Explain cataract for long question exam oriented according to ak khurana
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Kanski's Clinical Ophthalmology (the definitive systematic ophthalmology reference, equivalent in standard and organization to AK Khurana). I have enough material to write a thorough long-answer exam response. Let me now compose the full answer.
CATARACT
Based on AK Khurana / Kanski's Clinical Ophthalmology - Exam Oriented Long Answer
DEFINITION
Cataract is any opacity of the crystalline lens or its capsule. It is the commonest cause of reversible visual disability in the world, and phacoemulsification with intraocular lens (IOL) implantation is the most commonly performed surgical procedure globally. There is currently no medical treatment proven to prevent or reverse cataract formation.
ANATOMY OF THE LENS (Relevant to Cataract)
- Zonules suspend the lens in position.
- Capsule: an acellular membrane enclosing the entire lens.
- Epithelium: cuboid cells beneath the anterior capsule, extending to the equator. Cells in the germinative zone divide continuously and differentiate into lens fibres.
- Lens substance: central nucleus surrounded by cortex.
- The lens has no blood supply - it depends entirely on the aqueous humour for nutrition.
CLASSIFICATION OF CATARACT
A. Based on Aetiology
- Age-related (senile)
- Congenital
- Traumatic
- Secondary (complicated)
- Cataract in systemic disease
- Drug-induced (e.g., steroids, chlorpromazine)
- Radiation-induced
B. Based on Morphology
- Subcapsular (anterior / posterior)
- Nuclear
- Cortical
- Christmas tree
C. Based on Maturity (Senile Cataract)
- Immature
- Mature
- Hypermature
- Morgagnian
SYMPTOMS OF CATARACT
- Reduced visual acuity (initially correctable with glasses)
- Loss of contrast sensitivity
- Change in colour perception - particularly impaired perception of blue colours
- Glare - due to light scattering; worsened at night (headlight glare during driving)
- Monocular diplopia - especially on looking at point sources of light
- Difficulty in dim light / poor night vision
- Myopic shift (in nuclear cataract) - patient may be able to read without glasses again ("second sight of the aged")
AGE-RELATED (SENILE) CATARACT
1. Posterior Subcapsular Cataract (PSC)
- Located just anterior to the posterior capsule
- Granular or plaque-like appearance on oblique slit-lamp biomicroscopy
- Appears black and vacuolated on retroillumination; vacuoles = swollen Wedl cells (bladder cells = migratory lens epithelial cells)
- Due to its position at the nodal point of the eye, PSC causes profound visual impairment disproportionate to its size
- Symptoms: glare (worsened by miosis - e.g., in bright sunlight or near vision)
2. Anterior Subcapsular Cataract
- Lies directly under the lens capsule
- Associated with fibrous metaplasia of the lens epithelium
3. Nuclear Sclerotic Cataract
- An exaggeration of normal ageing
- Myopic shift due to increased refractive index of nucleus → "second sight of the aged"
- Yellowish hue due to deposition of urochrome pigment → may turn brown (brunescent), rarely black
- Best assessed with oblique slit-lamp beam
- On retroillumination: good red reflex but subtle nucleus-cortex demarcation
4. Cortical Cataract
- Involves anterior, posterior, or equatorial cortex
- Opacities start as clefts and vacuoles due to cortical hydration
- Results in typical cuneiform (wedge-shaped) or spoke-like radial opacities
- Often starts in the inferonasal quadrant
- Glare is a common symptom
5. Christmas Tree Cataract
- Polychromatic (multicoloured) needle-like deposits in the deep cortex/nucleus
- Associated with myotonic dystrophy (though can occur in others)
- Characteristic sparkling, multicoloured sheen on slit-lamp examination
STAGES OF SENILE CATARACT (Maturity)
| Stage | Features |
|---|---|
| Immature | Lens partially opaque; some cortex still clear |
| Mature | Lens completely opaque; fundus glow absent |
| Hypermature | Shrunken, wrinkled anterior capsule due to water leakage out of lens |
| Morgagnian | Hypermature cataract with liquefied cortex; nucleus sinks inferiorly due to gravity |
Exam note: Hypermature cataracts can leak lens proteins causing phacolytic glaucoma (macrophages clog trabecular meshwork). Morgagnian cataracts can cause phacomorphic glaucoma by pupillary block.
