Premalignant lesions of skin
Reading File
Finding Sources
Finding Sources
Searching PubMed
premalignant skin lesions management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Excellent - I now have rich content and clinical images from multiple authoritative dermatology textbooks. Let me compile a comprehensive answer.
Premalignant Lesions of the Skin
Premalignant (or potentially malignant) skin lesions are those with an increased risk of transforming into invasive cancer, most commonly squamous cell carcinoma (SCC) or melanoma. The atypical cells are confined to the epidermis in most cases; invasion has not yet occurred.
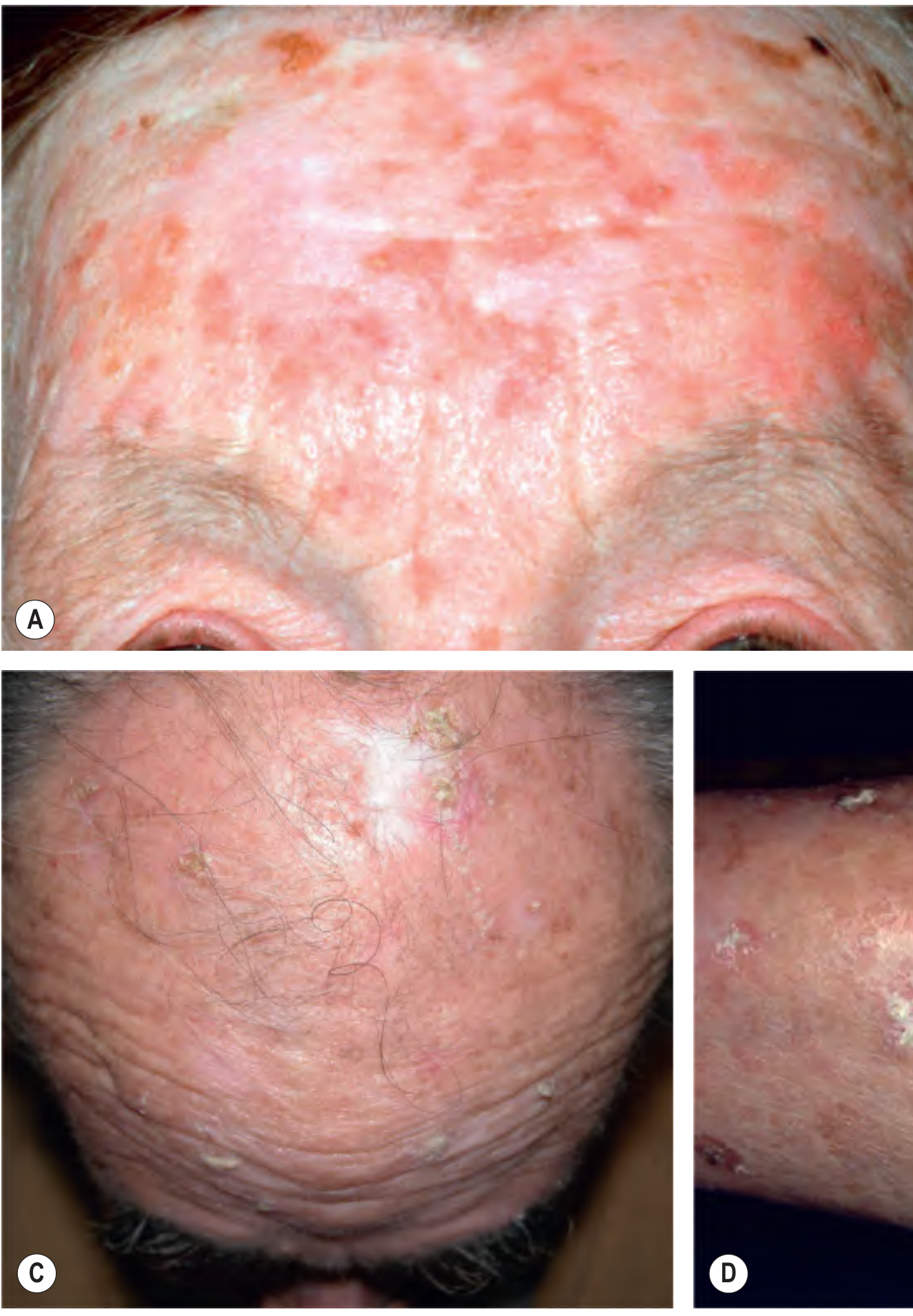
1. Actinic Keratosis (Solar Keratosis)
The most common premalignant skin lesion.
