Bone marrow injections in Orthopedics explain in detail methodology indications usage and contraindications advantages and disadvantages explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
bone marrow injection orthopedics methodology indications contraindications 2024
Finding Sources
Finding Sources
Searching PubMed
bone marrow aspirate concentrate orthopedic injection
Reading File
Reading File
Reading Web Page
bone marrow aspirate concentrate BMAC orthopedic methodology procedure indications contraindications advantages disadvantages
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
bone marrow aspirate concentrate BMAC harvest technique iliac crest centrifuge procedure orthopedics 2024
Loading Image
Reading Web Page
BMAC bone marrow aspirate concentrate procedure steps technique centrifugation indications contraindications complications
Finding Sources
Reading File
Reading File
Generating Image
Generating Image
Generating Image
Generating Image
Here is a comprehensive, detailed account of bone marrow injections in orthopedics, covering all aspects you requested.
Bone Marrow Injections in Orthopedics
(Bone Marrow Aspirate / Bone Marrow Aspirate Concentrate - BMA/BMAC)
1. Introduction and Background
Bone marrow injection in orthopedics refers to the harvesting of autologous bone marrow - typically from the iliac crest - and its application (either as raw aspirate or as a concentrated product) to injured or diseased musculoskeletal tissues to stimulate healing and regeneration.
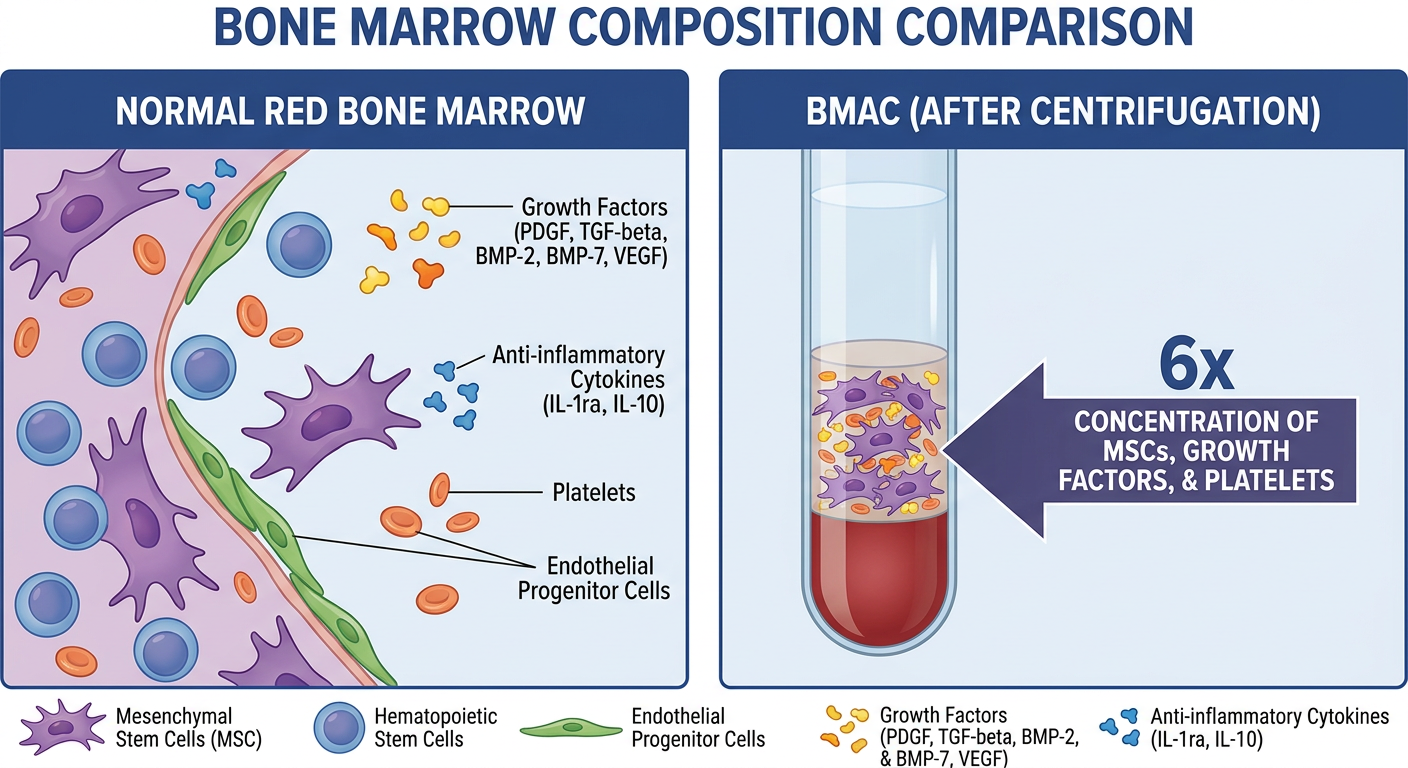
The product most commonly used clinically is Bone Marrow Aspirate Concentrate (BMAC), which is produced by centrifuging raw bone marrow aspirate to create a volume enriched 6-10x in:
- Mesenchymal Stem Cells (MSCs) - the key regenerative cells, comprising 0.001-0.01% of the bone marrow
- Hematopoietic progenitor cells
- Endothelial progenitor cells
- Growth factors: PDGF, TGF-β, BMP-2, BMP-7, VEGF, IGF-1
