Urology disease there diagnosis treatment and clinical interpretation to know which diseas is likely seen
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive material from the textbooks. Let me compose the full, organized response.
Urological Diseases: Diagnosis, Treatment & Clinical Interpretation
Sources: Campbell-Walsh-Wein Urology (3-Vol Set), Smith & Tanagho's General Urology 19e, Bailey & Love's Short Practice of Surgery 28e, Robbins & Cotran Pathologic Basis of Disease, Textbook of Family Medicine 9e
Quick Clinical Orientation
The table below gives the rapid "which disease is this?" approach before the detailed sections.
| Presentation Clue | Most Likely Disease |
|---|---|
| Older man + hesitancy + weak stream + nocturia | BPH |
| Older man + firm nodule on DRE + elevated PSA | Prostate cancer |
| Painless hematuria (any age) | Bladder cancer until proven otherwise |
| Sudden severe flank pain radiating to groin + hematuria | Urolithiasis (renal/ureteral calculus) |
| Dysuria + frequency + fever + CVA tenderness | Urinary tract infection (pyelonephritis if fever) |
| Young male + painless testicular mass | Testicular cancer |
| Inability to void + suprapubic pain | Acute urinary retention |
| Recurrent UTIs + residual urine | Bladder outflow obstruction secondary to BPH |
1. Benign Prostatic Hyperplasia (BPH)
Epidemiology
- Occurs in men over 50; by age 60, 50% have histological BPH
- Most common cause of bladder outflow obstruction (BOO) in men >70 years
- Affects the transitional zone of the prostate (submucous glands)
Anatomy of BPH
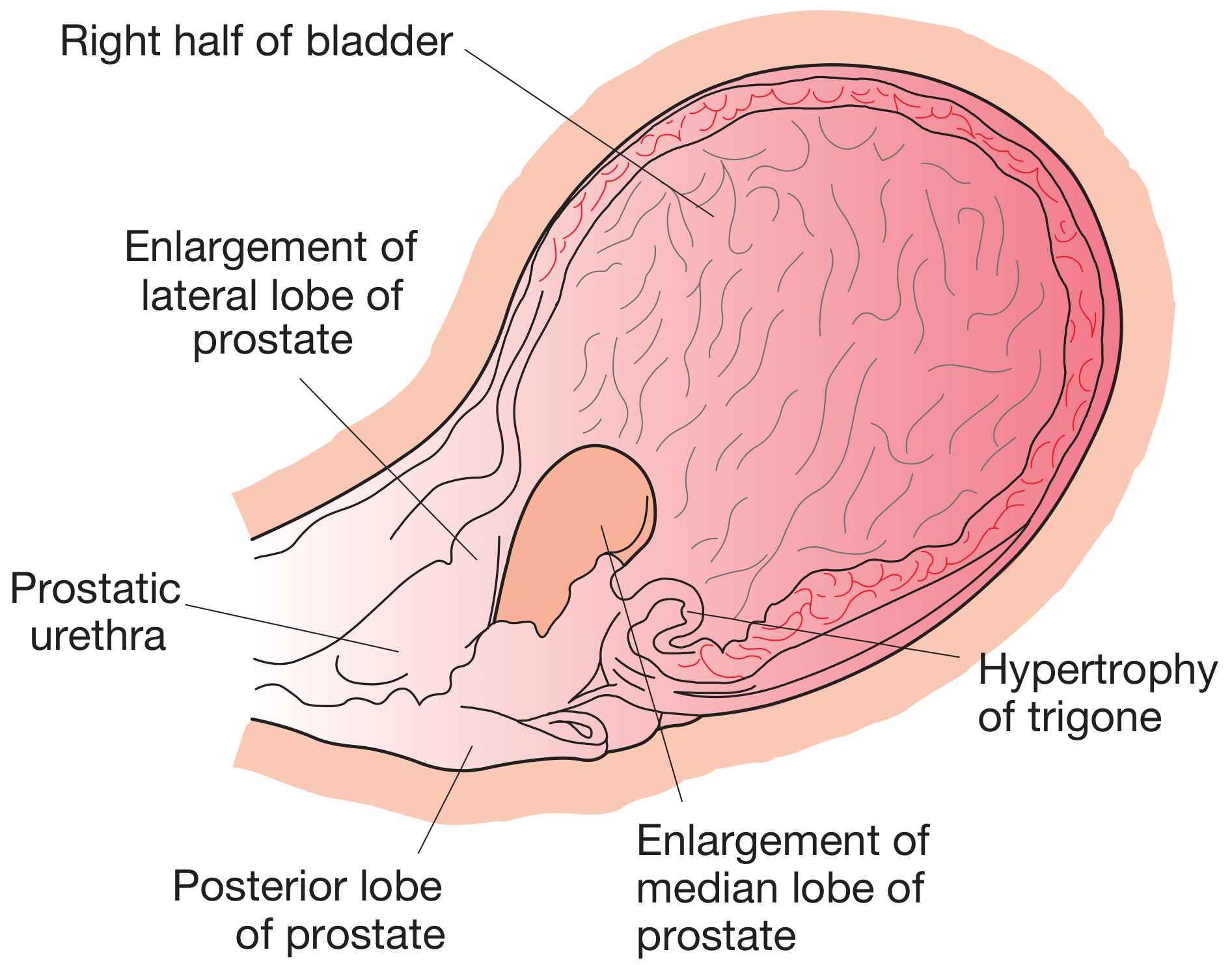
Fig. Diagram of late-stage bladder outflow obstruction showing BPH with lateral and median lobe enlargement, bladder trabeculation, and trigone hypertrophy. (Bailey & Love's Surgery 28e)
Clinical Features - LUTS
Voiding (obstructive) symptoms:
- Hesitancy (worsened when bladder is full)
- Poor urinary flow (not improved by straining)