Pathogenesis & Epidemiology
Actinic keratoses (AKs) arise from cumulative UV-induced DNA damage to keratinocytes. The term "actinic keratosis" is preferred over "solar keratosis" (the abbreviation SK overlaps with seborrheic keratosis). Risk is highest in:
- The elderly
- Lighter Fitzpatrick skin phototypes (I-II)
- History of chronic cumulative sun exposure
- Immunosuppressed patients (organ transplant recipients have markedly increased risk)
Clinical Features
AKs present on chronically sun-damaged skin of the head, neck, upper trunk, dorsal hands, and forearms. The typical lesion is a rough erythematous macule or papule with white-to-yellow scale - often easier to feel (rough, sandpaper texture on palpation) than to see.
Lesions cluster in areas of highest cumulative UV exposure: superior helix of the ear, upper forehead, supraorbital ridge, nasal bridge, malar eminences, dorsal hands, extensor forearms, bald scalp.
Clinical Subtypes
| Subtype | Features |
|---|---|
| Classic | Rough erythematous macule/papule with scale |
| Hypertrophic (hyperkeratotic) | Papule/plaque with thick scale-crust and erythematous base; may form a cutaneous horn |
| Pigmented | Resembles lentigo; lacks the typical erythema |
| Lichenoid | Resembles lichen planus clinically and histologically |
| Atrophic | Thin, slightly depressed; can be subtle |
| Actinic cheilitis | Involves the lower lip; represents AK on mucosal surface |
Malignant Potential
The risk of an individual AK progressing to invasive cutaneous SCC (cSCC) is estimated at 0.1% per lesion per year, though population-level estimates range from 0.1% to 20%. AKs may spontaneously regress but can reappear at the same site. - Dermatology 2-Volume Set 5e, p. 2254
Treatment
Lesion-directed:
- Cryotherapy (liquid nitrogen) - the most widely used method; single freeze-thaw cycle of 8-10 seconds; 1-2 mm margin; cure rates up to 99% reported. Longer freeze times for hypertrophic AKs.
- Surgical excision - reserved for suspicious lesions needing histology
Field-directed (for multiple/confluent lesions):
- Topical 5-fluorouracil (5-FU) 5% or 0.5% - induces inflammatory destruction of dysplastic keratinocytes
- Topical imiquimod 5% or 3.75% - immunomodulator (TLR-7 agonist)
- Diclofenac 3% gel (Solaraze) - COX-2 inhibitor mechanism
- Ingenol mebutate gel - short-duration treatment
- Photodynamic therapy (PDT) - may have better cosmetic outcomes than cryotherapy for individual lesions (Cochrane review)
- Topical calcipotriol + 5-FU - combination showing efficacy in recent systematic review (PMID: 38783539)
A 2026 meta-analysis comparing PDT vs imiquimod for AK (PMID: 41578002) found both are effective field-directed therapies with comparable efficacy.
Chemoprevention: Acitretin (25 mg/day) has been shown in a prospective crossover study to prevent SCC development in renal transplant recipients, and reduces keratinocyte carcinoma development in xeroderma pigmentosum and basal cell nevus syndrome. - Dermatology 2-Volume Set 5e
2. Bowen's Disease (Squamous Cell Carcinoma in Situ)
Definition & Features
Bowen's disease is full-thickness epithelial dysplasia - squamous cell carcinoma confined to the epidermis (in situ). It typically presents as a slowly growing, scaly, erythematous plaque that can resemble eczema or psoriasis (biopsy is essential for diagnosis).