- Anti-inflammatory cytokines: IL-1ra, IL-10, IL-4
2. Biological Basis and Mechanism of Action
2.1 Why Bone Marrow?
The bone marrow is a rich repository of multipotent stem cells. MSCs can differentiate into:
- Osteoblasts - for bone repair
- Chondrocytes - for cartilage regeneration
- Tenocytes - for tendon healing
- Fibroblasts - for soft tissue repair
2.2 Mechanisms
| Mechanism | Effect |
|---|---|
| Osteoinduction | MSCs differentiate into osteoprogenitor cells → osteoblasts; BMPs stimulate new bone formation |
| Osteoconduction | Provides scaffold for bone ingrowth when used with allograft |
| Chondrogenesis | MSCs differentiate into chondrocytes, producing Type II collagen and aggrecan |
| Paracrine signaling | Secreted growth factors recruit host cells, stimulate angiogenesis and extracellular matrix production |
| Anti-inflammation | Cytokines (IL-1ra, IL-10) reduce synovial inflammation in OA |
| Immunomodulation | MSCs suppress T-cell activation, reducing the inflammatory milieu |
Importantly, preclinical studies (and data from Rockwood and Green's Fractures in Adults, 10th Ed., 2025) indicate that injected cells likely do not engraft permanently, but rather exert their effects through secreted bioactive factors and paracrine signaling.
3. Harvest Sites
Bone marrow can be harvested from multiple anatomic sites. The number of MSCs varies by location:
| Site | Notes |
|---|---|
| Posterior Superior Iliac Crest (PSIC) | Most common; highest MSC yield; 50-60 mL readily obtained |
| Anterior Iliac Crest | Alternative if prone positioning not possible |
| Proximal Tibia | Intraoperative convenience for lower extremity procedures |
| Distal Femur | Used during knee procedures |
| Calcaneus | Foot and ankle procedures |
| Proximal Humerus | Upper extremity procedures |
| Vertebral body | Spinal fusion procedures |
The posterior iliac crest remains the gold standard due to highest MSC density.