- Intermittent stream (stops and starts)
- Terminal dribbling
- Sensation of incomplete bladder emptying
- Episodes of near retention
Storage (irritative) symptoms:
- Frequency
- Nocturia
- Urgency and urge incontinence
Complications of untreated BOO:
- Acute urinary retention (first symptom in some men)
- Chronic retention + hydronephrosis + renal impairment
- Bladder trabeculation and diverticula
- Urinary tract infections
- Bladder stones
- Recurrent hematuria (vascular prostate)
Diagnosis
Essential investigations:
- Urine dipstick (blood, leukocyte esterase, glucose, protein)
- Urine culture
- Serum creatinine (screen for renal impairment)
- Urinary flow rate + post-void residual (PVR) by ultrasound
- Normal peak flow: >15 mL/s (voided volume >200 mL)
- Equivocal: 10-15 mL/s
- Low (suggestive of BOO): <10 mL/s
- High voiding pressure: >80 cmH2O
Additional investigations:
- PSA (after counselling) - if free-to-total PSA <15% with PSA 4-10 ng/mL: suspicious for cancer; consider mpMRI
- Pressure-flow urodynamic studies (especially if: suspected neuropathy, dominant irritative symptoms, young/old men, post-surgical recurrence)
- TRUS-guided or transperineal biopsy if suspicious mpMRI lesion
- Upper tract imaging (IVU/CT urography/ultrasound) if hematuria or infection present
- Cystourethroscopy prior to prostatectomy to exclude stricture or bladder carcinoma
Treatment
Conservative (watchful waiting):
- Fluid manipulation (avoid binge drinking, late-night fluids)
- Reduce caffeine and alcohol
Drug therapy:
- Alpha-blockers (e.g., tamsulosin, alfuzosin) - relax smooth muscle, rapid symptom relief
- 5-alpha reductase inhibitors (e.g., finasteride, dutasteride) - for large glands, shrink prostate over months
- Combination therapy (alpha-blocker + 5-ARI) gives better outcomes in glands >35 g
Strong surgical indications:
- Acute retention in fit men with no reversible cause (25% of prostatectomies)
