skull x ray positioning
Reading File
Finding Sources
Searching the Web
skull x-ray positioning projections radiography technique
Finding Sources
Reading Web Page
https://ce4rt.com/positioning/radiographic-positioning-of-th…
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is a complete, well-organized guide to skull X-ray positioning.
Skull X-Ray Positioning
Anatomical Reference Lines (Essential)
Before any projection, you must understand the key positioning lines:
| Line | Landmarks |
|---|---|
| Midsagittal Plane (MSP) | Divides skull into equal left and right halves; must always be centered and perpendicular to IR (unless lateral) |
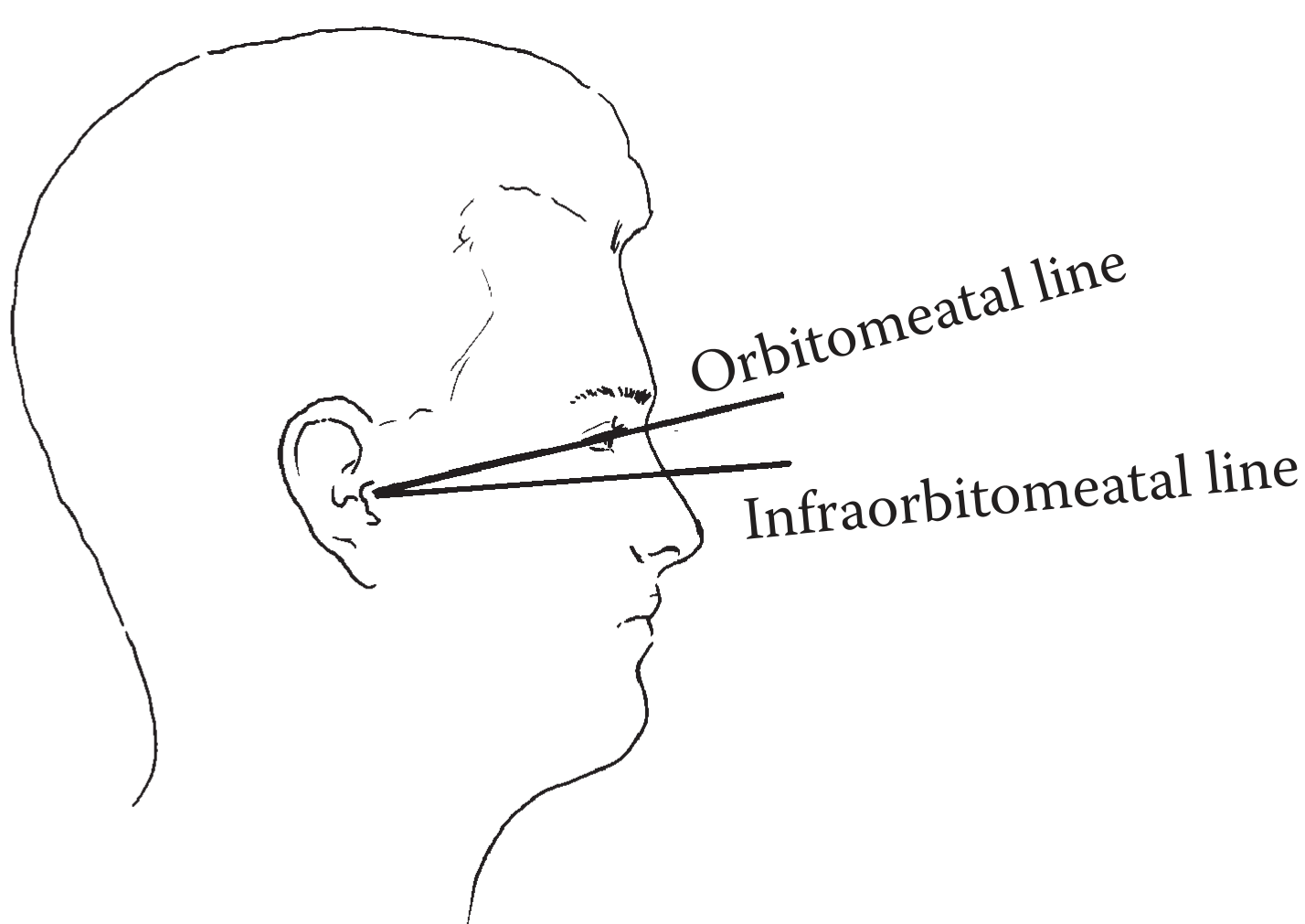
| Orbitomeatal Line (OML) | Outer canthus of eye to external auditory meatus (EAM) |
| Infraorbitomeatal Line (IOML) | Inferior orbital margin to EAM; ~7° lower than OML |
| Interpupillary Line (IPL) | Between the two pupils; perpendicular to IR in frontal views |
1. PA Occipito-Frontal (Occipitofrontal / 0°)
| Parameter | Detail |
|---|---|
| Position | Prone (or erect); forehead and nose rest on the IR |
| MSP | Centered and perpendicular to IR |
| OML | Perpendicular to IR |
| CR | Perpendicular (0°), directed to nasion |
| IR size | 24 × 30 cm (10 × 12 in.) |
| Centering | Nasion |
Structures demonstrated: Frontal bone, frontal and anterior ethmoid sinuses, crista galli, internal auditory canals, greater and lesser wings of sphenoid, petrous ridges projected in the lower third of the orbits.