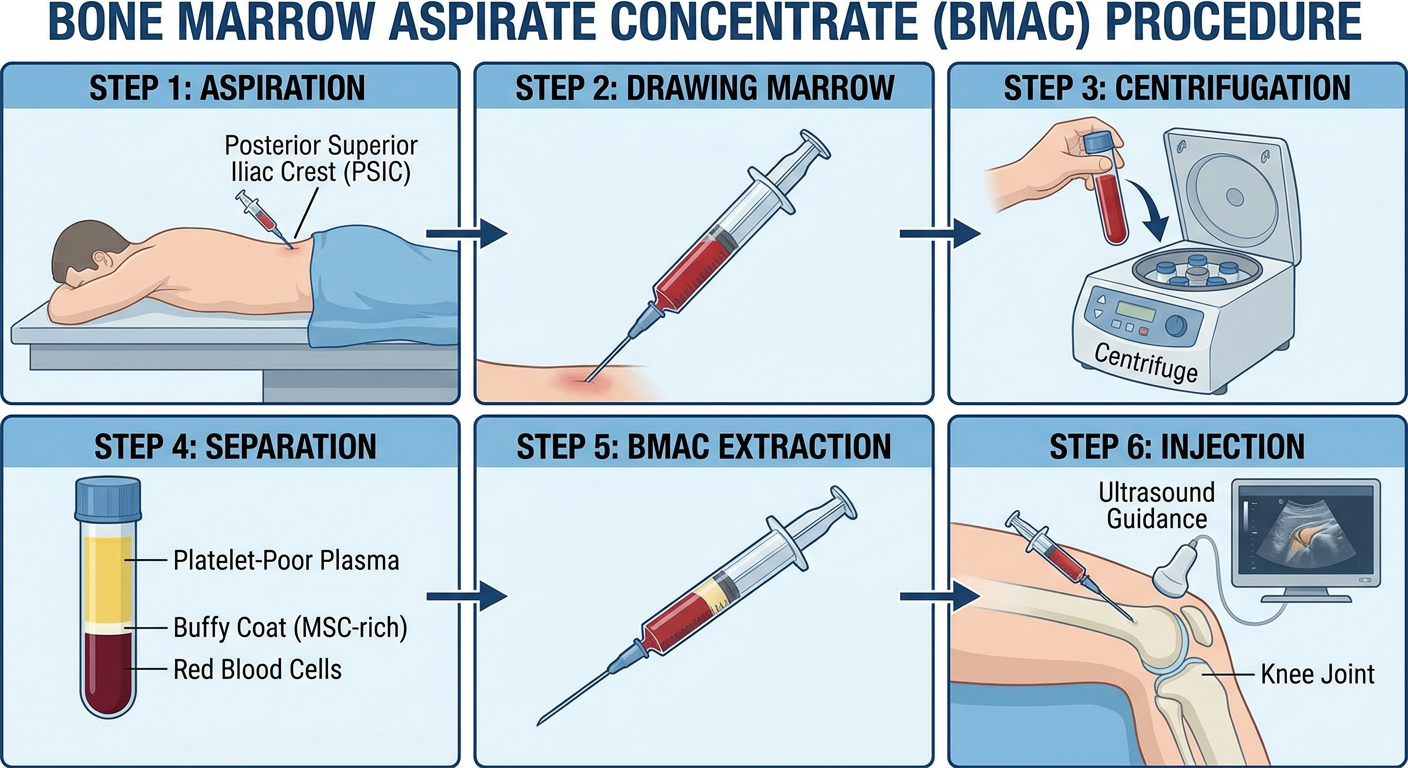
4. Methodology - Step-by-Step Procedure
4.1 Pre-Procedure
- Baseline blood tests: CBC, coagulation profile
- Patient counseling and informed consent
- Cessation of NSAIDs 5-7 days before procedure (reduces platelet function interference)
- Positioning: Prone (posterior iliac approach) or supine (anterior iliac approach)
- Sterile field preparation
- Anesthesia: Monitored anesthesia care (conscious sedation) or local anesthetic infiltration (1% lidocaine to skin, periosteum)
4.2 Bone Marrow Aspiration
Equipment needed:
- Bone marrow aspiration needle/cannula (e.g., Jamshidi needle, 11G or 8G)
- Anticoagulant-lined syringes (ACD-A - Acid Citrate Dextrose Solution A to prevent clotting)
- 10-60 mL syringes
Technique (Iliac Crest):
- Palpate and mark the posterior superior iliac spine (PSIS)
- Make a 5-7 mm stab incision through skin and subcutaneous tissue
- Insert the trocar cannula through the incision down to the iliac cortex
- Advance through the outer cortex into the cancellous bone with a rotational motion under controlled force
- Remove the trocar; confirm position - the cannula should be seated in cancellous bone
- Attach an ACD-A-primed syringe and aspirate 5-10 mL per site
- To obtain additional marrow, withdraw the needle slightly and redirect at a new angle (do NOT aspirate >10-15 mL per insertion - excessive volume dilutes with peripheral blood, reducing MSC concentration)
- Repeat at 2-4 separate insertion sites within the same skin incision to collect 60-120 mL total aspirate
Key technical point: Each syringe should contain only 5-10 mL per position to maintain MSC concentration. Large-volume aspiration from a single site dilutes with sinusoidal blood and reduces cell yield significantly.