SLIT-LAMP APPEARANCE
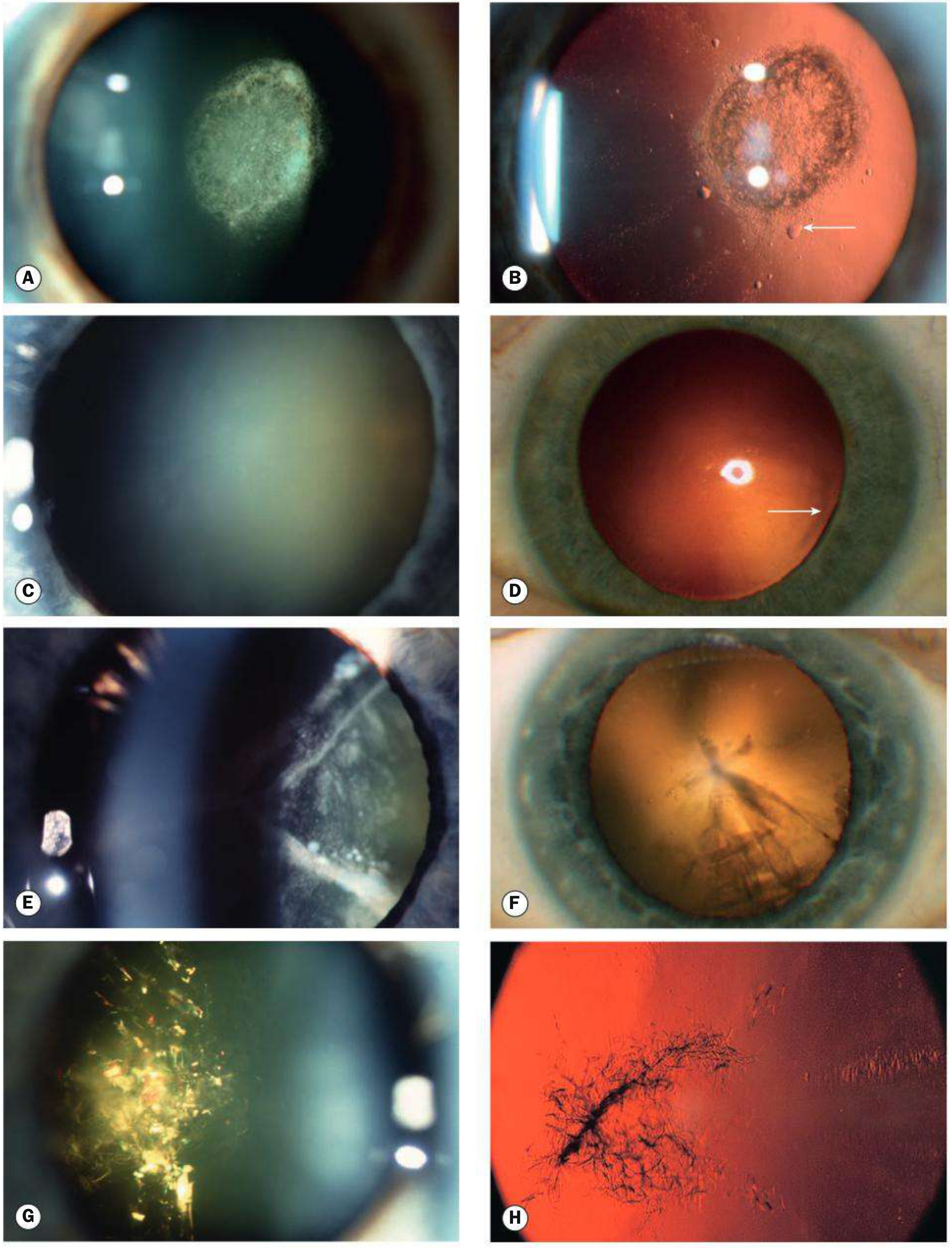
Fig: Age-related cataract types (Kanski's Clinical Ophthalmology)
CATARACT IN SYSTEMIC DISEASE
1. Diabetes Mellitus
- Hyperglycaemia → high aqueous glucose → glucose diffuses into lens → metabolized to sorbitol → osmotic overhydration of lens
- Early: refractive fluctuation (hyperglycaemia → myopia; hypoglycaemia → hypermetropia)
- Classic diabetic cataract (rare, in young): snowflake cortical opacities - may mature within days or resolve spontaneously
- Age-related cataract occurs earlier in diabetics
- Nuclear sclerosis is common and progresses rapidly
- ~1 in 5 cataract surgery patients has diabetes
2. Myotonic Dystrophy
- ~90% develop fine iridescent cortical opacities in the 3rd decade (sometimes like Christmas tree cataract)
- Progress to visually disabling star-shaped wedge-shaped cortical + subcapsular opacities by the 5th decade
3. Atopic Dermatitis
- ~10% of severe cases develop cataracts in the 2nd-4th decades
- Characteristic: shield-like dense anterior subcapsular plaque wrinkling the anterior capsule
- Posterior subcapsular opacities may also occur
4. Neurofibromatosis Type 2
- Early cataract in >60% of patients
- Opacities: posterior subcapsular, capsular, cortical, or mixed
- Tend to develop in early adulthood
5. Steroid-induced
- Prolonged topical/systemic/inhaled corticosteroids → posterior subcapsular cataract
6. Wilson's Disease
- Sunflower cataract - greenish-brown pigment deposits in anterior lens capsule (due to copper deposition)
SECONDARY (COMPLICATED) CATARACT
A secondary cataract develops due to a primary ocular disease:
| Primary Disease | Cataract Features |
|---|---|
| Chronic anterior uveitis | Most common cause; polychromatic lustre at posterior pole → anterior and posterior opacities; steroids used in treatment are also causative |
| Acute congestive angle closure | Glaukomflecken - small grey-white anterior subcapsular opacities; represent focal lens epithelial infarcts; pathognomonic of previous acute ACG |
| High myopia | Posterior subcapsular opacity + early nuclear sclerosis |
| Retinitis pigmentosa | Posterior subcapsular cataract |
| Absolute glaucoma | Anterior subcapsular or total cataract |
TRAUMATIC CATARACT
| Cause | Cataract Features |
|---|---|
| Penetrating trauma | Rupture of lens capsule → rapid opacification |
| Blunt trauma | Characteristic flower-shaped (rosette) opacity |
| Electric shock / lightning | Diffuse milky-white opacification or multiple snowflake-like or stellate subcapsular opacities |
| Infrared radiation (glassblowers) | True exfoliation of anterior lens capsule ("glassblower's cataract") |
| Ionizing radiation | Posterior subcapsular opacities; may not manifest for months-years |
| Intralenticular foreign body | Siderosis lentis (iron), chalcosis (copper) |
CONGENITAL CATARACT
Epidemiology
- Occurs in ~3 in 10,000 live births
- 2/3 are bilateral; 1/3 are unilateral (usually sporadic)
- Aetiology: 1/3 systemic disease; 1/3 inherited; 1/3 unknown cause
- Autosomal dominant (AD) is the most common inheritance pattern
Associated Metabolic Disorders
| Disorder | Cataract Type | Key Features |
|---|---|---|
| Galactosaemia (AR - GALT enzyme deficiency) | "Oil droplet" opacity | Within first weeks of life; exclusion of galactose may reverse early changes |
| Lowe syndrome (X-linked recessive - OCRL1 gene) | Universal, dense | Oculo-cerebro-renal; congenital glaucoma in ~50%; female carriers may have cortical opacities |
