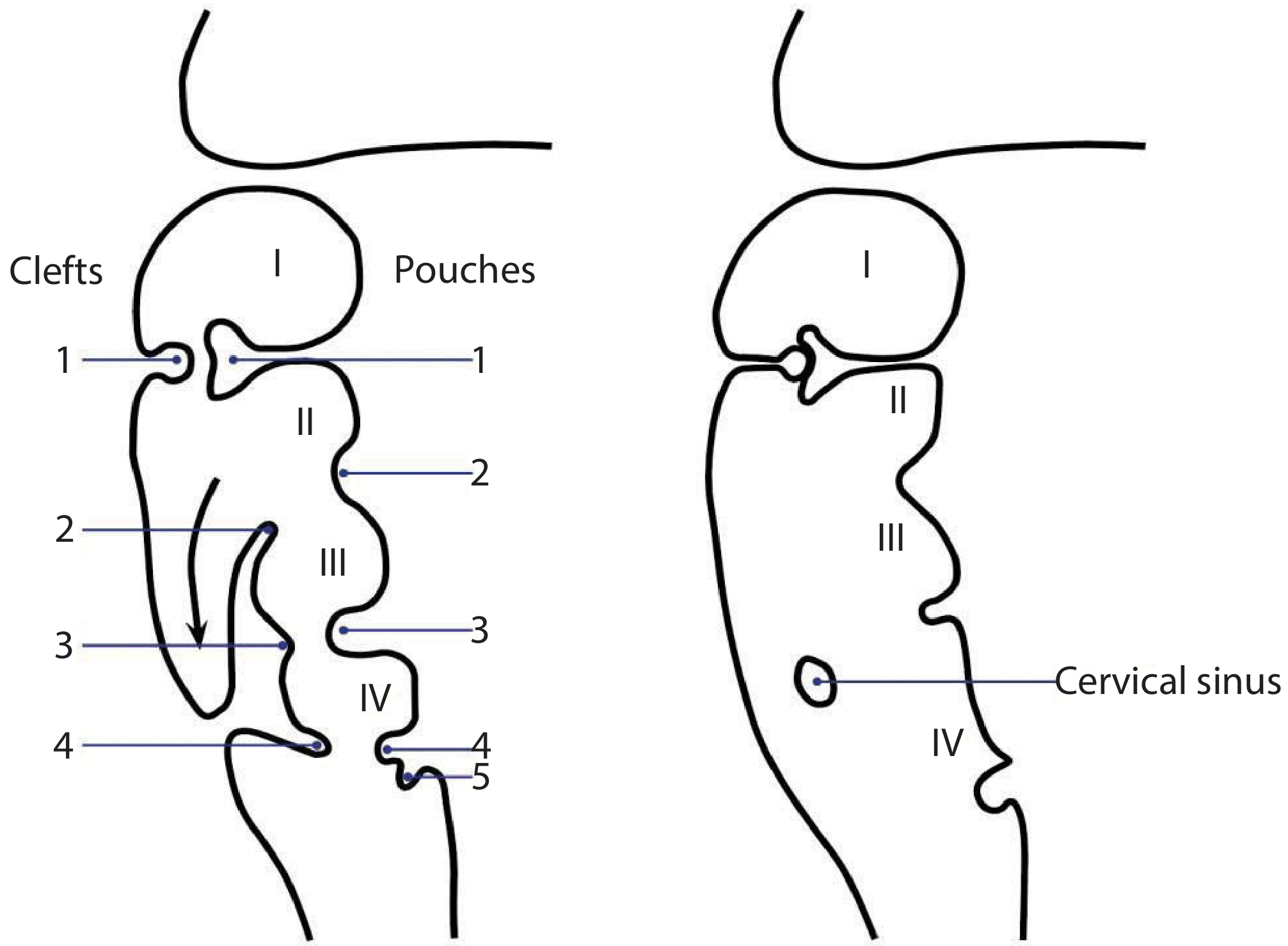
Figure: Branchial apparatus in utero. Left - early stage showing clefts (left, ectoderm) and pouches (right, endoderm) between arches I-IV. Right - later stage showing the cervical sinus formed by overgrowth of the 2nd arch.
