Varicose vein in depth for 30 marks long question
Reading File
Finding Sources
Finding Sources
Searching PubMed
varicose veins management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material from Bailey & Love, Harrison's, and Schwartz's to write a thorough 30-mark answer. Let me compile everything into a comprehensive, well-structured response.
Varicose Veins - In-Depth (30 Marks)
Definition
Varicose veins are dilated, bulging, tortuous superficial veins measuring at least 3 mm in diameter, containing incompetent (refluxing) valves. The term derives from the Latin varix, meaning "twisted vein." They are distinguished from:
- Reticular veins: dilated intradermal veins, blue-green, 1-3 mm, do not protrude
- Telangiectasias (spider/thread veins): <1 mm, near skin surface, forming linear or spider-web patterns
(Harrison's Principles of Internal Medicine, 22nd Ed.)
Clinical Photo
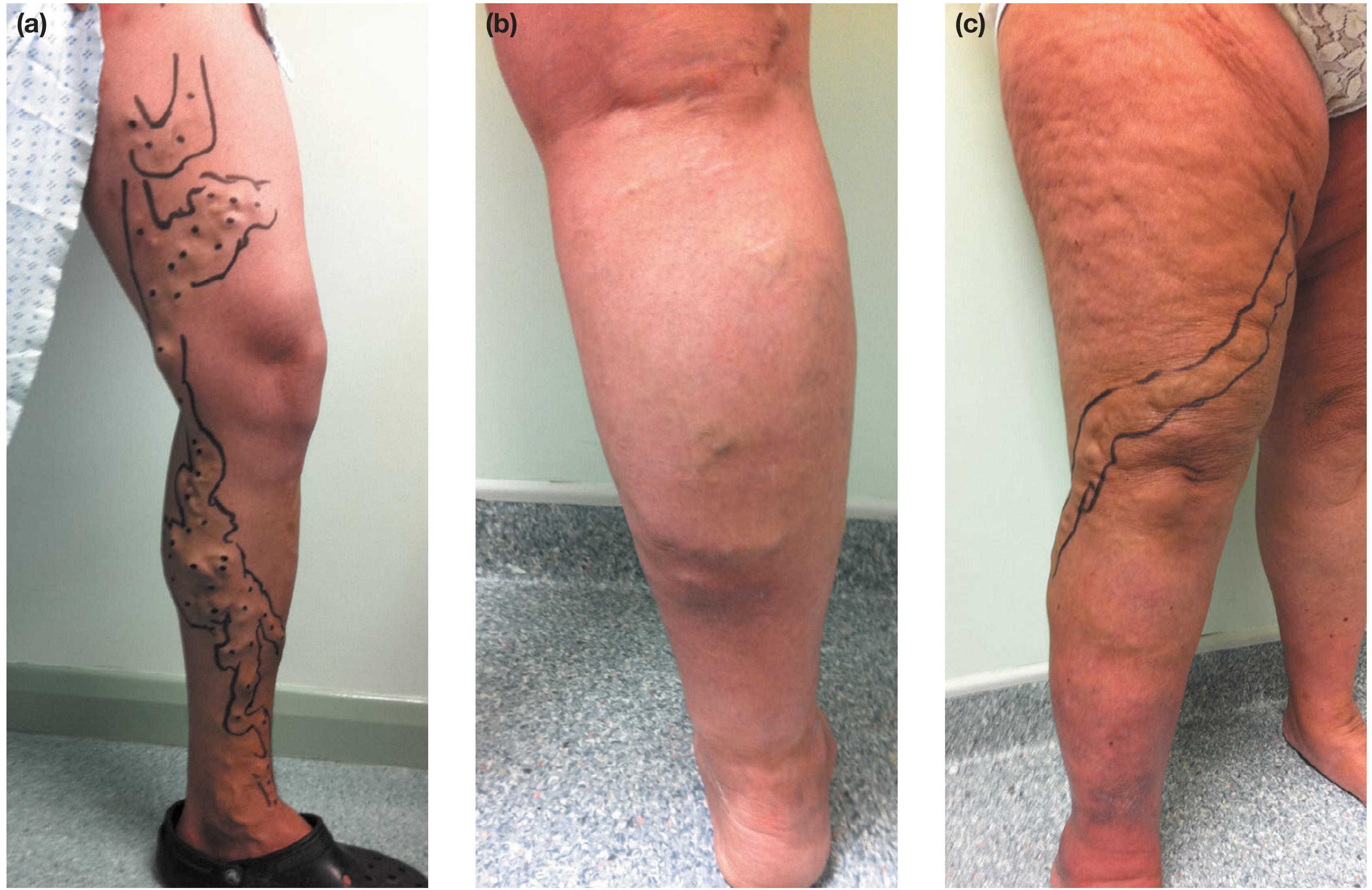
Fig: (a) left GSV territory varicosities marked for intervention; (b) SSV territory with recent phlebitis; (c) AAGSV territory with gaiter area skin changes. (Bailey & Love, 28th Ed.)