4.3 Processing - Centrifugation (BMAC Preparation)
Two main centrifugation systems are in use:
- Single-spin systems (e.g., Arthrex Angel, Harvest SmartPrep, Zimmer BioCUE)
- Double-spin / density gradient systems (Ficoll or similar)
Typical protocol:
- Transfer aspirate to centrifuge tubes containing anticoagulant
- Centrifuge at 1,500-3,200 rpm for 7-15 minutes (system dependent)
- Results in 3 layers:
- Bottom: Red blood cells and granulocytes (discarded)
- Middle (buffy coat): MSCs, platelets, mononuclear cells - the target layer
- Top: Platelet-poor plasma
- Carefully extract the buffy coat layer (approximately 3-7 mL from 60 mL aspirate)
- The final BMAC product is ~6x concentrated compared to raw aspirate
From Rockwood and Green (2025): A typical 300 cm³ aspirate concentrates to approximately 50 cm³ with an average of 2,579 ± 1,121 MSCs/cm³.
4.4 Injection of BMAC
- Injection is performed image-guided (ultrasound or fluoroscopy) for intra-articular/precise delivery
- Volume injected: typically 3-7 mL
- For intra-articular (knee, hip, shoulder): single or combined with hyaluronic acid
- For nonunion/fracture: percutaneous injection directly into fracture gap under fluoroscopy
- For osteochondral defects: arthroscopic delivery onto defect site, often mixed with scaffold material
- For spinal fusion: mixed with allograft or osteoconductive matrix
Total procedure time: approximately 2 hours
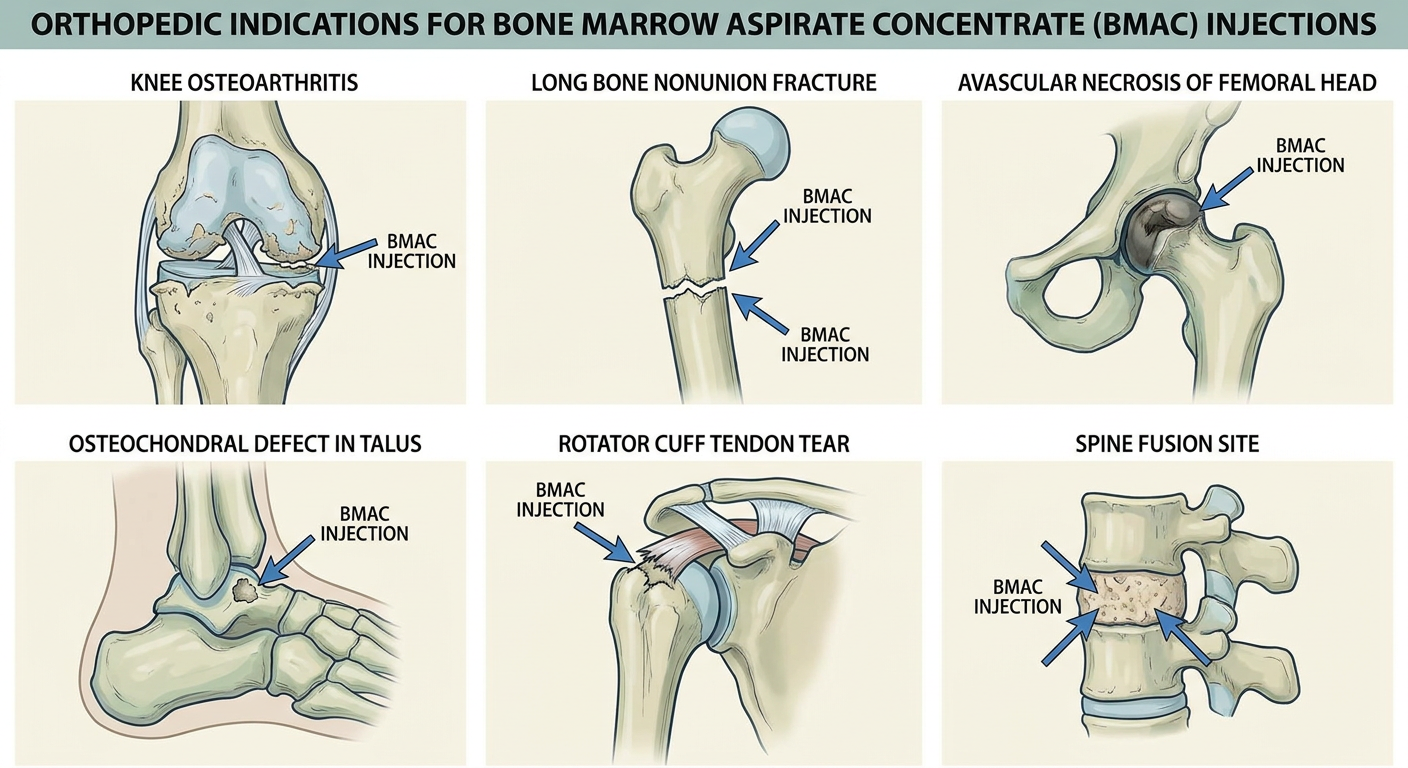
5. Indications
5.1 Established / Widely Used
| Indication | Evidence Level | Notes |
|---|---|---|
| Fracture Nonunion (long bones) | Level III-IV | Percutaneous BMAC injection; union rates 50-95% depending on type; highest rates in septic nonunion (83-100%) - Campbell's / Rockwood & Green |
| Delayed Union | Level III-IV | Early injection reduces time to union |
| Bone Defects / Grafting augmentation | Level IV | Mixed with cancellous allograft to augment osteogenic properties |
| Spinal Fusion | Level III | Combined with allograft/cage constructs |
| Osteochondral Defects (talus, knee) | Level III | BMAC + cartilage ECM scaffold shows superior MRI outcomes vs microfracture alone (Campbell's 2026) |
5.2 Regenerative / Biologics Applications
| Indication | Evidence Level | Notes |
|---|---|---|
| Knee Osteoarthritis | Level I-II | Multiple systematic reviews 2023-2024; BMAC/PRP superior to hyaluronic acid for pain and function |