- Chronic retention + renal impairment + PVR >250 mL + hydronephrosis (15% of prostatectomies)
- Complications: stone, infection, diverticulum
- Recurrent hematuria from a vascular prostate
Surgical options:
- TURP (transurethral resection of the prostate) - gold standard
- HoLEP (holmium laser enucleation of the prostate) - for large glands
- Open/robotic simple prostatectomy - for very large glands
- Minimally invasive options: UroLift, Rezum, prostatic artery embolization
2. Prostate Cancer
Epidemiology
- Most common cancer diagnosed in men; second most common cause of cancer death in men (after lung cancer)
- Major risk factors: age >65, African American race, family history
- African Americans have 70% higher incidence than whites
- Most cases are indolent; symptoms arise late
Clinical Features
- Localized prostate cancer is asymptomatic - most often detected by PSA or DRE
- Clinically advanced disease: symptoms of urinary obstruction (mimics BPH)
- Firm, irregular nodule on Digital Rectal Examination (DRE) - but DRE sensitivity/specificity is low; predicts cancer in only 18-28% of cases
- Metastatic disease: bone pain (especially axial skeleton), weight loss, lymphadenopathy
Pathology
Histology (prostatic adenocarcinoma):
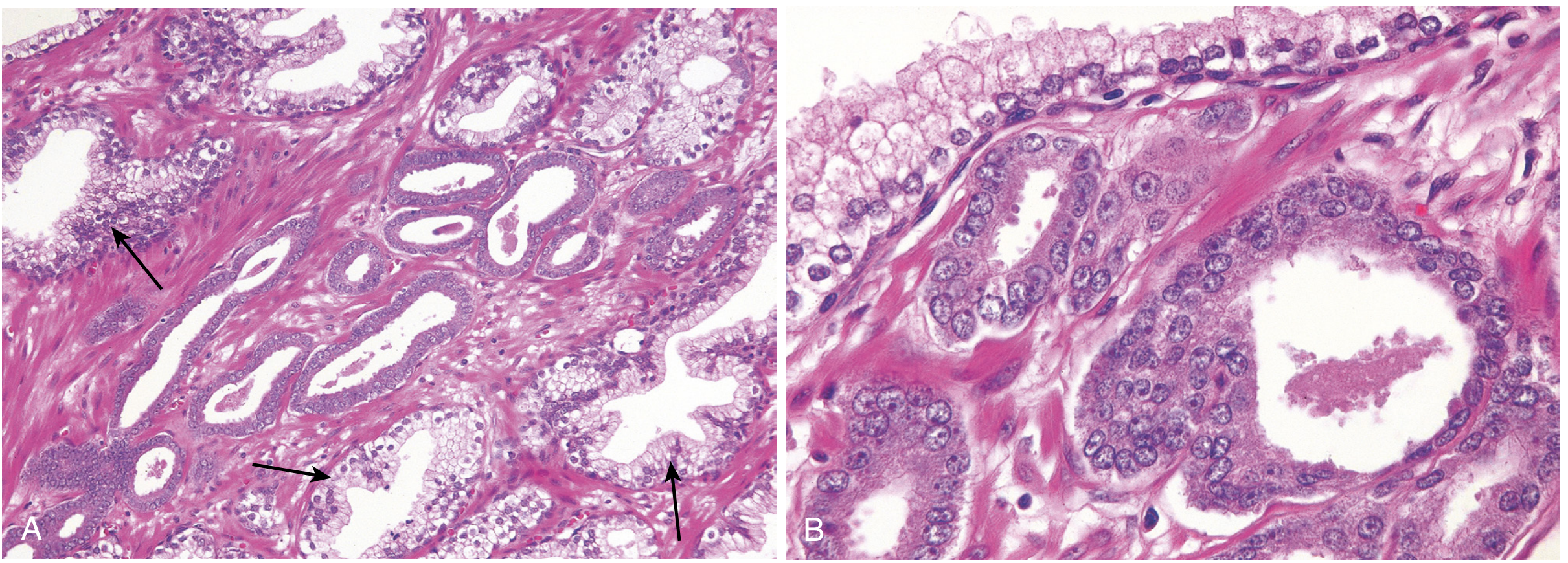
Fig. 21.34 Prostatic adenocarcinoma. (A) Small malignant glands crowded between larger benign glands. (B) Enlarged nuclei, prominent nucleoli, dark cytoplasm in malignant glands. (Robbins & Cotran)
Gleason Grading System:
| Grade Group | Gleason Score | Glandular Pattern |
|---|---|---|
| 1 | ≤6 (3+3) | Only individual discrete well-formed glands |
| 2 | 3+4 | Predominantly well-formed + lesser poorly-formed glands |
| 3 | 4+3 | Predominantly poorly formed + lesser well-formed |
| 4 | 4+4 / 3+5 / 5+3 | Only poorly formed/fused/cribriform glands |
| 5 | 4+5 / 5+4 / 5+5 | No gland formation; sheets of malignant cells |
Gleason scores 8-10 = advanced cancers, less likely to be cured.