Epidemiology
The adult prevalence of visible varicose veins is 30-50%. Key risk factors include:
| Factor | Detail |
|---|---|
| Sex | Higher prevalence in women than men |
| Age | Increases with age - Edinburgh Vein Study: 11.5% (18-24 yrs) rising to 55.7% (55-64 yrs) |
| Pregnancy | Increases risk via hormonal + mechanical effects |
| Family history | ~50% of primary varicose veins have a family history |
| Obesity/BMI | Higher BMI associated with greater risk |
| Prolonged standing | Inconclusive but likely contributory |
| Ethnicity | Influences prevalence |
(Bailey & Love's Short Practice of Surgery, 28th Ed.)
Anatomy Relevant to Varicose Veins
Superficial Venous System
- Great Saphenous Vein (GSV): longest vein in the body; originates medial foot, ascends anterior to medial malleolus, along medial calf and thigh, drains into the common femoral vein at the saphenofemoral junction (SFJ)
- Small Saphenous Vein (SSV): originates dorsolateral foot, ascends posterior to lateral malleolus, drains into the popliteal vein at the saphenopopliteal junction (SPJ)
Deep Venous System
- Paired anterior tibial, posterior tibial, and peroneal veins converge to form the popliteal vein - femoral vein - common femoral vein - external iliac - IVC
Perforating Veins
- Connect superficial to deep system; normally allow blood flow from superficial to deep; bicuspid valves throughout direct flow centrally
(Harrison's, 22nd Ed.)
Classification
Primary vs. Secondary
Primary varicose veins (~most common):
- Originate in the superficial system
- Result from intrinsic weakness of the vein wall, defective valve structure/function, and high intraluminal pressure
- ~50% have a family history
Secondary varicose veins:
- Result from deep venous hypertension
- Causes: deep-vein thrombosis (post-thrombotic syndrome), deep venous obstruction, incompetent perforating veins, arteriovenous fistulas, Klippel-Trenaunay syndrome
(Harrison's 22nd Ed., Bailey & Love 28th Ed.)
CEAP Classification (Clinical-Etiology-Anatomy-Pathophysiology)
The internationally accepted classification system:
Clinical (C):
| Class | Description |
|---|---|
| C0 | No visible/palpable signs |
| C1 | Telangiectasia or reticular veins |
| C2 | Varicose veins |
| C3 | Oedema |
| C4a | Pigmentation or eczema |
| C4b | Lipodermatosclerosis or atrophie blanche |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
Etiology (E): Ec (congenital), Ep (primary), Es (secondary), En (no identifiable cause)
Anatomy (A): As (superficial), Ad (deep), Ap (perforating), An (none identified)
Pathophysiology (P): Pr (reflux), Po (obstruction), Pr,o (both), Pn (none identifiable)
(Bailey & Love, 28th Ed.)
