Portal hypertension.causes,clinical features and management.TIPSS
Reading File
Finding Sources
Searching PubMed
"portal hypertension" AND "TIPS" management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
portal hypertension pathophysiology diagram TIPS transjugular intrahepatic portosystemic shunt
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Portal Hypertension
Definition
Portal hypertension is defined as an elevation in portal venous pressure above the normal range (3–5 mmHg). Clinically significant portal hypertension is present when the Hepatic Venous Pressure Gradient (HVPG) exceeds 10 mmHg; variceal bleeding risk rises sharply when HVPG exceeds 12 mmHg.
HVPG = Wedged Hepatic Venous Pressure (WHVP) − Free Hepatic Venous Pressure (FHVP), measured via balloon catheter passed through the jugular vein into the hepatic vein.
Causes / Classification
Causes are classified by the site of increased resistance to portal blood flow:
1. Prehepatic (Extrahepatic)
| Mechanism | Examples |
|---|---|
| Portal vein obstruction | Portal vein thrombosis, congenital atresia |
| Splenic vein obstruction | Splenic vein thrombosis (sinistral/left-sided portal HTN) |
| Increased inflow | Splenic arteriovenous fistula, massive splenomegaly |
2. Intrahepatic
Presinusoidal:
- Schistosomiasis (S. mansoni, S. japonicum) — eggs deposit in presinusoidal portal venules → granulomatous fibrosis; common in sub-Saharan Africa, Middle East, Asia
- Congenital hepatic fibrosis
- Nodular regenerative hyperplasia
- Idiopathic portal hypertension / hepatoportal sclerosis (more common in India, Japan)
- Sarcoidosis, myeloproliferative disorders, graft-versus-host disease
- Primary biliary cholangitis (early stage — presinusoidal; cirrhotic stage — sinusoidal)
Sinusoidal (most common group):
- Cirrhosis (all causes) — the leading cause worldwide
- Alcohol-associated liver disease
- Viral hepatitis (HBV, HCV)
- NAFLD/MASLD
- Primary biliary cholangitis (late stage)
- Autoimmune hepatitis
- Primary sclerosing cholangitis, haemochromatosis
- Infiltrative liver diseases
Postsinusoidal (intrahepatic):
- Sinusoidal obstruction syndrome (hepatic veno-occlusive disease)
3. Posthepatic (Extrahepatic)
- Budd-Chiari syndrome (hepatic vein obstruction)
- Inferior vena cava web or thrombosis
- Congestive heart failure / constrictive pericarditis → cardiac cirrhosis
- Severe tricuspid regurgitation
Most common cause in the United States and Europe: Cirrhosis (intrahepatic sinusoidal).
Pathophysiology
The central mechanism is a dual insult:
- Increased intrahepatic resistance — structural (fibrosis, nodule formation distorting sinusoidal architecture) + dynamic (hepatic stellate cell contraction, reduced intrahepatic nitric oxide)