| Hip Osteoarthritis | Level II-III | Systematic review (Giorgino et al, 2024) - promising but limited RCTs |
| Avascular Necrosis (AVN) of Femoral Head | Level II-III | Core decompression + BMAC injection is well-established for early stage AVN |
| Rotator Cuff Tears | Level III | Adjunct during repair to augment tendon healing |
| Tendinopathy (Achilles, patellar, lateral epicondyle) | Level III | Peritenonous injection |
| Ligament Reconstruction | Level III | Adjunct to ACL reconstruction |
| Unicameral Bone Cysts | Level III | Aspiration + injection with BMAC ± bone substitute (Campbell's Technique 27.xx) |
| Shoulder/Hip Arthritis | Level II | Intra-articular injection (2025 systematic review) |
| Foot and Ankle Fusion | Level III-IV | BMAC at arthrodesis sites for high-risk patients (Donaghue 2024) |
5.3 Open Fractures
A study by Hernigou et al. (cited in Rockwood and Green, 2025) demonstrated that early autologous BMC injection in 231 patients with severe open tibial fractures produced:
- Bone healing rate: 87.4% (vs 50.7% in controls)
- Significantly lower infection risk
6. Contraindications
6.1 Absolute Contraindications
| Contraindication | Reason |
|---|---|
| Active local or systemic infection / sepsis | Risk of seeding stem cells into infected environment; BMC injection into a purulent or active systemic infectious site is contraindicated |
| Active malignancy (especially hematologic malignancy - leukemia, lymphoma, myeloma) | Bone marrow may contain malignant cells; MSCs could promote tumor growth |
| Known coagulopathy / bleeding disorder (uncorrected) | Risk of uncontrolled hemorrhage at harvest and injection sites |
| Thrombocytopenia (platelets < 50,000/μL) | Inadequate hemostasis |
| Bone marrow disorders (aplastic anemia, myelodysplasia) | Insufficient or abnormal marrow yield |
6.2 Relative Contraindications
| Contraindication | Notes |
|---|---|
| Advanced age (>70-75) | Age-related decline in MSC count and potency; may reduce efficacy but not a hard contraindication |
| Morbid obesity (BMI >40) | Obese patients showed less benefit from BMAC for knee OA in a 2025 study (Pabinger et al.) |
| Autoimmune conditions on immunosuppression | Theoretical risk of altered MSC behavior; use with caution |
