Can you explain pharmacokinetics to me
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive content from Goodman & Gilman's. I also have the key ADME diagram. Let me now compile the full, well-structured answer.
Pharmacokinetics: What the Body Does to a Drug
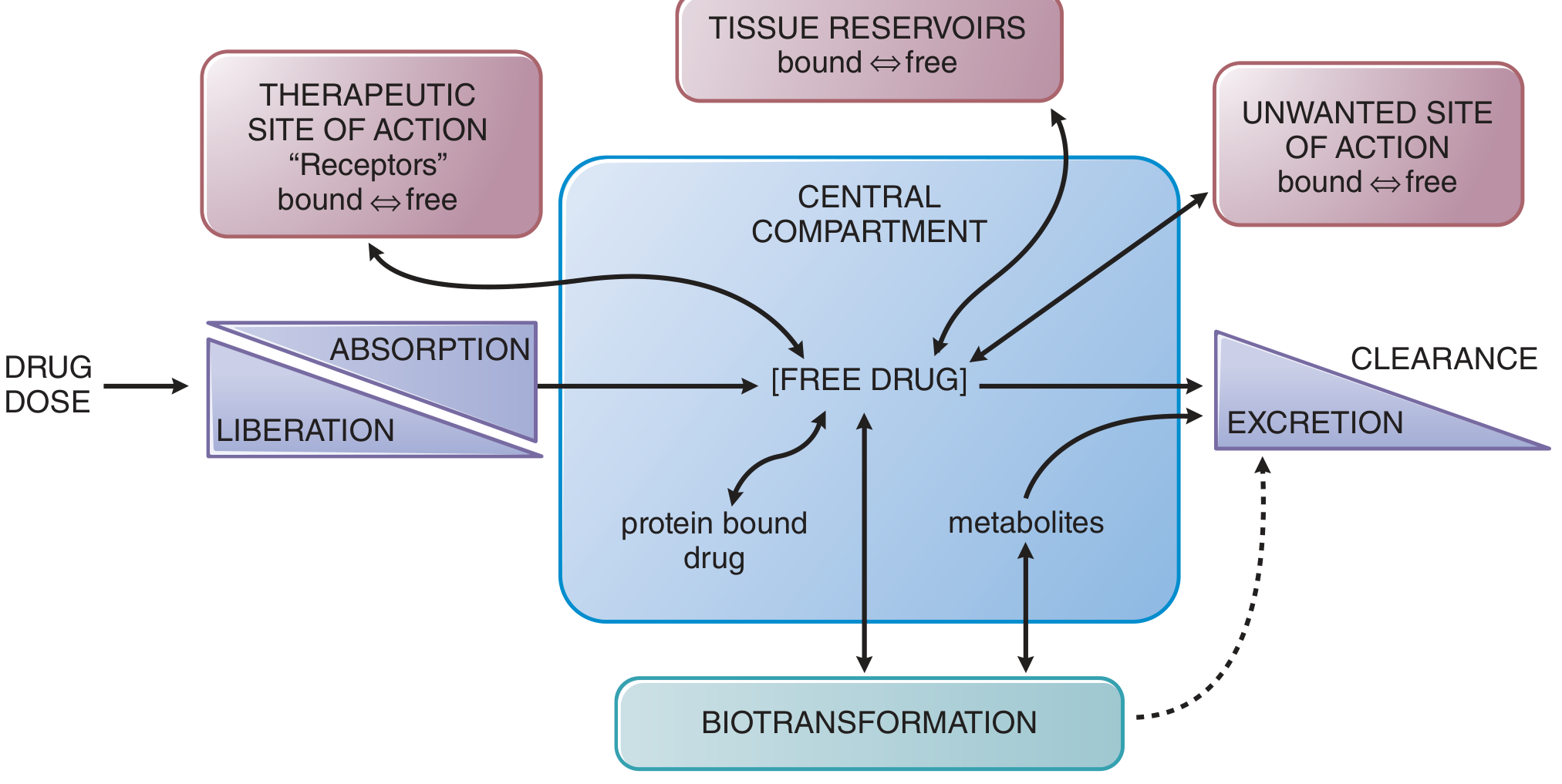
Pharmacokinetics (PK) describes the movement and fate of a drug in the body from the moment of administration to final elimination. As stated in Goodman & Gilman's The Pharmacological Basis of Therapeutics:
"ADME - the absorption, distribution, metabolism, and elimination of drugs - are the processes of pharmacokinetics. Understanding these processes and their interplay increases the probability of therapeutic success and reduces the occurrence of adverse drug events and drug-drug interactions."
Here is a visual overview of how these processes interact:
1. Absorption
Absorption is the process by which a drug moves from the site of administration into the systemic circulation.
Key factors affecting absorption:
- Route of administration - IV bypasses absorption entirely (100% bioavailability by definition). Oral, sublingual, intramuscular, subcutaneous, and topical routes all involve absorption steps.
- Molecular properties - Lipid solubility, molecular size, and degree of ionization all determine how readily a drug crosses cell membranes. Lipophilic, non-ionized drugs cross membranes more easily via passive diffusion.
- pH and ionization (Henderson-Hasselbalch) - Weak acids are better absorbed in acidic environments (stomach), weak bases in alkaline environments (small intestine). Ion trapping occurs when a drug is "trapped" on the more ionized side of a membrane.