Pathophysiology
The fundamental mechanism is chronic venous hypertension resulting from:
1. Valve Incompetence and Reflux
- Normal valves direct blood centrally (toward the heart)
- Valve leaflet failure allows retrograde flow (reflux) when standing
- Superficial reflux is defined as retrograde flow lasting >0.5 seconds; deep vein reflux >1 second
2. Vein Wall Changes
Progressive changes in the wall include:
- Inflammatory cell infiltration and activation
- Dysfunctional smooth muscle cell proliferation
- Collagen deposition
- Decreased elastin content
- Increased matrix metalloproteinases (MMPs)
- These lead to loss of compliance, dilatation, elongation (causing tortuosity), and secondary valvular dysfunction
3. Downstream Consequences
- Venous hypertension causes increased capillary pressure
- Extravasation of fluid, red blood cells, and fibrin into tissues
- RBC breakdown leads to haemosiderin deposition (pigmentation)
- Fibrin pericapillary cuffing impairs tissue oxygenation
- Chronic inflammation leads to lipodermatosclerosis and ulceration
(Bailey & Love, 28th Ed.; Harrison's, 22nd Ed.)
Clinical Features
Symptoms
Patients describe:
- Aching, heaviness, throbbing, burning, or bursting sensation
- Symptoms worsen throughout the day and with prolonged standing
- Relieved by elevation or compression hosiery
- Itching (more common with complications)
- Ankle swelling
- Unsightly cosmetic appearance
Signs
- Tortuous, dilated subcutaneous veins - visible and palpable
- GSV incompetence produces medial thigh and calf varicosities
- SSV incompetence produces posterolateral calf varicosities
- AAGSV incompetence produces anterolateral thigh and calf varicosities
- Saphena varix: a painless groin swelling apparent on standing, disappears on lying (can mimic a hernia; impulse on cough)
(Bailey & Love, 28th Ed.)
Complications
Chronic Complications (skin changes)
| Feature | Description |
|---|---|
| Oedema | Pitting initially, later non-pitting |
| Hyperpigmentation | Haemosiderin deposits from RBC extravasation |
| Venous eczema (stasis dermatitis) | Erythema, weeping, crusting |
| Lipodermatosclerosis | Induration + inflammation in lower leg above ankle - "inverted champagne bottle" deformity |
| Atrophie blanche | White scar patches with telangiectasias, near medial malleolus |
| Corona phlebectatica | Fan-shaped intradermal veins near ankle/foot |
| Venous ulcer | Shallow, irregular border, granulation tissue base, near malleoli - a C6 CEAP lesion |
Acute Complications
- Superficial vein thrombosis (thrombophlebitis): painful, red, indurated cord along varicosities
- Bleeding: from ruptured varicosities - can be severe and alarming (especially at night); first aid is elevation and pressure
- Deep vein thrombosis (less common, associated with propagation of SVT)
(Harrison's, 22nd Ed.; Bailey & Love, 28th Ed.)
Investigations
Duplex Ultrasound (Investigation of Choice)
- Tourniquet tests and handheld Doppler have been abandoned in favour of duplex ultrasound
- All patients should undergo duplex scanning before intervention
- Performed with patient standing
- High-frequency linear array transducer: 7.5-13 MHz
- Aims to establish:
- Presence and distribution of reflux in deep and superficial systems
- Exact extent of reflux including affected junctions and perforators
- Deep venous obstruction
- Suitability of veins for specific treatments (diameter, extent, tortuosity)
- Presence of deep venous disease
Mickey Mouse sign: transverse B-mode image at groin shows the common femoral artery (large circle), CFV (medium circle), and GSV (small circle)
Bedside Tests (Historical - now replaced by duplex)
- Brodie-Trendelenburg test: Leg elevated to empty veins, tourniquet applied to proximal thigh, patient stands. Rapid refilling after tourniquet removal = superficial incompetence. Filling while tourniquet is on = deep venous insufficiency
- Perthes test: Tourniquet applied, patient walks. If veins empty = deep system patent. If veins distend = deep obstruction
Other Investigations
- Plethysmography (photoplethysmography/air plethysmography) - assesses overall venous function
- Venography - reserved for complex/recurrent cases
- CT/MRI venography - for pelvic venous insufficiency or suspected outflow obstruction
(Bailey & Love, 28th Ed.; Harrison's, 22nd Ed.)