| Mannosidosis (AR - α-mannosidase deficiency) | Spoke-like posterior cortical opacities | Progressive mental deterioration |
| Hypo/pseudohypoparathyroidism | Various | Hypocalcaemia-related |
Associated Intrauterine Infections (TORCH)
| Infection | Cataract Features |
|---|---|
| Rubella | Pearly nuclear or diffuse cataract; ~15% of congenital rubella; live virus may be present in the lens for years post-delivery |
| Toxoplasmosis | Cataract + chorioretinitis + microphthalmos |
| Cytomegalovirus (CMV) | Various ocular features |
| Herpes simplex/Varicella | Lens opacities possible |
Morphological Types of Congenital Cataract
| Type | Description |
|---|---|
| Polar (anterior/posterior) | Localized at poles; often stationary; good prognosis |
| Nuclear | Involves embryonic/fetal nucleus; AD; often stationary |
| Lamellar (zonular) | Most common type requiring surgery; involves specific zone; AD |
| Sutural | Y-suture opacities; usually benign |
| Coronary | Club-shaped opacities at lens periphery |
| Cerulean (blue-dot) | Blue punctate opacities; AD; rarely visually significant |
| Total | Complete lens opacification; worst prognosis for vision |
| Oil droplet | Galactosaemia-specific |
MANAGEMENT OF CATARACT
Indications for Surgery
- Visual: when cataract causes sufficient visual disability (functional indications)
- Medical: phacolytic glaucoma, phacomorphic glaucoma, subluxated lens causing uveitis
- Social: to allow fundus examination (e.g., diabetic retinopathy monitoring)
- Congenital: dense unilateral/bilateral cataract - surgery urgently needed to prevent amblyopia
Preoperative Assessment
General medical:
- Diabetes - optimize glycaemic control
- Hypertension - defer if systolic >170 mmHg / diastolic >100 mmHg
- Anticoagulants (e.g., warfarin, aspirin) - consider stopping based on risk
- Alpha-blockers (e.g., tamsulosin) - major cause of Intraoperative Floppy Iris Syndrome (IFIS)
Ophthalmic assessment:
- Visual acuity (Snellen chart)
- Cover test (rule out amblyopia/squint)
- Pupillary responses (cataract never causes RAPD - its presence implies posterior segment pathology)
- Slit-lamp examination (cornea, AC depth, pupil dilation, lens type)
- Fundal examination (macular pathology, retinal detachment)
- Biometry - IOL power calculation (using A-scan ultrasound or optical biometry)
Anaesthesia Options
- Topical (most common for routine phacoemulsification)
- Sub-Tenon's/peribulbar/retrobulbar (regional)
- General anaesthesia (in children, uncooperative patients)
SURGICAL TECHNIQUES
1. Intracapsular Cataract Extraction (ICCE) - Historical
- Entire lens including capsule removed through a large incision
- Now largely abandoned
- Complications: vitreous loss, aphakia, bullous keratopathy
2. Extracapsular Cataract Extraction (ECCE)
- Nucleus expressed through a large (~10-12 mm) limbal incision; posterior capsule left intact
- IOL implanted in the capsular bag
- Still used for very hard (brunescent/black) nuclei
3. Manual Small-Incision Cataract Surgery (MSICS)
- Scleral tunnel incision (~6-7 mm) - self-sealing
- Nucleus expressed through the tunnel without phacoemulsification
- Widely used in developing countries (cost-effective)
- Technique: scleral tunnel → anterior capsulotomy (can-opener or manual CCC) → nucleus expression → cortical aspiration (Simcoe cannula) → IOL implantation