| Prior radiation to harvest site | Impairs bone marrow cellularity |
| End-stage arthritis (KL Grade IV) | Debated; 4-year data on KL Grade III-IV showed favorable outcomes |
| Anticoagulant therapy | Bridging/temporary cessation required |
| NSAIDs use | Should stop 5-7 days before procedure |
| Prior corticosteroid injection | Wait 4-6 weeks after intra-articular steroids before BMAC injection |
| Pregnancy | Insufficient safety data |
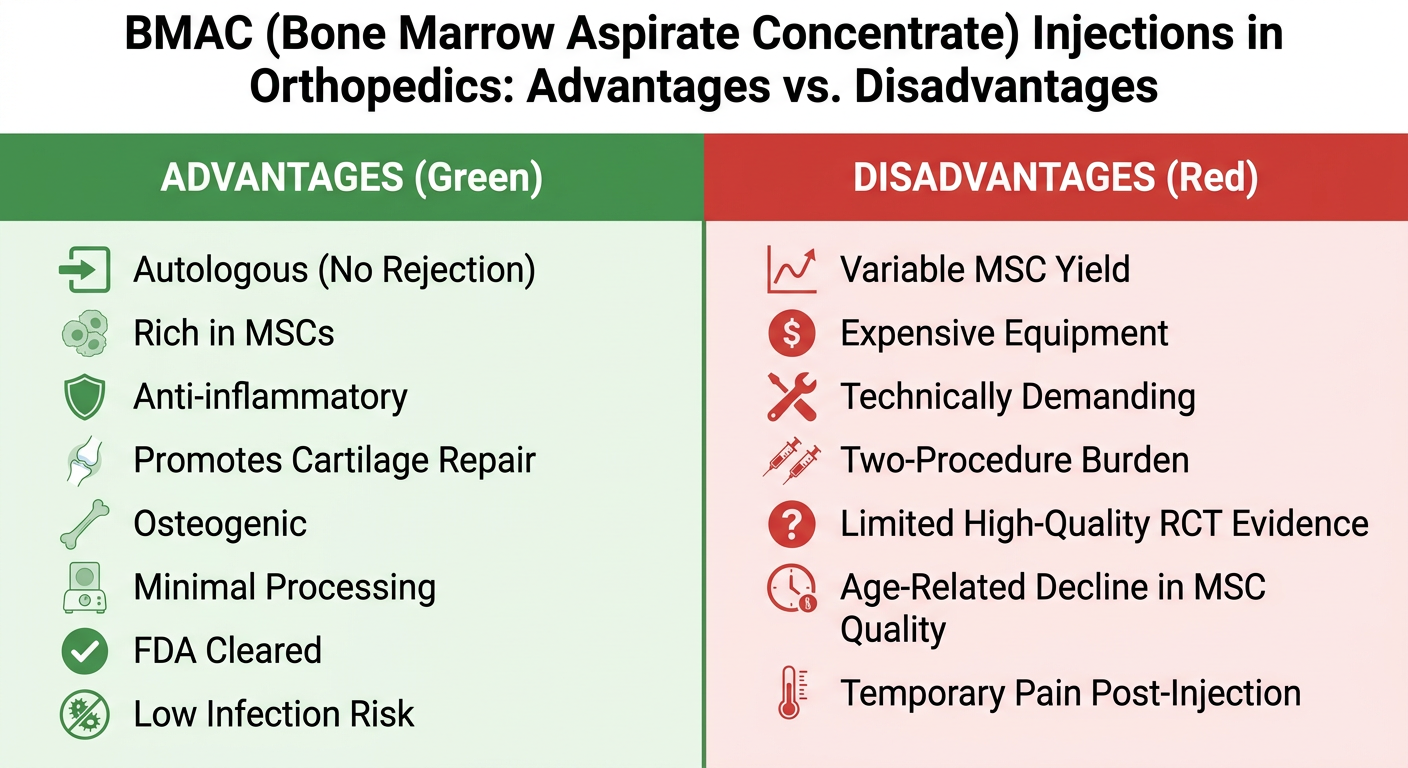
7. Advantages
| Advantage | Details |
|---|---|
| Autologous - no immunogenic risk | Patient's own cells; no risk of rejection, graft-versus-host disease, or disease transmission |
| Multi-lineage potential | MSCs can become bone, cartilage, tendon, or ligament - versatile across orthopedic conditions |
| Rich in growth factors | PDGF, TGF-β, BMP-2/7, VEGF, FGF - naturally concentrated cocktail without synthetic supplementation |
| Anti-inflammatory | IL-1ra and IL-10 down-regulate destructive inflammatory pathways in OA and post-injury states |
| FDA cleared (minimally manipulated) | BMAC produced without expansion or genetic manipulation qualifies as "minimally manipulated" under FDA guidelines |
| Single-session procedure | Harvest and injection performed in the same surgical session |
| Low risk of complications | Rate of serious adverse events is very low; main side effect is transient pain |
| No animal/donor products | Avoids risks of xenograft or allograft transmission |
| Synergistic with other biologics | Can be combined with PRP, hyaluronic acid, cartilage scaffolds, or bone substitutes |
| Disease-modifying potential | Unlike steroids or HA, BMAC may address OA pathophysiology rather than just symptoms |
8. Disadvantages and Limitations
| Disadvantage | Details |
|---|---|
| High variability in MSC yield | MSC content varies 10-100x between patients; age, health, and site affect harvest; no reliable pre-procedure predictors |
| Cost | Equipment (centrifuge systems), procedure time, and facility costs; typically $2,000-5,000 USD per procedure; usually not covered by insurance |
| Two-site burden | Iliac crest aspiration adds procedure time, donor site pain, and risk of complications |
| Technically demanding | Requires proper aspiration technique; poor technique drastically reduces MSC yield |