- Common on sun-exposed sites (face, scalp, dorsal hands, lower legs)
- Genital variant: Erythroplasia of Queyrat (glans penis) - presents as a red, velvety plaque
Malignant Potential
- Fewer than 5% of cutaneous Bowen's disease lesions progress to invasive SCC
- However, 10%-30% of genital lesions (erythroplasia of Queyrat) become invasive - Dermatology 2-Volume Set 5e
Treatment
- 5-FU topical or imiquimod
- Photodynamic therapy
- Cryotherapy (though cure rates are lower - ~50% in some studies with 2 freeze-thaw cycles)
- Surgical excision with 4-5 mm margins
- Radiotherapy: 40-50 Gy in 10-20 fractions - 5-year cure rates of 98-100%
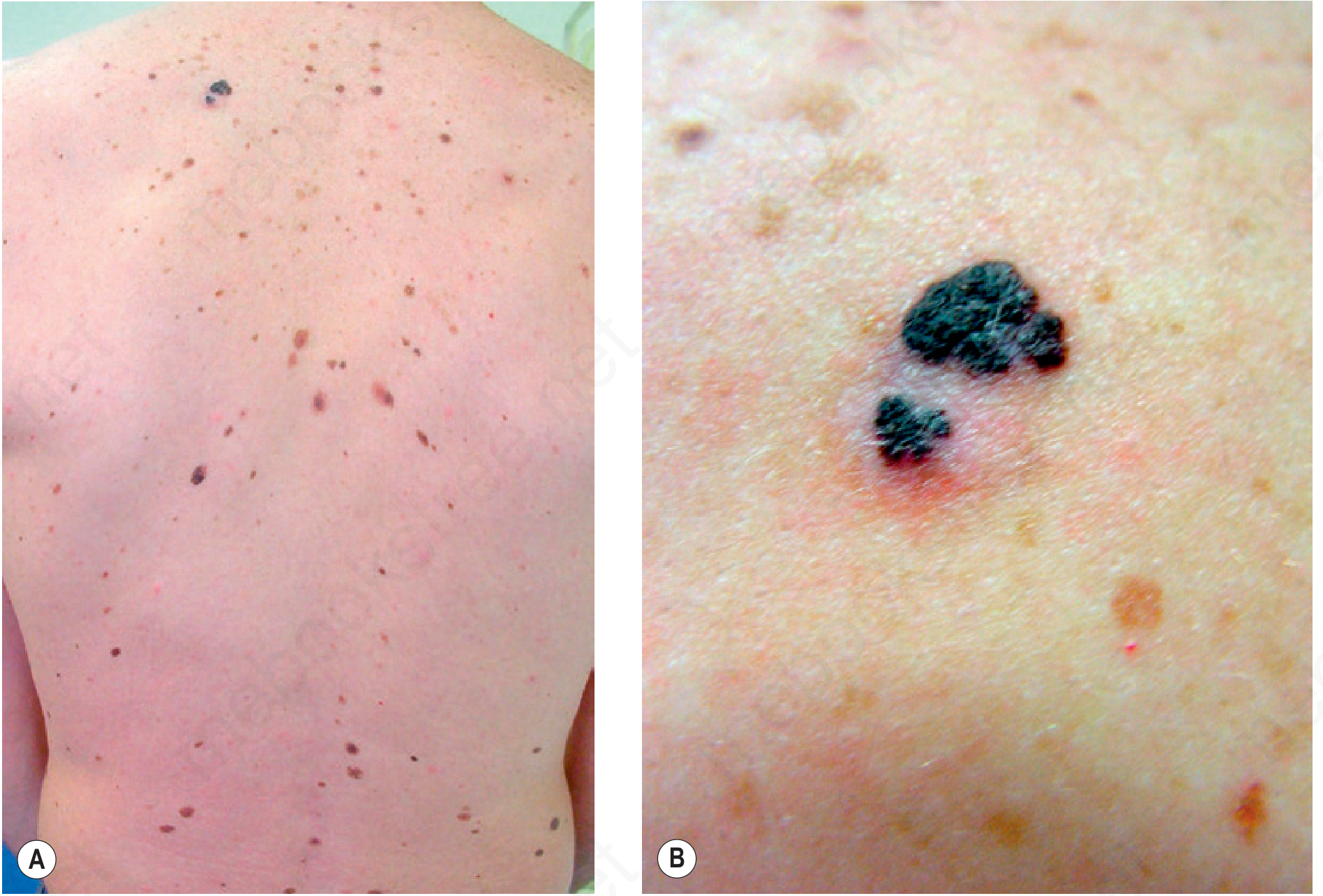
3. Dysplastic Nevus (Atypical Nevus / Clark Nevus)
Background
First described by Clark et al. in 1978 in the context of familial melanoma ("B-K mole syndrome"). Patients with dysplastic nevi in at least two blood relatives with melanoma have a lifetime risk of melanoma approaching 100%. The condition is called Dysplastic Nevus Syndrome (DNS) or Familial Atypical Multiple Mole-Melanoma (FAMM) syndrome.