4. Phacoemulsification (Gold Standard)
Principle: Ultrasonic vibration of a hollow titanium needle breaks the lens nucleus into small pieces (emulsification), which are then aspirated.
Incision: Clear corneal incision - typically 2.2-2.8 mm (microincision phaco) - self-sealing, sutureless.
Steps of Phacoemulsification:
- Corneal/scleral incision (main port + side port)
- Injection of OVD (ophthalmic viscosurgical device/viscoelastic) to maintain AC
- Continuous Curvilinear Capsulorhexis (CCC) - circular tear of anterior capsule using bent needle/capsulorrhexis forceps
- Hydrodissection - BSS injected under capsule to free cortical-capsular adhesions
- Hydrodelineation - separates nucleus from epinucleus
- Phacoemulsification of nucleus (various techniques: divide-and-conquer, stop-and-chop, phaco-chop)
- Irrigation and aspiration (I&A) of cortical remnants
- IOL implantation into the capsular bag
- OVD removal and wound hydration/closure
Phaco machine components:
- Peristaltic pump: flow-controlled; vacuum builds only on occlusion; independent adjustment of flow rate (AFR)
- Venturi pump: vacuum-controlled; synchronized vacuum and AFR; no independent AFR adjustment
- Phaco handpiece with titanium needle + fluid-cooling sleeve
5. Femtosecond Laser-Assisted Cataract Surgery (FLACS)
- Laser performs: capsulotomy, nuclear fragmentation, and corneal incisions with high precision
- Advantages: reproducible capsulotomy, reduced phaco energy, astigmatism correction
- Limitations: cost, risk of incomplete capsulotomy
INTRAOCULAR LENSES (IOL)
Types
| Type | Description |
|---|---|
| Monofocal IOL | Single focus (distance); most common |
| Multifocal IOL | Distance + near focus; risk of dysphotopsia, halos |
| Toric IOL | Corrects pre-existing corneal astigmatism |
| Extended depth of focus (EDOF) | Elongated focal range |
| Accommodating IOL | Attempts to mimic accommodation |
IOL Power Calculation
- Optical biometry (IOLMaster) - preferred, non-contact
- A-scan ultrasound - contact/immersion
- Formulae: SRK/T (most widely used), Holladay, Hoffer Q, Barrett Universal II
IOL Placement
- In-the-bag (capsular bag): ideal position
- Ciliary sulcus: used if posterior capsule torn; requires 3-piece IOL (not 1-piece)
- Optic capture through capsulorhexis can be done for stabilization
COMPLICATIONS OF CATARACT SURGERY
Intraoperative
| Complication | Notes |
|---|---|
| Posterior capsule rupture (PCR) | Most feared; manage with vitrectomy; IOL in sulcus/ACIOL |
| Vitreous loss | Requires anterior vitrectomy |
| Zonular dialysis | Weak zonules in pseudoexfoliation, Marfan's |
| Suprachoroidal hemorrhage | Rare, devastating |
| IFIS (Intraoperative Floppy Iris Syndrome) | Due to alpha-1 blockers (tamsulosin); floppy iris, prolapse, miosis |
| Dropped nucleus | Nucleus falls into vitreous; requires vitreoretinal surgery |
Early Postoperative
| Complication | Notes |
|---|---|
| Endophthalmitis | Most serious; organisms: Staph. epidermidis (most common), Staph. aureus; treated with intravitreal antibiotics (vancomycin + ceftazidime) |
| Corneal decompensation | Bullous keratopathy |
| Elevated IOP | Retained OVD, hyphema |
| Wound leak | Seidel-positive |
| Uveitis | Toxic anterior segment syndrome (TASS) |
Late Postoperative
| Complication | Notes |
|---|---|
| Posterior Capsular Opacification (PCO) | Most common late complication; "after-cataract"; due to Elschnig pearl formation from residual lens epithelial cells (Wedl cells); treated by Nd:YAG laser posterior capsulotomy |