| Limited high-quality evidence | Most studies are Level III-IV; lack of large, well-powered, double-blind RCTs with long-term follow-up (Rockwood & Green, 2025) |
| No standardized protocol | Centrifugation speed, time, volume, injection site, and dose vary widely across institutions - making comparison difficult |
| Temporary donor site pain | Iliac crest soreness lasting 3-7 days is common |
| Age-related decline | MSC number and potency decline with age; reduced efficacy in elderly patients |
| Not curative in advanced OA | Delays rather than reverses severe joint degeneration |
| Regulatory uncertainty | More complex BMAC preparations (with ex vivo expansion) may require IND application |
| Risk of fat/hematoma at injection site | Rare but possible |
9. Complications
Harvest Site (Iliac Crest)
- Donor site pain (most common, 3-7 days)
- Hematoma at harvest site
- Injury to lateral femoral cutaneous nerve (LFCN) - paresthesia/meralgia paresthetica
- Superior gluteal artery injury (rare)
- Iliac wing fracture (very rare, usually with osteoporotic bone)
- Infection at harvest site
Injection Site
- Transient pain and swelling (most common)
- Infection (rare due to autologous nature)
- Hematoma
- Neurovascular injury (ultrasound guidance reduces this risk)
- Theoretical tumor promotion (in undetected malignancy)
10. Comparison with Other Biologics
| Parameter | BMAC | PRP | Hyaluronic Acid | Corticosteroid |
|---|---|---|---|---|
| Source | Bone marrow | Blood | Synthetic/Rooster combs | Synthetic |
| MSC content | High | None | None | None |
| Growth factors | High | Moderate | None | None |
| Anti-inflammatory | Moderate-High | Moderate | Mild | High (short-term) |
| Duration of effect | 6-24+ months | 3-12 months | 3-6 months | 1-3 months |
| Evidence for OA | Level I-II | Level I-II | Level I | Level I |
| Cost | High ($2k-5k) | Moderate ($500-1k) | Moderate ($200-500) | Low |
| Procedure complexity | High | Low | Low | Low |
| Disease modification | Possible | Unlikely | No | No |
A 2024 network meta-analysis (Jawanda et al., Arthroscopy, PMID 38331363) found PRP, BMAC, and HA all outperform corticosteroids in pain and function at minimum 6 months for knee OA.
A 2023 systematic review and meta-analysis (Belk et al., Arthroscopy, PMID 36913992) found patients receiving PRP or BMAC had significantly better outcomes than those receiving HA for knee OA.