Genetics
- ~25-33% of familial melanoma cases have germline mutations in CDKN2A (p16/INK4A) on chromosome 9p - encodes an inhibitor of CDK4, suppressing cell proliferation
- Mutations in CDK4 account for a smaller subset of familial melanomas
Clinical Features
- Size: Usually 5-12 mm (common acquired nevi are ≤6 mm)
- Color: Variegated tan, brown, and pink; the pink component is in the macular portion
- Border: Irregular, indistinct
- Structure: A macular component is always present, often surrounding a papular center ("fried egg" appearance)
- Predominate on the back and sun-exposed areas
- Sporadic dysplastic nevi occur in 5-20% of the general population and are not necessarily a marker for DNS
Histology
Architectural disorder and cytologic atypia at the dermal-epidermal junction (DEJ): bridging of rete ridges, lamellar fibroplasia, lymphocytic infiltrate, and "shouldering" (junctional extension beyond the dermal component).
Management
- Mild-to-moderate dysplasia with clear margins: observation
- Severe dysplasia: complete excision with 2-5 mm margins
- DNS patients: regular full-body skin examinations, sun protection, education on ABCDE criteria
4. Lentigo Maligna (Melanoma In Situ on Photodamaged Skin)
- Presents as a slowly growing, irregular, tan-to-brown hyperpigmented patch on the face of elderly patients (most common on the cheek/nose)
- Is the in situ form of lentigo maligna melanoma (LMM)
- May involve large areas making simple excision difficult
- Treatment: Surgical excision with 5-10 mm margins; radiotherapy (35-100 Gy in 5-10 large fractions; or 40-50 Gy in 10-20 fractions) is a well-established alternative with 5-year cure rates of 90-95%, especially in elderly patients where size/location prohibits excision - Dermatology 2-Volume Set 5e
5. Leukoplakia and Erythroplakia (Oral/Mucocutaneous)
Leukoplakia
Defined by WHO as "a white patch or plaque that cannot be scraped off and cannot be characterized clinically or pathologically as any other disease." Applied only to lesions of no known etiology.
- Affects ~3% of the world's population
- 5-25% of lesions are premalignant
- All leukoplakias must be considered precancerous until proven otherwise by histology
- Risk factors: tobacco (all forms), alcohol, HPV infection
- Histology ranges from simple hyperkeratosis with acanthosis to severe dysplasia and carcinoma in situ
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Erythroplakia
- A red, velvety, possibly eroded area in the oral cavity, level with or slightly depressed relative to surrounding mucosa
- Much less common than leukoplakia but far more ominous
- Histology: approximately 90% show severe dysplasia, carcinoma in situ, or minimally invasive carcinoma
- Intermediate form: Speckled erythroplakia (mixed red-white)
Both are most common in persons aged 40-70 years, with a 2:1 male preponderance.