pTNM Staging (AJCC 8th edition): Based on tumor extent (T), nodal spread (N), and distant metastasis (M).
Diagnosis
- PSA (Prostate-Specific Antigen): Widely used but controversial for screening. Clear value in monitoring recurrence after treatment
- PSA 4-10 ng/mL: indeterminate; free-to-total PSA <15% raises suspicion
- Rising PSA after treatment indicates recurrence
- mpMRI (multiparametric MRI): Identifies suspicious index lesions
- Transrectal needle biopsy (TRUS-guided or transperineal): Required to confirm diagnosis
Treatment
- Localized, low-risk (Grade Group 1): Active surveillance (serial PSA + mpMRI + biopsy)
- Localized, high-risk: Radical prostatectomy OR radiation therapy (external beam or brachytherapy), with or without hormonal manipulation (androgen deprivation therapy, ADT)
- >90% of patients with localized high-risk disease who receive surgery or radiation can expect to live 15 years
- Metastatic disease: ADT (LHRH agonists/antagonists ± anti-androgens); enzalutamide, abiraterone for castration-resistant prostate cancer (CRPC); chemotherapy (docetaxel) for high-volume metastatic disease
3. Bladder Cancer
Epidemiology
- Incidence increases with age; 4x more common in men than women; white men have 2x higher incidence than African Americans
- Cigarette smoking is the most prominent risk factor (4-7x increased risk)
- Other risk factors: aromatic amines (dye/rubber industry), benzidine, cyclophosphamide, pelvic radiation, chronic catheterization, aristolochic acid
Clinical Features
- Painless hematuria (gross or microscopic) = most common presenting sign
- Irritative LUTS (frequency, urgency) - especially with carcinoma in situ (CIS)
- Advanced disease: flank pain (ureteric obstruction), pelvic pain
Pathology
- 75-85% are superficial (non-muscle-invasive) at diagnosis: stages pTa, pT1, carcinoma in situ
- Remainder are muscle-invasive (pT2+) or metastatic at presentation
- Histology: predominantly transitional cell (urothelial) carcinoma; squamous cell and adenocarcinoma are less common
Diagnosis
- Cystoscopy + biopsy - gold standard for diagnosis and staging
- Urine cytology - high specificity; false negatives limit sensitivity
- No imaging test reliably detects all bladder cancers, but CT urography evaluates upper tracts and extent of disease
Treatment
Non-muscle-invasive bladder cancer (NMIBC):
- Transurethral resection of bladder tumor (TURBT)
- Intravesical BCG (Bacillus Calmette-Guerin) therapy - reduces recurrence and progression for high-risk NMIBC
- Intravesical chemotherapy (mitomycin C) - for low-to-intermediate risk
Muscle-invasive bladder cancer (MIBC):
- Radical cystectomy (gold standard) + urinary diversion; robotic-assisted cystectomy increasingly used
- Neoadjuvant cisplatin-based chemotherapy before cystectomy improves survival
- Bladder-preserving trimodality therapy (TURBT + chemotherapy + radiation) for selected patients
Metastatic:
- Cisplatin-based chemotherapy (gemcitabine + cisplatin)
- Immune checkpoint inhibitors (atezolizumab, pembrolizumab) for platinum-ineligible patients or second-line
4. Urinary Tract Infection (UTI) and Pyelonephritis
Classification
- Lower UTI: Cystitis (bladder), urethritis
- Upper UTI: Pyelonephritis (kidney parenchyma), urosepsis
Clinical Features
| Feature | Lower UTI (Cystitis) | Upper UTI (Pyelonephritis) |
|---|---|---|
| Dysuria | Yes | Yes |
| Frequency/urgency | Yes | Yes |
| Suprapubic pain | Yes | Less prominent |
| Fever/chills | No | Yes (often high fever) |
| CVA tenderness | No | Yes (costovertebral angle) |
| Nausea/vomiting | No | Common |
| Systemic toxicity | No | Yes |
Special context - surgical patients: The AUA guidelines require eradication of UTI before urologic endoscopic surgery. Preoperative UTI (especially recurrent) is a high-risk factor for postoperative infection. If sterilization is impossible (e.g., infected stones, indwelling catheter), perioperative culture to guide antibiotic choice.