- Increased portal blood flow — splanchnic arteriolar vasodilation (mediated by nitric oxide, prostacyclin, glucagon) → hyperdynamic circulation → further raises portal pressure
This leads to:
- Portosystemic collateral formation (varices)
- Splanchnic vasodilation → activation of RAAS + SNS → renal sodium retention → ascites
- Systemic inflammation via bacterial translocation (PAMPs/DAMPs)
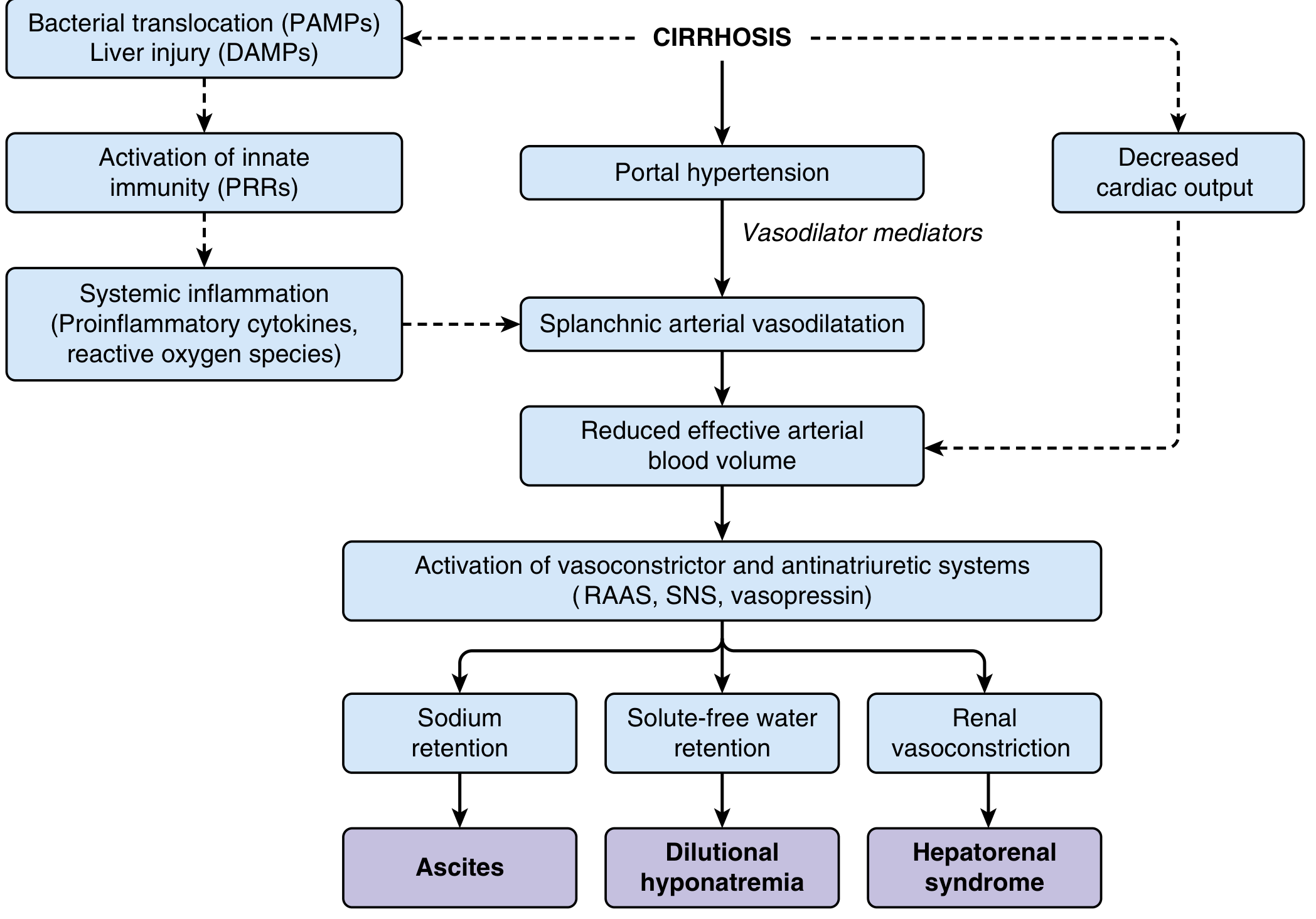
Pathophysiology of ascites and renal dysfunction in advanced cirrhosis — Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Clinical Features
Consequences of Portosystemic Collateral Formation
- Gastroesophageal varices — ~30% of compensated and ~60% of decompensated cirrhotics; supplied mainly by the left gastric (coronary) vein
- Anorectal varices — present in ~45% of cirrhotics (distinguish from haemorrhoids, which do not communicate with portal system)
- Caput medusae — recanalization and dilation of the umbilical vein → visible periumbilical collaterals
- Splenorenal and mesocaval shunts — spontaneous but ineffective at decompression
Splenomegaly & Hypersplenism
- Enlarged, tortuous splenic vessels
- Functional hypersplenism: leukopenia, thrombocytopenia, anaemia (pancytopenia)
Ascites
- Combination of portal hypertension + hepatocyte dysfunction
- Sodium retention (RAAS/SNS activation) drives fluid accumulation
Systemic Complications (Full Spectrum)
| System | Complications |
|---|---|
| GI | Variceal bleeding (oesophageal, gastric), portal hypertensive gastropathy |
| Renal | Hepatorenal syndrome, dilutional hyponatraemia |
| Pulmonary | Hepatopulmonary syndrome, portopulmonary hypertension, hepatic hydrothorax |
| Cardiac | Cirrhotic cardiomyopathy |
| Neurological | Hepatic encephalopathy |
| Haematological | Anaemia, hypersplenism, impaired coagulation, hypercoagulability |
| Infections | SBP, bacteraemia, UTI, pneumonia |
| Malignancy | HCC, cholangiocarcinoma |
Management
A. Primary Prevention of Variceal Bleeding (Prophylaxis)
Pharmacological:
- Non-selective β-blockers (propranolol, nadolol, carvedilol) — reduce portal pressure; meta-analyses show ~45% reduction in index variceal bleed and ~50% decrease in bleeding mortality
- ~20% of patients do not respond; ~20% cannot tolerate
Endoscopic:
- Variceal band ligation (VBL) — recommended for medium-to-large varices; performed every 1–2 weeks until obliteration, then EGD at 1–3 months, then every 6 months surveillance
B. Acute Variceal Haemorrhage