6. Other Notable Premalignant Conditions
| Condition | Cancer Risk | Notes |
|---|---|---|
| Radiation dermatitis (chronic) | SCC | Develops years after therapeutic radiation |
| Burn scars (Marjolin's ulcer) | SCC (aggressive) | Can metastasize in up to 30% |
| Arsenical keratoses | SCC, BCC | Chronic arsenic exposure; multiple palmoplantar keratoses |
| Xeroderma pigmentosum | SCC, BCC, melanoma | Autosomal recessive; defective nucleotide excision repair |
| Giant congenital melanocytic nevus | Melanoma | Lifetime risk ~5-10%; neurocutaneous melanosis risk |
| Lichen sclerosus (anogenital) | SCC | ~4-6% malignant transformation |
| Human papillomavirus (HPV) lesions | SCC | HPV-16, 18 in genital lesions; acitretin can reduce development |
Summary Table
| Lesion | Precursor to | Malignant Transformation Risk | First-Line Treatment |
|---|---|---|---|
| Actinic keratosis | Cutaneous SCC | 0.1%/lesion/year | Cryotherapy (single) or 5-FU/imiquimod (field) |
| Bowen's disease | Invasive SCC | <5% (cutaneous); 10-30% (genital) | 5-FU, PDT, excision |
| Dysplastic nevus | Melanoma | Variable; near 100% lifetime in FAMM | Excision (severe); surveillance |
| Lentigo maligna | Lentigo maligna melanoma | High if untreated | Wide excision or radiotherapy |
| Leukoplakia | Oral SCC | 5-25% | Remove irritants, biopsy, ablation |
| Erythroplakia | Oral SCC | ~90% (severe dysplasia or CIS) | Biopsy + aggressive ablation/excision |
Recent evidence update: A 2026 systematic review and meta-analysis (PMID: 41578002) confirmed both PDT and imiquimod as effective field-directed treatments for AK with comparable outcomes. For hypertrophic AK and Bowen's disease, topical calcipotriol combined with 5-FU shows promising activity in a 2024 systematic review.
Sources: Dermatology 2-Volume Set 5e (Bolognia et al.), Andrews' Diseases of the Skin, Robbins & Cotran Pathologic Basis of Disease, Textbook of Family Medicine 9e, Fitzpatrick's Dermatology
Granulomatous lesions of skin
Finding Sources
Finding Sources
Searching PubMed
granulomatous skin disease
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Granulomatous Lesions of the Skin
A granuloma is a focal aggregate of activated macrophages (epithelioid histiocytes), often with multinucleated giant cells, lymphocytes, and plasma cells. Granulomatous skin lesions are classified broadly by aetiology into infectious, non-infectious inflammatory, and foreign body types.
Classification Overview
| Category | Examples |
|---|---|
| Infectious | Tuberculosis (cutis), Leprosy, Deep fungal infections, Leishmaniasis |
| Non-infectious inflammatory | Sarcoidosis, Granuloma annulare, Necrobiosis lipoidica, Rheumatoid nodule |
| Foreign body | Silica, suture, keratin, tattoo pigment, beryllium |
| Vasculitic/eosinophilic | Granulomatosis with polyangiitis (Wegener), Eosinophilic granulomatosis with polyangiitis |
1. Granuloma Annulare (GA)
Overview
A relatively common, idiopathic disorder of the dermis and subcutaneous tissue. Affects all ages and races; women are affected twice as often as men. Most cases spontaneously resolve leaving entirely normal skin, though loss of elastic tissue may occur in some.