Diagnosis
- Urinalysis (dipstick): leukocyte esterase, nitrites, blood
- Urine microscopy: pyuria (>5 WBC/hpf), bacteriuria
- Urine culture + sensitivity (gold standard)
- Blood cultures if sepsis suspected
- Imaging (ultrasound or CT) if: obstruction suspected, treatment failure, recurrent infection
Treatment
- Uncomplicated lower UTI (women): Trimethoprim-sulfamethoxazole 3 days, or nitrofurantoin 5-7 days, or fosfomycin single dose
- Complicated UTI / pyelonephritis: Fluoroquinolones (ciprofloxacin) 7-14 days; IV antibiotics if septic (piperacillin-tazobactam, ceftriaxone)
- Pre-surgical UTI: Treat to sterile urine before manipulation; if preoperative sterilization impossible, culture-guided perioperative antibiotics
- Key principle: Antibiotics for sepsis should be administered as soon as possible; culture first if feasible
5. Urinary Calculi (Urolithiasis / Nephrolithiasis)
Epidemiology & Risk Factors
- Calcium oxalate stones: most common (80%)
- Struvite (infection) stones: associated with urea-splitting organisms (Proteus, Klebsiella)
- Uric acid stones: associated with gout, low urine pH
- Cystine stones: rare, genetic (cystinuria)
- Major risk factors: dehydration, obesity, hypercalciuria, hyperoxaluria, hypocitraturia, anatomical anomalies, metabolic disorders (renal tubular acidosis, hyperparathyroidism), Medullary sponge kidney
Clinical Features
- Renal colic: Sudden, severe, colicky flank pain radiating to the groin/ipsilateral testicle/labia - classic presentation
- Hematuria (gross or microscopic) in ~90%
- Nausea and vomiting
- Fever = medical emergency (obstruction + sepsis requires urgent decompression)
- CVA tenderness
- Large stones may be palpable as a mass (hydronephrotic kidney)
Special situations:
- Renal transplant patients: no typical renal colic (denervated kidney); may mimic graft rejection
- Pregnancy: most common non-obstetric cause of acute abdominal pain; incidence ~1:1500 pregnancies
- Obesity: limits diagnostic imaging options and treatment delivery (weight limits for CT/fluoroscopy, SWL focal length challenges)
Diagnosis
- Non-contrast CT KUB (CT urogram) - gold standard; detects all stone types, measures size and location
- Ultrasound - preferred in pregnancy; detects hydronephrosis
- Plain KUB X-ray - detects radio-opaque stones (calcium, struvite); uric acid stones are radiolucent
- Urinalysis + urine culture
- Serum creatinine, calcium, uric acid
- 24-hour urine metabolic evaluation (for recurrent stone formers)
Treatment
Conservative (stones <5 mm):
- Adequate hydration + analgesics (NSAIDs, opioids)
- Alpha-blockers (tamsulosin) to facilitate medical expulsive therapy
- Most stones <5 mm pass spontaneously
Interventional:
- ESWL (Extracorporeal Shock Wave Lithotripsy): Stones ≤2 cm; non-invasive
- Ureteroscopy + laser lithotripsy (URS): Ureteral stones; preferred in pregnancy (avoid fluoroscopy)
- Percutaneous Nephrolithotomy (PCNL): Large stones >2 cm, staghorn calculi; requires prone positioning
- Ureteral stent / nephrostomy tube: Emergency decompression for obstructed infected kidney
6. Renal Cell Carcinoma (RCC)
Epidemiology & Risk Factors
- Clear cell RCC (ccRCC): most common subtype; associated with VHL gene mutations (von Hippel-Lindau)
- Risk factors: smoking, obesity, hypertension, hereditary syndromes (VHL, hereditary papillary RCC)
Clinical Features - "Classic Triad" (seen in <10% of cases)
- Hematuria
- Flank pain
- Palpable flank mass
More often now discovered incidentally on imaging. Paraneoplastic syndromes: polycythemia (ectopic EPO), hypercalcemia, hypertension, Stauffer syndrome (non-metastatic hepatic dysfunction).