Note: Contraindicated in unconscious patients or suspected facial fractures.
2. PA Axial - Caldwell Method (15° Caudal)
| Parameter | Detail |
|---|---|
| Position | Prone or erect; forehead and nose on IR |
| MSP | Perpendicular to IR, centered to midline |
| OML | Perpendicular to IR |
| CR | 15° caudal, directed to exit at nasion |
| Centering | Nasion |
Structures demonstrated: Frontal and ethmoid sinuses, superior orbital margins, greater and lesser sphenoid wings, superior orbital fissures, petrous ridges projected in the lower third of orbits, crista galli. Best view for fractures with medial/lateral displacement.
3. AP Projection (Reverse Caldwell)
| Parameter | Detail |
|---|---|
| Position | Supine; back of head on IR |
| MSP | Centered and perpendicular to IR |
| OML | Perpendicular to IR (may use thin sponge under head) |
| CR | Perpendicular to midpoint of cassette |
| IR size | 24 × 30 cm lengthwise |
| Upper border | ~1 inch (2.5 cm) above vertex |
Structures demonstrated: AP view of all major cranial bones. Used when patient cannot be prone.
(Source: Brogdon's Forensic Radiology)
4. Lateral Projection
| Parameter | Detail |
|---|---|
| Position | Lateral recumbent (or erect); affected side closest to IR |
| MSP | Parallel to IR |
| IPL | Perpendicular to IR |
| IOML | Parallel to the long axis of the IR |
| CR | Perpendicular to IR, directed 2.5 cm (1 in.) superior to EAM |
| IR size | 24 × 30 cm, placed vertically |
Structures demonstrated: Lateral view of cranial bones, sella turcica, anterior/posterior clinoid processes, dorsum sellae, sphenoid sinuses, vertex.
Cross-table lateral (trauma): IR placed vertically against the side of the skull; horizontal beam directed perpendicular to IR. Upper cassette border 1.9-2.5 cm above vertex. Used when the patient cannot be moved.
5. AP Axial - Towne's Method (30° or 37° Caudal)

| Parameter | Detail |