4. NERVE SUPPLY TERMINOLOGY
Each branchial arch has two nerves:
| Nerve Type | Definition | Example |
|---|---|---|
| Post-trematic nerve | Cranial nerve of that arch; runs in the groove below (post = behind the cleft) | Arch 1 = V (Trigeminal), Arch 2 = VII (Facial), Arch 3 = IX (Glossopharyngeal) |
| Pre-trematic nerve | From the arch below; supplies endodermal surface of the arch above | Chorda tympani (from VII) → 1st arch; Jacobson's nerve / tympanic branch of IX → 2nd arch |
5. ARCH-BY-ARCH DERIVATIVES (Comprehensive Table)
| Arch | Name | Nerve | Cartilage/Bone | Muscles | Artery | Internal Pouch Derivative | External Cleft Derivative |
|---|---|---|---|---|---|---|---|
| 1 | Mandibular arch | V3 (Mandibular branch of Trigeminal) | Meckel's cartilage → Maxilla, Malleus, Incus, Anterior malleolar ligament, Sphenomandibular ligament | Mylohyoid, Anterior belly of digastric, Tensor tympani, Tensor veli palatini, Muscles of mastication | 1st aortic arch → Maxillary artery | Eustachian tube, Middle ear cleft, Medial surface of tympanic membrane | External auditory meatus, Lateral surface of tympanic membrane |
| 2 | Hyoid arch | VII (Facial nerve) | Reichert's cartilage → Stapes superstructure, Styloid process, Stylohyoid ligament, Lesser cornu + upper body of hyoid | Muscles of facial expression, Posterior belly of digastric, Platysma, Stapedius | 2nd aortic arch → Stapedial artery | Palatine tonsil (tonsillar fossa) | Grows caudally to cover 3rd and 4th clefts, forms cervical sinus of His |
| 3 | - | IX (Glossopharyngeal) | Greater cornu + lower body of hyoid | Stylopharyngeus, Superior & middle constrictors | 3rd aortic arch → Common & proximal internal carotid | Inferior parathyroid glands, Thymic duct | Obliterated |
| 4 | - | X (Vagus) - Superior laryngeal nerve | Thyroid lamina (cartilage) | Cricothyroid | 4th aortic arch → Arch of aorta (left), Subclavian (right) | Superior parathyroid glands | Obliterated |
| 5 | - | Obliterates early | - | - | - | - | - |
| 6 | - | X (Vagus) - Recurrent laryngeal nerve | Cricoid, Arytenoid cartilages | Inferior constrictor, Intrinsic muscles of larynx | 6th aortic arch → Ductus arteriosus (left), Disappears (right) | Ultimobranchial body → Parafollicular C-cells of thyroid | Obliterated |
6. IMPORTANT ARCH-SPECIFIC NOTES
First Arch (Mandibular)
- Meckel's cartilage: the ventral portion forms the ossicles (malleus and incus), while the dorsal portion contributes to the mandible
- The tensor tympani attaches to the malleus (1st arch origin), hence innervated by V (mandibular)
- The tensor veli palatini is the only soft palate muscle from arch 1 (all others are from arch 2/vagus)
- First pouch expands to form the Eustachian tube, middle ear, and mastoid antrum - this space is fully formed by 8 months' gestation
Second Arch (Hyoid / Reichert's)
- Stapedius muscle - attached to stapes (2nd arch), hence innervated by VII (facial)
- The 2nd arch grows caudally and comes to cover the 3rd and 4th clefts - forming the cervical sinus of His
- The chorda tympani (pretrematic nerve of arch 2) supplies taste to anterior 2/3 of tongue and secretomotor to submandibular gland - it runs through the middle layer of the tympanic membrane (the mesodermal layer between arch 1 and arch 2 ectoderm/endoderm)
- Second arch mesoderm almost covers the neck entirely and forms the platysma muscle
Pinna / Auricle
- Develops from cartilaginous hillocks (tubercles) surrounding the 1st pharyngeal groove
- Majority of auricle is derived from 2nd arch cartilages
- Tragus alone is the only contribution from the 1st arch
- Rudimentary pinna is formed by ~60 days
Tympanic Membrane (3 layers)
- Outer layer (ectoderm): 1st branchial cleft
- Inner layer (endoderm): 1st pharyngeal pouch
- Middle layer (mesoderm): intervening mesenchyme from 1st and 2nd arches
7. CERVICAL SINUS OF HIS
- Formed when the 2nd branchial arch grows caudally to meet the 5th arch
- The 2nd arch overgrows the 3rd and 4th clefts, burying them