Diagnosis
- CT scan (abdomen/pelvis) with contrast - key modality; enhancing renal mass
- MRI if iodine allergy or inferior vena cava thrombus assessment
- Biopsy if small/indeterminate mass or prior to systemic therapy
Treatment
- Surgical: Radical or partial nephrectomy (robotic-assisted increasingly used) for localized disease
- Targeted therapy: VEGF inhibitors (sunitinib, pazopanib) or mTOR inhibitors for metastatic disease
- Immunotherapy: Nivolumab + ipilimumab combination - first-line for intermediate/poor-risk metastatic RCC; pembrolizumab + axitinib for favorable-risk
7. Testicular Cancer
Epidemiology
- Most common solid tumor in men aged 15-35
- Risk factors: cryptorchidism, prior contralateral testicular cancer, Klinefelter syndrome
- Isochromosome 12p is a hallmark chromosomal finding
Classification
- Germ cell tumors (GCTs): 95% of cases
- Seminoma (35%): more common; radiosensitive; elevated hCG in ~15%
- Non-seminomatous GCT (NSGCT): teratoma, embryonal carcinoma, yolk sac tumor, choriocarcinoma; elevated AFP and/or hCG
Clinical Features
- Painless testicular mass - classic presentation
- Testicular heaviness or dragging sensation
- ~10% present with acute pain (mimicking epididymo-orchitis)
- Metastatic: back/flank pain (retroperitoneal lymphadenopathy), gynecomastia (hCG-secreting tumors)
Diagnosis
- Testicular ultrasound - first-line imaging; highly sensitive
- Serum tumor markers: AFP, beta-hCG, LDH - essential for staging and monitoring
- CT chest/abdomen/pelvis for staging
- Radical orchiectomy (inguinal approach) - definitive diagnosis + treatment of primary; never do a scrotal biopsy (risk of lymphatic spread to inguinal nodes)
Treatment
- Stage I seminoma: Radical orchiectomy + surveillance, or adjuvant carboplatin x1 cycle, or radiotherapy to para-aortic nodes
- Stage I NSGCT: Orchiectomy + surveillance, or RPLND (retroperitoneal lymph node dissection)
- Advanced (Stage II/III): BEP chemotherapy (bleomycin, etoposide, cisplatin) - highly curative even in metastatic disease
- Prognosis is excellent: overall cure rate >95% for seminoma, ~80% for NSGCT
Clinical Decision Summary
PAINLESS HEMATURIA → Bladder cancer (cystoscopy)
→ Also consider: RCC, upper tract urothelial cancer
PAINFUL HEMATURIA + COLICKY FLANK PAIN → Urolithiasis (CT KUB)
LUTS IN OLDER MAN (hesitancy, weak stream)
→ BPH (most likely)
→ Rule out: prostate cancer (PSA + DRE), urethral stricture
PSA ELEVATED + ABNORMAL DRE
→ Prostate cancer (mpMRI + biopsy)
FEVER + DYSURIA + CVA TENDERNESS → Pyelonephritis (urine culture + imaging)
FEVER + FLANK PAIN + STONE ON CT → Emergency decompression (septic obstruction)
YOUNG MAN + PAINLESS TESTICULAR SWELLING
→ Testicular cancer (ultrasound + tumor markers + inguinal orchiectomy)
→ Differential: epididymo-orchitis (painful, tender, fever)
Sources: Campbell-Walsh-Wein Urology 3-Volume Set; Smith & Tanagho's General Urology 19e; Bailey & Love's Short Practice of Surgery 28e; Robbins & Cotran Pathologic Basis of Disease; Textbook of Family Medicine 9e.
This is a shared conversation. Sign in to Orris to start your own chat.