Histology
- Palisading granuloma: epithelioid histiocytes arranged in a palisade around a central zone of degenerated collagen and increased mucin (distinguishes it from necrobiosis lipoidica)
- Interstitial pattern: scattered histiocytes between collagen bundles without true palisading
Clinical Variants
A. Localized GA (most common)
- Tends to affect children and young-to-middle-aged adults
- One or a few lesions on lateral/dorsal fingers, hands, dorsal feet, elbows, or ankles
- Erythematous to violaceous, thinly bordered plaques or papules that spread peripherally while undergoing central involution - forming annular (ring-shaped) lesions
- Overlying skin remains normal; lesions never ulcerate
-
50% clear within 2 years; recur in 40%
- Association with autoimmune thyroiditis in women
B. Generalized GA
- Affects mostly women in the fifth and sixth decades, also adolescents
- Hundreds of lesions; symmetric papular or annular eruption favoring the nape of neck, upper trunk, proximal extremities; face, genitals spared
- Associated with diabetes mellitus and dyslipidemia (elevated cholesterol, triglycerides, LDL)
C. Subcutaneous (deep) GA
- Predominantly in children under 6 years
- Firm, skin-colored to pink nodules, often on the scalp, lower legs, hands, buttocks
D. Perforating GA
- Rare; central umbilication with elimination of altered dermal material through the epidermis
- May occur on fingers, hands, and trunk
Associations & Triggers
- Koebner (isomorphic) response
- Can occur in healed herpes zoster areas
- Drug-induced GA: allopurinol, gold, diclofenac, calcium channel blockers, biologics
- Sun-exposed areas (actinic granuloma - O'Brien variant)
Management
Many lesions resolve spontaneously. Treatment options include:
- Intralesional triamcinolone - for localized disease
- Potent topical corticosteroids ± occlusion
- Cryotherapy
- Generalized: hydroxychloroquine, dapsone, isotretinoin, PUVA, narrowband UVB, cyclosporine, biologics (TNF inhibitors, JAK inhibitors)
- Andrews' Diseases of the Skin, p. 978-994; Dermatology 2-Volume Set 5e
2. Necrobiosis Lipoidica (NL)
Coined by Urbach in 1932 as "necrobiosis lipoidica diabeticorum." The shortened term NL is preferred because not all patients have diabetes.
Epidemiology
- Mean age of onset: ~30 years; women 3:1 over men
- 60% occur in type 1 (insulin-dependent) diabetic patients; 20% in pre-diabetic individuals
- NL precedes diabetes by ~2 years in 15% of cases
- Prevalence of NL in diabetics: only 0.3-3% (uncommon marker despite strong association)
- Diabetes control does not correlate with disease activity
Clinical Features
- Classically on the anterior pretibial shins (bilateral); also ankles, calves, thighs, feet
- Early: small, sharply bordered red-brown papules with slight scale
- Established: well-defined oval/round plaques with depressed, waxy, sulfur-yellow center with prominent telangiectasias ("glazed porcelain" appearance) and a raised violaceous border
- Ulceration occurs in 13-35% of cases on the legs - the most serious complication
- Rare: squamous cell carcinoma arising in chronic ulcers
- Overlapping associations with GA and sarcoidosis

Histology
- At low magnification: layered palisaded granulomas with pale-pink degenerated collagen alternating with amphophilic-staining histiocytes - involving the full thickness of the reticular dermis and often panniculus
- Key distinguishing features from GA:
- No increased mucin in centers of granulomas
- No normal dermis between granulomas (in GA, intervening collagen is relatively normal)
- Thinned overlying epidermis with loss of rete ridges
- Plasma cells prominent
- Punch biopsy specimens appear rectangular (not tapered) due to dermal firmness
Management
Treatment is often disappointing:
- Potent topical glucocorticoids - may slow early progression
- Intralesional triamcinolone to active border (risk of ulceration)
- Short-term systemic glucocorticoids for active disease
- Aspirin + dipyridamole (variable results)
- Wound care for ulcerated lesions
- Tacrolimus, thalidomide, ciclosporin, anti-TNF agents reported in case series
- Fitzpatrick's Dermatology, p. 2530; Andrews' Diseases of the Skin, p. 623
3. Sarcoidosis (Cutaneous)
Cutaneous sarcoidosis occurs in 20-30% of patients with systemic sarcoidosis; more common and severe in Black patients.