- This creates a transient ectodermal-lined space called the cervical sinus
- Normally obliterates completely; failure to do so leads to branchial remnants
8. PHARYNGEAL POUCH DERIVATIVES (Summary)
| Pouch | Derivative |
|---|---|
| 1st | Eustachian tube, middle ear (tympanic cavity), mastoid antrum, medial surface of tympanic membrane |
| 2nd | Palatine tonsil, tonsillar fossa |
| 3rd (dorsal) | Inferior parathyroid glands |
| 3rd (ventral) | Thymus |
| 4th (dorsal) | Superior parathyroid glands |
| 4th/6th (ventral) | Ultimobranchial body → Parafollicular (C) cells of thyroid |
9. AORTIC ARCH ARTERIES - SUMMARY
| Arch Artery | Adult Derivative |
|---|---|
| 1st | Maxillary artery (part) |
| 2nd | Stapedial artery (regresses in adults) |
| 3rd | Common carotid, proximal internal carotid |
| 4th (Left) | Arch of aorta |
| 4th (Right) | Proximal subclavian artery |
| 5th | Obliterates |
| 6th (Left) | Ductus arteriosus / ligamentum arteriosum |
| 6th (Right) | Disappears |
10. CONGENITAL BRANCHIAL ANOMALIES
Failure of normal obliteration of the branchial apparatus results in:
- Cyst - epithelium-lined cavity with no opening
- Sinus - blind-ended tract opening onto one epithelial surface (external or internal)
- Fistula - a complete tract running from one epithelial surface to another (ecto-endodermal junction breakdown)
Branchial Anomalies by Cleft Origin
| Origin | Frequency | External Opening | Internal Opening | Key Relationship |
|---|---|---|---|---|
| 1st cleft | ~5% | Anterior/inferior to tragus (Type I); Posterior to angle of mandible (Type II) | External ear canal or conchal bowl | Facial nerve (can run deep or superficial) |
| 2nd cleft | ~90% | Anterior border of SCM (lower 1/3) | Tonsillar fossa | Passes between ICA and ECA, deep to posterior belly of digastric |
| 3rd cleft | ~4% | Anterior border of SCM (lower 1/3) | Pyriform fossa | Passes posterior to ICA |
| 4th cleft | <1% | Lower anterior border of SCM | Pyriform fossa / hypopharynx | Passes posterior to subclavian artery (right) or aortic arch (left) |
Work Classification (1st Cleft Anomalies - 1972)
- Type I: Duplication of membranous external auditory canal (ectoderm only) - superficial to facial nerve
- Type II: Contains both ectoderm and mesoderm (skin and cartilage) - inconstant relationship with facial nerve
Aetiology of Branchial Cysts - 4 Theories
- Branchial apparatus theory - remnants of pharyngeal pouches or branchial clefts; cysts should be present at birth (but peak is 2nd-3rd decade - contradicts this)
- Cervical sinus theory - remnants of the cervical sinus of His (2nd arch growing down to meet 5th arch)
- Thymopharyngeal duct theory - remnants of the connection between thymus and 3rd branchial pouch
- Inclusion theory (most widely accepted) - epithelial inclusions within lymph nodes; supported by lymphoid tissue in cyst walls and late peak presentation
Histology of Branchial Cysts
- Lined by stratified squamous epithelium (90%)
- 10% may have respiratory epithelium
- 80% have lymphoid tissue in the outer wall
- Contents: straw-coloured fluid containing cholesterol crystals
11. KEY CLINICAL POINTS
- Structures innervated by cranial nerves in the neck are derived from the branchial apparatus
- The 5th arch has no clinical significance as it obliterates early
- Branchial anomalies account for up to 19% of all paediatric cervical masses
- Peak incidence of branchial cysts is in the 3rd decade (2nd-3rd decade)
- 2nd branchial cleft anomalies are the most common (~90-95% of all branchial cleft anomalies)
- Treatment of 1st and 2nd branchial fistulae: complete surgical excision of tract with CN VII monitoring
- 3rd and 4th branchial cleft anomalies may be managed with endoscopic ablation of the internal (pyriform fossa) opening
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol. 1 and Vol. 2) - Developmental Anatomy, Branchial Cysts, Development of the Human Ear
- K.J. Lee's Essential Otolaryngology - Branchial Arch Syndromes
This is a shared conversation. Sign in to Orris to start your own chat.