- Transport proteins - Active transporters (e.g., P-glycoprotein, OATPs) can facilitate or limit absorption.
Bioavailability (F)
Bioavailability is the fraction of an administered dose that reaches the systemic circulation unchanged. It is reduced by:
- Incomplete absorption from the GI tract
- First-pass effect - After oral ingestion, drugs enter the portal vein and pass directly to the liver before reaching systemic circulation. Hepatic metabolism there can significantly reduce the available drug. Some drugs (e.g., lidocaine, naloxone) are so extensively metabolized on first pass that they cannot be given orally at all. Others like propranolol are dosed orally by accounting for the large first-pass effect.
2. Distribution
Once in the circulation, a drug distributes throughout the body into tissues.
Key factors:
- Blood flow - Highly perfused organs (heart, brain, liver, kidney) equilibrate rapidly. Slowly perfused tissues (muscle, fat, bone) equilibrate slowly.
- Plasma protein binding - Drugs bind reversibly to albumin or alpha-1 acid glycoprotein. Only free (unbound) drug is pharmacologically active, crosses membranes, and is eliminated.
- Lipophilicity - Lipophilic drugs penetrate membranes readily, including the blood-brain barrier (BBB).
Volume of Distribution (V_d)
V_d is a theoretical volume that relates the amount of drug in the body to the plasma concentration:
V_d = Amount of drug in body / Plasma concentration
- A small V_d (close to plasma volume, ~3-5 L) means the drug stays in blood - usually because it is highly protein-bound and/or hydrophilic.
- A large V_d (hundreds of liters) means the drug is extensively sequestered in tissues (e.g., chloroquine V_d ~ 200-800 L/kg).
3. Metabolism (Biotransformation)
Metabolism converts drugs into metabolites, usually making them more water-soluble for excretion. It occurs primarily in the liver (and to lesser extent in the gut wall, lungs, and kidneys).
Two phases:
| Phase | Reaction | Purpose | Example |
|---|---|---|---|
| Phase I | Oxidation, reduction, hydrolysis | Add or expose a functional group (-OH, -NH2) | Cytochrome P450 (CYP) enzymes |
| Phase II | Conjugation | Attach a large polar group (glucuronide, sulfate) to increase water solubility | UGTs, sulfotransferases |
Cytochrome P450 (CYP) enzymes - The CYP3A4 isoform metabolizes ~50% of all drugs. CYP2D6, CYP2C9, and CYP2C19 are also important. Drug-drug interactions often arise from one drug inhibiting or inducing another's CYP metabolism.
Prodrugs - Some drugs are administered in an inactive form and must be metabolized to the active compound (e.g., codeine → morphine via CYP2D6).
4. Excretion
The primary routes of elimination are:
- Renal (most common) - Glomerular filtration, active tubular secretion, and passive tubular reabsorption all affect how much drug exits in urine. Altering urine pH affects excretion: alkaline urine promotes excretion of weak acids (e.g., aspirin); acidic urine promotes excretion of weak bases.
- Biliary/Fecal - Drugs and metabolites secreted into bile can be excreted in feces or reabsorbed in the intestine (enterohepatic recirculation).
- Other routes - Lungs (volatile anesthetics), breast milk, sweat, saliva.
Key PK Parameters
Clearance (CL)
CL is the volume of plasma from which drug is completely removed per unit time:
CL = Rate of elimination / Plasma concentration
Total clearance is the sum of all organ clearances:
CL_total = CL_renal + CL_hepatic + CL_other
For a single dose: CL = Dose / AUC (where AUC = area under the concentration-time curve)
Half-Life (t₁/₂)
The time for plasma concentration to fall by 50%:
t₁/₂ = 0.693 × V_d / CL
This equation reveals that half-life is not an independent parameter - it depends on both V_d and CL. Importantly:
- ~4-5 half-lives are needed to reach steady state during repeated dosing
- ~4-5 half-lives are needed for a drug to be ~97% eliminated after stopping
Steady State
With repeated dosing, drug accumulates until the rate in = rate out. The average steady-state concentration is:
C_ss = (F × Dosing rate) / CL
Nonlinear Pharmacokinetics
Most drugs follow first-order kinetics (a constant fraction eliminated per unit time). Some drugs saturate their metabolic enzymes at therapeutic concentrations and switch to zero-order kinetics (a constant amount eliminated per unit time, regardless of concentration). This is clinically important for drugs like phenytoin, alcohol, and aspirin at high doses, where small dose increases can cause disproportionately large rises in plasma concentration.
Quick Reference Summary
| Parameter | Definition | Clinical relevance |
|---|---|---|
| F (Bioavailability) | Fraction of dose reaching systemic circulation | Determines oral dose needed |
| V_d | Apparent volume into which drug distributes | Affects loading dose; high V_d = hard to dialyze out |
| CL | Volume of plasma cleared per unit time | Determines maintenance dose |
| t₁/₂ | Time for 50% reduction in plasma concentration | Determines dosing interval & time to steady state |
| AUC | Total drug exposure over time | Reflects overall bioavailability |
| C_max / T_max | Peak concentration / Time to peak | Relates to efficacy and toxicity thresholds |
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics, Katzung's Basic and Clinical Pharmacology 16th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.