Pathogenesis
The triggering antigen is uncertain. Proposed mechanisms:
- Autoimmune etiology
- Inorganic dusts/particles (zirconium, talc, beryllium)
- Infectious triggers: mycobacterial DNA sequences identified in ~25% of sarcoidal tissues; M. tuberculosis catalase-peroxidase (mKatG) protein proposed as a triggering antigen
- Transmissibility via Kveim reagent; sarcoidal granulomas in organ recipients from donors with sarcoidosis
- JAK/STAT pathway activation - basis for emerging JAK inhibitor therapy
Histology
- Naked (sarcoidal) granulomas: tight clusters of epithelioid histiocytes and multinucleated giant cells with minimal or absent surrounding lymphocytic infiltrate ("naked" appearance)
- Schaumann bodies (calcified concentric lamellated inclusions) and asteroid bodies in giant cells
- No caseation necrosis (unlike tuberculosis)
Spectrum of Cutaneous Manifestations
Specific (granulomatous) lesions:
| Type | Features |
|---|---|
| Papules | Flesh-colored to red-brown; favor periorificial sites on face |
| Lupus pernio | Disfiguring violaceous plaques and nodules on nose, nasal alae, malar areas, periorbital - most specific marker of chronic systemic disease |
| Plaques | Brownish-red, indurated; favor trunk and extremities |
| Scar sarcoidosis | Infiltration of old scars or tattoos (especially red/yellow pigments) weeks to decades after initial injury |
| Subcutaneous (Darier-Roussy) | Firm, mobile nodules on extremities |
| Annular/lichenoid/atrophic | Less common variants |
| Alopecia | Scarring or nonscarring |
Non-specific lesion:
- Erythema nodosum - non-granulomatous panniculitis; seen in acute (Lofgren syndrome) sarcoidosis; generally indicates good prognosis
Lofgren Syndrome
Acute sarcoidosis triad: erythema nodosum + bilateral hilar adenopathy + polyarthritis/periarthritis. Generally self-limiting with good prognosis.
Management of Cutaneous Sarcoidosis
- Topical/intralesional corticosteroids - first-line for localized disease
- Hydroxychloroquine - effective for cutaneous and hypercalcemia
- Methotrexate - for refractory/widespread disease
- TNF inhibitors (adalimumab, infliximab) - for lupus pernio and refractory disease
- JAK inhibitors - topical ruxolitinib and oral agents emerging as options (recent 2025 systematic review PMID: 40192197)
- Dermatology 2-Volume Set 5e; Fishman's Pulmonary Diseases and Disorders
4. Cutaneous Tuberculosis
No ideal classification exists, but the following system is based on mechanism of acquisition:
Categories Based on Route of Infection
A. Inoculation from Exogenous Source (High Bacillary Load)
| Disease | Features |
|---|---|
| Primary inoculation TB (Tuberculous chancre) | Children; face/extremities; 2-4 weeks after inoculation - painless indurated papule → nodule or ulcer + regional lymphadenopathy (primary complex); heals spontaneously in ~1 year |
| TB verrucosa cutis | Exogenous inoculation in a previously sensitized person (strong immunity, strongly positive tuberculin test); dorsa of fingers/hands in adults, ankles/buttocks in children; begins as small papule → hyperkeratotic warty plaque with peripheral expansion, sometimes central clearing; "Prosecutor's wart" |
B. Endogenous Spread
| Disease | Features |
|---|---|
| Scrofuloderma | Contiguous spread from underlying infected lymph node or bone; most common on neck, axilla, groin; begins as firm subcutaneous nodule → softens → cold abscess → ulceration with undermined bluish edges and sinuses |
| TB cutis orificialis | Autoinoculation of mucous membranes/orifices in patients with cavitary pulmonary or GI TB; painful ulcers around mouth, nostrils, anus |
C. Hematogenous Spread
| Disease | Features |
|---|---|
| Lupus vulgaris | Most common form in high-immunity individuals; "apple jelly" nodules on diascopy (soft, translucent, yellow-brown nodules); face/head/neck; slowly progressive plaques with scarring; risk of SCC in chronic lesions |