|---|---|
| Position | Supine; back of skull on IR |
| MSP | Perpendicular to IR, centered |
| OML | Perpendicular to IR |
| CR | 30° caudal (if OML is perpendicular) OR 37° caudal (if IOML is used instead) |
| Entry point | CR enters 1/2 inch (1.3 cm) above eyebrows |
| Exit point | Exits at the mastoid process area |
| IR centering | Centered at CR exit point |
Structures demonstrated: Occipital bone, foramen magnum, dorsum sellae, petrous pyramids, posterior clinoid processes. Excellent for occipital fractures. (Brogdon's Forensic Radiology)
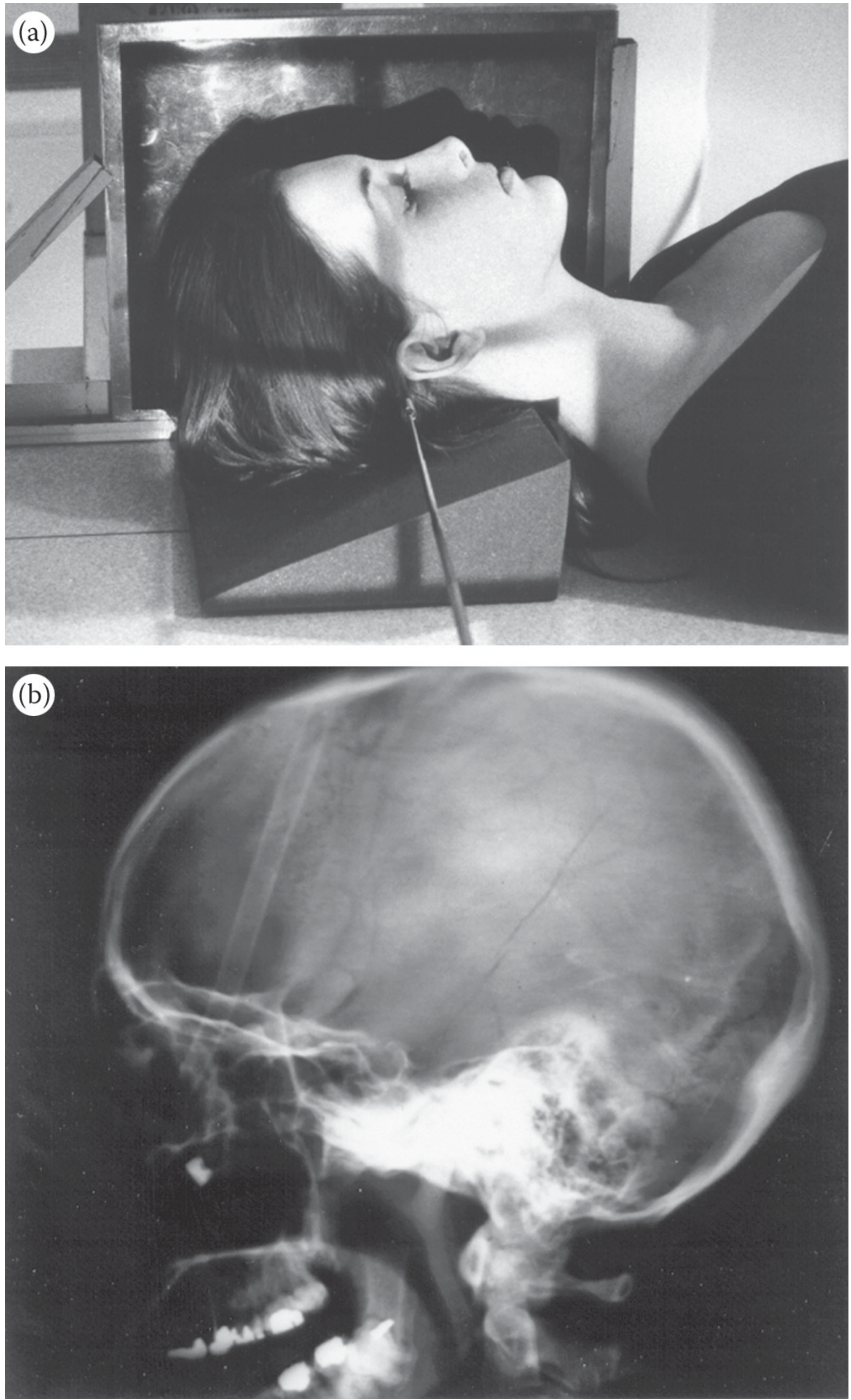
6. Submentovertex (SMV) - Base View
| Parameter | Detail |
|---|---|
| Position | Supine (or seated); neck hyperextended |
| IOML | As parallel as possible to the IR |
| MSP | Perpendicular to IR |
| CR | Perpendicular to IOML, directed through sella turcica |
Structures demonstrated: Cranial base, foramen ovale/spinosum/lacerum, zygomatic arches, mandibular condyles, sphenoid sinuses, petrous pyramids, carotid canals.
Contraindicated if cervical spine injury is suspected.
7. Verticosubmental (VSM) - Schüller Method
An alternative to SMV when the patient cannot hyperextend the neck:
- Position: Prone
- MSP: Centered to grid
- CR: Perpendicular to IOML
Key Positioning Tips
- Remove all artifacts before imaging: dentures, hair grips, ear clips, hearing aids, and glasses.
- Grid cassette is standard for skull work.
- Check the MSP is not rotated - in PA/AP views, the orbital plates, lesser wings, and petrous ridges should be symmetric.
- Rotation check on lateral: orbital roofs and mandibular rami should be perfectly superimposed.
- For Towne's, the dorsum sellae should project into the foramen magnum if CR angulation is correct.
Source: Brogdon's Forensic Radiology (medical library); CE4RT Skull Positioning Reference
This is a shared conversation. Sign in to Orris to start your own chat.