Differential Diagnosis
- Lymphoedema: non-pitting, no varicosities, Stemmer's sign positive
- Deep vein thrombosis: acute, painful, warm
- Congestive cardiac failure: bilateral pitting oedema
- Hypoalbuminaemia (nephrotic syndrome, liver disease): bilateral oedema
- Lipoedema: bilateral, spares the foot, painful
- Arteriovenous fistula (secondary varicosities with bruit/thrill)
- Klippel-Trenaunay syndrome: port-wine stain + varicosities + limb hypertrophy
Management
Conservative (Non-operative) Management
Indications: mild symptoms, preference, pregnancy, bilateral occlusive deep venous disease, patient unfit for intervention.
-
Compression hosiery (stockings):
- Graduated compression: 20-30 mmHg, 30-40 mmHg, 40-50 mmHg
- Knee-high to waist-high
- Relieves symptoms in many patients; does not cure the underlying reflux
-
Lifestyle modifications:
- Weight reduction
- Avoid prolonged standing
- Regular walking (calf muscle pump activation)
- Leg elevation
Indications for Active Intervention
- Symptoms worsening or unrelieved by compression
- Lipodermatosclerosis
- Venous ulcer (healed C5 or active C6)
- Recurrent superficial thrombophlebitis
- Bleeding varicose veins
- Significant cosmetic concern
Interventional Management Options
1. Endovenous Thermal Ablation (FIRST-LINE - minimally invasive)
A catheter/device is inserted percutaneously into the incompetent vein; tumescent local anaesthetic is injected around the vein (compresses vein, hydro-dissects nerves, acts as heat sink). Thermal energy destroys the vein wall causing permanent occlusion.
Endovenous Laser Ablation (EVLA):
- Flexible glass fibre inserted into the vein
- Laser energy (typically 1470 nm wavelength) transmitted to the tip
- Vigorous thermal energy generation causes vein wall destruction
- Suitable for any vein accepting a guidewire
- Higher efficacy in large diameter veins (>15 mm)
- Requires laser safety protocols
Radiofrequency Ablation (RFA):
- Uses metal coil catheter (e.g. ClosureFast)
- Automatic treatment cycle on single button press - shorter learning curve
- Slightly less pain and bruising post-procedure
- Less suitable for large diameter veins
Both techniques treat junctional and truncal incompetence only; residual varicosities require adjuvant phlebectomy or sclerotherapy.
2. Foam Sclerotherapy (Ultrasound-Guided Foam Sclerotherapy - UGFS)
- Sclerosant solution made into foam using Tessari method (1:3 or 1:4 ratio of sclerosant to air oscillated between two syringes via 3-way tap)
- Common agents: sodium tetradecyl sulfate, polidocanol
- Destroys venous endothelium; vein fibroses
- Leg elevated before injection; maximum 10-12 mL per session
- Advantages: no tumescent anaesthetic, treats tortuous veins, can treat over damaged skin, low cost
- Disadvantages: lower efficacy than thermal ablation, higher reintervention rates, risk of phlebitis and pigmentation
- Liquid sclerotherapy used for telangiectasias (smaller concentrations)
(Schwartz's Principles of Surgery, 11th Ed.; Bailey & Love, 28th Ed.)
3. Mechanochemical Ablation (MOCA - e.g., ClariVein)
- Rotating wire disrupts endothelium mechanically; sclerosant delivered simultaneously
- No tumescent anaesthetic required
- Good for smaller veins; does not require thermal energy
4. Cyanoacrylate Glue Ablation (VenaSeal)
- Medical adhesive injected into the vein, sealing it shut
- No tumescent anaesthetic
- No compression hosiery required post-procedure
5. Surgical Treatment (Still indicated in selected cases)
Saphenofemoral Junction (SFJ) Ligation and GSV Stripping:
- Under general or spinal anaesthesia
- Groin crease incision to expose SFJ
- Tributaries ligated (superficial inferior epigastric, superficial circumflex iliac, external pudendal veins)
- Flush SFJ ligation performed
- GSV stripped retrogradely to the knee using a stripper
- Concurrent avulsion phlebectomy (stab avulsion) of varicosities via 2-3 mm incisions
SSV surgery: patient prone; SPJ identified (variable anatomy - duplex marking essential), SPJ ligated, SSV stripped.