| Acute miliary TB | Least effective host immunity; widespread tiny papules, vesicles, or purpura; in immunocompromised |
| TB gumma/abscess | Hematogenous; fluctuant subcutaneous abscesses that ulcerate |
D. Tuberculids (hypersensitivity reactions - high immunity, organisms rarely found)
| Disease | Features |
|---|---|
| Erythema induratum (Bazin disease) | Recurring nodules on posterior calves in middle-aged women → ulcerate → heal with scarring; PCR positive for M. tuberculosis DNA |
| Papulonecrotic tuberculid | Bilateral symmetric necrotic papules on extensor extremities; heal with varioliform scars |
| Lichen scrofulosorum | Grouped lichenoid papules on trunk in children with TB of lymph nodes or bone |
Diagnosis
- PPD (tuberculin skin test) / IGRA: positive in paucibacillary forms (lupus vulgaris, TB verrucosa cutis)
- AFB smear + culture (gold standard; positive mainly in multibacillary forms)
- PCR for mycobacterial DNA - detects even in tuberculids
- Histology: caseating granulomas in most forms
Treatment
Standard anti-TB regimen: 2 months HRZE + 4 months HR (isoniazid, rifampicin, pyrazinamide, ethambutol)
5. Leprosy (Hansen's Disease)
Caused by Mycobacterium leprae. Cutaneous granulomas vary with host immunity:
| Type | Immunity | Granuloma | Bacilli | Clinical |
|---|---|---|---|---|
| Tuberculoid (TT) | High | Well-formed epithelioid, with lymphocytic cuffing; nerves destroyed | Absent (paucibacillary) | Few well-defined hypopigmented anesthetic plaques; enlarged peripheral nerves |
| Lepromatous (LL) | Low/absent | Poorly formed, "foamy" (Virchow cells - lipid-laden macrophages); no lymphocytes | Numerous (multibacillary) | Diffuse infiltration; leonine facies, madarosis; nodules (lepromas) |
| Borderline (BT, BB, BL) | Intermediate | Variable | Variable | Unstable; liable to reactions |
Reactions:
- Type 1 (reversal): sudden upgrading of cell-mediated immunity; acute inflammation in existing lesions
- Type 2 (ENL - erythema nodosum leprosum): immune complex-mediated; in BL/LL; tender erythematous nodules + systemic features
6. Foreign Body Granulomas
Occur in response to endogenous or exogenous materials that resist degradation:
| Stimulus | Notes |
|---|---|
| Suture/surgical material | Epithelioid granulomas around suture fragments |
| Silica | Sarcoidal-pattern granulomas; often decades after exposure |
| Tattoo pigments (red/yellow) | Mercury sulfide (red), cadmium sulfide (yellow) - most reactive |
| Keratin (from ruptured cyst) | Xanthogranulomatous or suppurative pattern |
| Paraffin/silicone | Sclerosing lipogranuloma |
| Zirconium | Epithelioid granulomas in axillary skin from deodorants |
| Beryllium | Clinically and histologically indistinguishable from sarcoidosis |
Histology: Polarizable foreign material within giant cells; mixed inflammatory infiltrate; often suppurative component with neutrophils in addition to granuloma.
Key Histologic Comparisons
| Feature | Granuloma Annulare | Necrobiosis Lipoidica | Sarcoidosis | TB |
|---|---|---|---|---|
| Granuloma type | Palisading (incomplete) | Palisading (layered, full thickness) | Naked (tight, no lymphocytes) | Caseating |
| Central material | Mucin + degenerated collagen | Degenerated collagen (no mucin) | None | Caseous necrosis |
| Dermis affected | Upper/mid dermis | Full reticular dermis + panniculus | Variable | Variable |
| Organisms | Absent | Absent | Absent | Present (variable) |
| Epidermis | Normal | Thinned, rete ridges lost | Normal | Variable |
Sources: Andrews' Diseases of the Skin (Clinical Dermatology); Dermatology 2-Volume Set 5e (Bolognia et al.); Fitzpatrick's Dermatology 9e; Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.