- Resuscitation — ICU admission; target Hb ~8 g/dL (avoid over-transfusion — worsens portal pressure and rebleeding); cautious use of FFP and platelets for severe coagulopathy
- Antibiotic prophylaxis — ceftriaxone 1 g/day IV; reduces bacterial infection risk and improves survival (SBP accounts for ~50% of infections in this setting)
- Vasoactive drugs (initiate immediately on clinical suspicion):
- Octreotide (somatostatin analogue) — preferred agent; can be administered for ≥5 days; reduces splanchnic blood flow
- Terlipressin (where available) — most potent vasoconstrictor
- Note: vasopressin limited by systemic side effects (hypertension, MI, arrhythmias, ischaemia)
- Endoscopy (EGD) — as soon as feasible; VBL is first-line; combination of pharmacologic + endoscopic therapy improves 5-day haemostasis
- Balloon tamponade (Sengstaken-Blakemore tube) — for refractory bleeding when endoscopy fails; controls bleeding in up to 90%; limited to ≤36 hours due to risk of aspiration, airway obstruction, and oesophageal perforation
- TIPSS — for refractory or recurrent bleeding not controlled by endoscopic/medical therapy (see below)
C. Secondary Prevention (Post-Bleed)
- If left untreated, 70% of patients rebleed within 2 years
- Combination of non-selective β-blocker + repeated VBL is standard
- TIPSS — superior to endoscopic/pharmacologic therapy for secondary prevention; rebleeding occurs in only 5–15% post-TIPS (usually due to stent occlusion)
D. Ascites Management
- Low-sodium diet + diuretics (spironolactone ± furosemide)
- Large-volume paracentesis (LVP) with albumin infusion for refractory ascites
- TIPSS — for refractory ascites (see below)
TIPSS (Transjugular Intrahepatic Portosystemic Shunt/Stent)
What It Is
TIPSS is a percutaneous, non-surgical procedure performed by an interventional radiologist that creates an artificial side-to-side portocaval shunt inside the liver parenchyma — connecting a portal vein branch to a hepatic vein via a covered metal stent.
First introduced in 1989 by Richter and colleagues.
Technique
- Access via the right internal jugular vein under fluoroscopic guidance
- Guidewire and sheath advanced through SVC → IVC → hepatic vein
- Contrast injected to locate the portal vein; needle advanced through liver parenchyma to create a transhepatic tract
- Angioplasty balloon dilates the tract
- PTFE (polytetrafluoroethylene)-covered stent deployed — now the current standard (higher patency vs. uncovered stents)
The procedure creates a direct portal-to-systemic communication, effectively reducing portal venous pressure.
Goal PPG (portosystemic pressure gradient): <12 mmHg to prevent variceal haemorrhage; <10 mmHg when the indication is ascites.