(Bailey & Love, 28th Ed.)
Complications of Surgery / Treatment
Complications of Standard Varicose Vein Surgery
| Complication | Notes |
|---|---|
| Haematoma | Common; groin or along stripped vein |
| Wound infection | Groin incision especially |
| DVT/PE | TED stockings + mobilisation |
| Saphenous nerve injury | Paraesthesia/numbness medial lower leg (GSV stripping below knee) |
| Sural nerve injury | SSV stripping |
| Common femoral vein/artery injury | Rare but serious |
| Lymphocoele / lymphatic fistula | Groin |
| Recurrence | Due to neovascularisation in groin, missed sites, new disease |
(Bailey & Love, 28th Ed.)
Varicose Veins in Special Circumstances
Varicose Veins and Pregnancy
- Hormonal changes (progesterone) cause vein wall relaxation
- IVC compression by gravid uterus raises venous pressure
- Management: compression hosiery throughout pregnancy; definitive treatment deferred until 3-6 months after delivery
Bleeding Varicose Veins
- May be life-threatening in elderly patients on anticoagulants
- First aid: lie patient flat, elevate limb, apply firm pressure
- Definitive treatment: injection sclerotherapy or surgery
Venous Ulcers
- C6 CEAP; typically near medial malleolus
- Shallow, irregular border, granulation tissue base
- Management: compression bandaging (multilayer), treatment of underlying reflux, wound care
- Compression increases healing rates (Cochrane Review)
- Physiotherapy (leg exercises, calf pump activation) also beneficial
Summary Table: Treatment Options
| Method | Anaesthesia | Mechanism | Best For |
|---|---|---|---|
| EVLA | Tumescent LA | Laser thermal | GSV/SSV reflux, large veins |
| RFA | Tumescent LA | Radiofrequency thermal | GSV/SSV reflux, standard |
| UGFS | None | Chemical endothelial damage | Tributary veins, recurrences |
| MOCA | None | Mechanical + chemical | Mid-sized veins |
| Cyanoacrylate | None | Mechanical occlusion | Straight truncal veins |
| Surgery | GA/spinal | Excision/stripping | Any, complex recurrences |
| Compression | N/A | Symptomatic | Conservative, pregnancy |
Recent Evidence (2024-2025)
- A 2025 systematic review (PMID 41390389) comparing endovenous ablation vs surgical stripping found that endovenous techniques achieve comparable or superior clinical effectiveness with better patient-reported outcomes, supporting their use as first-line intervention.
- A 2024 systematic review (PMID 39025298) on anatomical reflux patterns confirmed that GSV reflux is the most common pattern in primary chronic venous disease, informing targeted treatment planning.
- A 2025 systematic review (PMID 40504402) confirms physiotherapy (calf exercises, compression, positioning) improves venous ulcer healing alongside standard wound care.