11. From the Operative Orthopaedics Textbook
From Campbell's Operative Orthopaedics 15th Ed. (2026):
"When mixed with autogenous bone or perhaps even host bone marrow aspirate (BMA) or bone marrow aspirate concentrate (BMAC), cancellous allograft can be used in nonstructural applications... High-quality evidence comparing autogenous autograft with allograft combined with BMA or BMAC is lacking."
For osteochondral talar lesions:
"Satisfactory patient-reported outcomes and superior MRI results have been noted with micronized allogenic cartilage ECM with bone marrow concentrate (BMAC) compared with microfracture alone in arthroscopic repair of osteochondral talar lesions."
12. Special Considerations by Condition
12.1 Fracture Nonunion
- Best results in atrophic nonunions with adequate bone stock
- Percutaneous injection under fluoroscopy directly into fracture gap
- BMAC can be loaded onto scaffolds (bioactive glass, calcium phosphate)
- Evidence supports use in septic nonunion where BMAC reduced reinfection rate
12.2 Knee Osteoarthritis
- Most studied BMAC application
- Typical injection volume: 5-7 mL intra-articular
- Can be combined with HA for synergistic effect
- 4-year follow-up data (Pabinger et al., Sci Reports 2024) shows sustained benefit even in KL Grade III-IV
- Obese patients (high BMI) show significantly less benefit
12.3 Avascular Necrosis (AVN) of Femoral Head
- Standard approach: core decompression + BMAC injection into necrotic zone
- Best results in Steinberg Stage I-III (pre-collapse)
- BMAC promotes revascularization through VEGF and angiogenic factors
12.4 Osteochondral Defects
- Delivered arthroscopically in combination with cartilage ECM scaffolds
- BMAC provides MSCs that differentiate into chondrocyte-like cells within the scaffold
- Superior MRI and patient-reported outcomes vs microfracture alone
12.5 Spinal Fusion
- BMAC mixed with allograft in interbody or posterolateral fusion
- Augments osteogenic potential of allograft, which has limited intrinsic osteogenesis
13. Post-Procedure Care
- Activity restriction for 24-48 hours
- Ice and elevation of treated joint
- Avoid NSAIDs for 2-4 weeks post-injection (may impair MSC activity)
- Physical therapy can begin at 2-4 weeks
- Pain and swelling at injection site typically resolve within 3-7 days
- Clinical improvement often noted at 4-8 weeks, with maximum benefit at 3-6 months
- Full procedure time: approximately 2 hours (harvest + processing + injection)
14. Current Evidence Summary and Future Directions
What the evidence supports:
- BMAC is superior to hyaluronic acid for knee OA at 6+ months (Level I-II)
- BMAC is safe with minimal adverse events across all orthopedic applications
- BMAC combined with scaffolds improves osteochondral repair vs microfracture alone
- Early BMAC injection in open fractures significantly reduces infection risk and improves healing
Ongoing limitations:
- Lack of large RCTs with long-term follow-up
- No standardized centrifugation protocols
- Variability in MSC content between patients and centers
- Reimbursement challenges limit widespread adoption
- Multiple clinical trials ongoing (NCT05517434 ABLE OA trial completing 2026)
Emerging directions:
- BMAC combined with 3D bioprinted scaffolds
- Ex vivo expansion of MSCs (regulatory pathway under FDA IND)
- Combined BMAC + gene-activated matrices (BMP gene therapy)
- Point-of-care MSC quantification to predict responders
Key References
- Campbell's Operative Orthopaedics, 15th Ed. 2026 (Elsevier)
- Rockwood and Green's Fractures in Adults, 10th Ed. 2025 (Wolters Kluwer)
- Belk JW et al. Arthroscopy 2023 [PMID 36913992] - Meta-analysis: BMAC/PRP > HA for knee OA
- Jawanda H et al. Arthroscopy 2024 [PMID 38331363] - Network meta-analysis: BMAC/PRP/HA > Corticosteroids
- Moyal AJ et al. Eur J Orthop Surg Traumatol 2024 [PMID 39060552] - BMAC in long-bone nonunion
- Pabinger C et al. Sci Reports 2024 - 4-year results of BMAC for KL III-IV knee OA
- Zimmer Biomet Bone Marrow Aspiration Surgical Technique Guide
- Cleveland Clinic BMAC Procedure Overview
This is a shared conversation. Sign in to Orris to start your own chat.