| Cystoid Macular Oedema (CMO) | Irvine-Gass syndrome; treat with topical NSAIDs, steroids, anti-VEGF |
| Retinal detachment | More common in high myopes |
| IOL dislocation/subluxation | Especially with weak zonules |
| Dysphotopsia | Positive (glare/halos) or negative (dark shadow in temporal periphery) |
| Capsulophimosis | Anterior capsule contraction; treat with Nd:YAG anterior capsulotomy |
POSTERIOR CAPSULAR OPACIFICATION (PCO) - AFTER-CATARACT
- Most common late complication of cataract surgery
- Occurs due to proliferation of residual lens epithelial cells (particularly Elschnig pearls = Wedl cells)
- Patient presents with gradual painless decrease in vision weeks to months after surgery
- Slit-lamp: pearl-like opacities on posterior capsule
- Treatment: Nd:YAG laser posterior capsulotomy
- Power: start at 1 mJ/pulse
- Pattern: cruciate or circumferential
- Opening size: ~4-5 mm (= dilated pupil size)
- Complications of YAG: IOP spike, IOL pitting, retinal detachment, CMO
CONGENITAL CATARACT - MANAGEMENT
Urgency
- Dense bilateral cataract: surgery within first 6-8 weeks of life to prevent deprivation amblyopia
- Dense unilateral cataract: surgery as soon as possible (ideally within first 6 weeks); more aggressive amblyopia treatment needed post-surgery
Surgical Technique in Children
- Posterior capsulectomy + anterior vitrectomy performed at time of primary surgery (posterior capsule opacifies rapidly in children)
- Primary IOL implantation controversial in children <2 years; contact lenses/aphakic glasses used instead
Post-surgical Management
- Optical rehabilitation: aphakic glasses / contact lenses / IOL
- Amblyopia treatment (patching of fellow eye) - critical for unilateral cataract
DRUGS CAUSING CATARACT (Drug-induced)
| Drug | Type of Cataract |
|---|---|
| Corticosteroids (systemic/topical) | Posterior subcapsular |
| Chlorpromazine | Anterior subcapsular stellate deposits |
| Amiodarone | Anterior subcapsular / axial |
| Gold salts (chrysiasis) | Anterior subcapsular |
| Busulfan | PSC |
| Allopurinol | PSC |
| Miotics (long-acting, e.g., phospholine iodide) | Anterior subcapsular |
KEY EXAM POINTS TO REMEMBER
- Cataract = commonest cause of reversible blindness worldwide
- PSC is most visually disabling relative to size (nodal point location)
- "Second sight of the aged" = nuclear cataract → myopic shift
- Morgagnian cataract = liquefied cortex + sunken nucleus (hypermature)
- Glaukomflecken = pathognomonic of previous acute ACG
- Oil droplet cataract = galactosaemia (treatable by diet!)
- Congenital rubella = pearly nuclear cataract; live virus in lens years after birth (beware during surgery)
- IFIS = caused by alpha-1 blockers (tamsulosin) - always take drug history
- After-cataract (PCO) = treated by Nd:YAG capsulotomy
- Endophthalmitis = most feared early post-op complication; intravitreal vancomycin + ceftazidime
- Phaco = phacoemulsification via ultrasonic vibration; self-sealing small incision; gold standard
- IOL power = calculated by optical biometry (IOLMaster); SRK/T formula most used
- Cataract NEVER causes RAPD - its presence implies significant posterior segment disease
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition | AK Khurana's Ophthalmology (comprehensive principles consistent with above)
This is a shared conversation. Sign in to Orris to start your own chat.