Pre-TIPS (Panel A): Dilated left gastric vein with large gastroesophageal varix. Post-TIPS (Panel B): Successful shunt — contrast no longer fills varices
Indications
| Primary Indications | Other Indications |
|---|---|
| Refractory ascites | Portal hypertensive gastropathy |
| Acute variceal haemorrhage (failure of endoscopic/pharmacologic therapy) | Hepatic hydrothorax |
| Prevention of recurrent variceal haemorrhage | Budd-Chiari syndrome |
| Hepatorenal syndrome (selected cases) | |
| Hepatopulmonary syndrome |
Contraindications
Absolute:
- Congestive heart failure
- Severe tricuspid regurgitation
- Severe pulmonary hypertension (mean pulmonary pressure >45 mmHg)
- Uncontrolled systemic sepsis
- Severe pre-existing hepatic encephalopathy
- Multiple hepatic cysts / unrelieved biliary obstruction
- Primary prevention of variceal bleeding (not indicated in asymptomatic patients)
Relative:
- MELD score ≥18 (significantly higher post-procedure mortality; some centres use ≥25 as the threshold)
- Serum bilirubin >3 mg/dL
- Serum sodium ≤130 mEq/L
- Portal or hepatic vein thrombosis
- Centrally located hepatic mass
- Moderate pulmonary hypertension
- Pre-existing hepatic encephalopathy (relative — predictor of mortality)
Outcomes & Patency
- 1-year patency: ~93%, 3-year patency: ~75% with PTFE-covered stents
- Rebleeding in 5–15% post-TIPS; most due to stent stenosis or thrombosis
- Ascites recurrence: 42% TIPS vs. 89% paracentesis
- Transplant-free survival at 6/12/24/36 months with TIPS: 75%/63%/49%/38% vs. 65%/53%/35%/29% with paracentesis
- Earlier TIPS placement (before waiting for transplant) associated with improved 1-year transplant survival (93% vs. 53%)
Complications
| Complication | Detail |
|---|---|
| Hepatic encephalopathy | Most significant long-term complication; 20–30% risk due to portosystemic shunting; manage with lactulose + rifaximin |
| Shunt dysfunction (stenosis/thrombosis) | ~1/3 of patients within 1 year; significantly reduced with PTFE-covered stents |
| Liver failure | Diversion of portal (hepatotrophic) blood flow away from hepatocytes |
| Right heart failure | Volume overload from splanchnic blood redirected to systemic circulation |
| Intraperitoneal haemorrhage | Capsular perforation in up to 33%; clinically significant in 1–2% |
| Abdominal wall hernia incarceration | After ascites resolution post-TIPS |
| Procedure-related mortality | 0.6–4.3% (varies with institutional experience); fatal causes: hepatic artery/portal vein laceration, right heart failure |
TIPSS vs. Surgical Shunts
- TIPS can be completely removed with the explanted liver at transplantation — advantage over surgical shunts, which require ligation/revision intraoperatively
- In noncirrhotic portal hypertension or well-compensated cirrhosis where TIPS is not feasible, surgical portosystemic shunts remain effective (>90% success in controlling variceal bleeding)
- Parallel TIPS (double TIPS) has been described for TIPS occlusion or Budd-Chiari syndrome refractory to single shunting
Stent Size
- Smaller diameter stents (8–10 mm) are associated with lower incidence of hepatic encephalopathy post-TIPSS without reducing ascites clearance — a useful approach in patients at high encephalopathy risk
Summary: TIPSS at a Glance
| Feature | Detail |
|---|---|
| Route | Right internal jugular vein → hepatic vein → portal vein |
| Stent | PTFE-covered metal stent (current standard) |
| Goal | PPG <12 mmHg (bleeding); <10 mmHg (ascites) |
| Main indications | Refractory ascites, variceal haemorrhage, recurrence prevention |
| Key absolute contraindications | CCF, severe TR, severe PH, uncontrolled sepsis, severe HE |
| Key relative contraindications | MELD ≥18, bilirubin >3 mg/dL, portal/hepatic vein thrombosis |
| Main long-term complication | Hepatic encephalopathy (20–30%) |
| 1-year patency | ~93% (PTFE stent) |
Sources: Schwartz's Principles of Surgery (11e), Current Surgical Therapy (14e), Sleisenger & Fordtran's GI and Liver Disease, Yamada's Textbook of Gastroenterology (7e), Comprehensive Clinical Nephrology (7e)
Recent evidence note: A 2024 systematic review (PMID 38935315) confirmed TIPS efficacy for ectopic variceal bleeding. A 2024 meta-analysis (PMID 39126599) assessed TIPS safety in hepatocellular carcinoma. A 2025 systematic review (PMID 40741106) identified cardiovascular predictors of cardiac decompensation post-TIPS — cardiovascular risk stratification before TIPS is increasingly recognised as important.
This is a shared conversation. Sign in to Orris to start your own chat.