Key Points for Exam
- Varicose veins = dilated superficial veins ≥3 mm with valvular reflux
- Prevalence 30-50%; increased risk with female sex, age, pregnancy, family history, obesity
- Primary (intrinsic valve/wall defect) vs. secondary (DVT, AV fistula)
- CEAP classification C0-C6 is the gold standard for clinical staging
- Pathophysiology: valve failure → retrograde flow → chronic venous hypertension → skin changes → ulceration
- Investigation of choice: duplex ultrasound standing with augmentation
- Management ladder: compression → endovenous thermal ablation (first-line) → foam sclerotherapy → surgery
- EVLA and RFA are equally effective; RFA has slightly lower pain; EVLA better for very large veins
- Complications include thrombophlebitis, bleeding, chronic skin changes, and venous ulceration
- Saphenous nerve injury is the key nerve injury in GSV stripping below the knee
Sources:
- Bailey & Love's Short Practice of Surgery, 28th Edition
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
- Schwartz's Principles of Surgery, 11th Edition
- Gray's Anatomy for Students
- Lim EQ et al. BMC Surg 2025 [PMID 41390389]
- Tan MKH et al. J Vasc Surg Venous Lymphat Disord 2024 [PMID 39025298]
Create a summary document on varicose vein management algorithms
Asking for Preferences
Reading File
Running Command
Writing File
Running Command
Editing File
Running Command
Running Command
Your PDF is ready for download:
Varicose Vein Management Summary
PDF Document · PDF
Here's what's inside the document (4 pages, professionally formatted for junior doctors/residents):
Page 1
- Title block with colour-coded section pills
- Section 1 - Definition & Classification: venous spectrum table (telangiectasia → reticular → varicose), primary vs secondary side-by-side comparison boxes
Page 2
- Section 2 - CEAP Classification: full C0–C6 table with colour-coding (red for C6, green for C5, amber for C4) and management actions per class
- Section 3 - Clinical Assessment Algorithm: 5 step-by-step numbered flowchart steps (History → Examination → Duplex USS → Secondary causes → CEAP grading) with a clinical pearl banner on duplex replacing tourniquet tests
Page 3
- Section 4 - Management Algorithm: visual flowchart-style layout - conservative vs intervention branches, deep system patent/obstructed decision tree, intervention selection
- Section 5 - Treatment Modalities Table: EVLA, RFA, UGFS, MOCA, VenaSeal, Surgery, Compression - mechanism, anaesthesia, best use, key points
Page 4
- Section 6 - Special Situations: colour-coded boxes for venous ulcer, thrombophlebitis, bleeding varicosities, pregnancy, recurrence
- Section 7 - Complications Table: chronic + acute + post-treatment complications with management
- Section 8 - Duplex USS Quick Reference: protocol checklist + reflux definitions side-by-side
- Section 9 - Clinical Pearls: 15 high-yield facts including 2025 evidence (PMID 41390389)
- References from Bailey & Love 28th Ed, Harrison's 22nd Ed, Schwartz's 11th Ed
Generate a case-based exam question worksheet on varicose vein management
Asking for Preferences
Running Command
Writing File
Running Command
Running Command
Your worksheet is ready:
Varicose Vein Worksheet
PDF Document · PDF
Here's what the worksheet contains:
Structure
Part I - Clinical Questions (all cases together for exam simulation)
Part II - Answer Key with Explanations (on a separate page)
The 10 Cases & 15 Questions
| Case | Vignette | Difficulty | Topic |
|---|---|---|---|
| 1 | 48F, medial thigh varicosities, 2 pregnancies | Easy | CEAP Dx + Investigation |
| 2 | 62M, lipodermatosclerosis, partial compression relief | Medium | CEAP C4b + Intervention |
| 3 | 34F, SVT extending to within 2.5 cm of SPJ | Medium | Thrombophlebitis |
| 4 | 78M on warfarin, profuse spontaneous bleed | Hard | Emergency management |
| 5 | 29F, 22 weeks pregnant, new varicosities | Easy | Pregnancy / Conservative |
| 6 | 70M, medial malleolus ulcer, ABPI 0.9 | Medium | Venous ulcer (x2 Qs) |
| 7 | Post-op numbness medial lower leg after GSV stripping | Medium | Surgical complications |
| 8 | 45M, 7mm GSV reflux, needs quick return to work | Hard | EVLA vs UGFS + tributaries |
| 9 | 52F, painless groin lump, appears on standing | Medium | Saphena varix DDx |
| 10 | 58M, recurrent varicosities 8 years post-surgery | Hard | Neovascularisation (x2 Qs) |
Answer Key Features
- Quick reference answer grid at the top (all 15 answers at a glance)
- Full explanation for each correct answer (mechanism + clinical reasoning)
- Explanation for each distractor (why each wrong option is wrong)
- Self-assessment scoring guide (Excellent/Good/Average/Needs Improvement)
- Referenced to Bailey & Love, Harrison's, Schwartz's, and 2024-25 PubMed evidence
This is a shared conversation. Sign in to Orris to start your own chat.