LIVER CIRROSIS DIAGNOSIS AND TRESTMENT
Reading File
Finding Sources
Searching PubMed
"liver cirrhosis"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Searching the Web
liver cirrhosis diagnosis treatment guidelines 2024 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative content from Goldman-Cecil Medicine, Robbins & Kumar Basic Pathology, and recent guidelines. Here is the full, well-organized answer:
Liver Cirrhosis: Diagnosis and Treatment
1. Definition and Pathology
Cirrhosis is the end stage of any chronic liver disease, defined as the diffuse transformation of the liver into regenerative parenchymal nodules surrounded by fibrous bands. It is not a specific entity - rather, it is the morphologic endpoint of many conditions, and its prognosis and management depend heavily on the underlying etiology and stage.
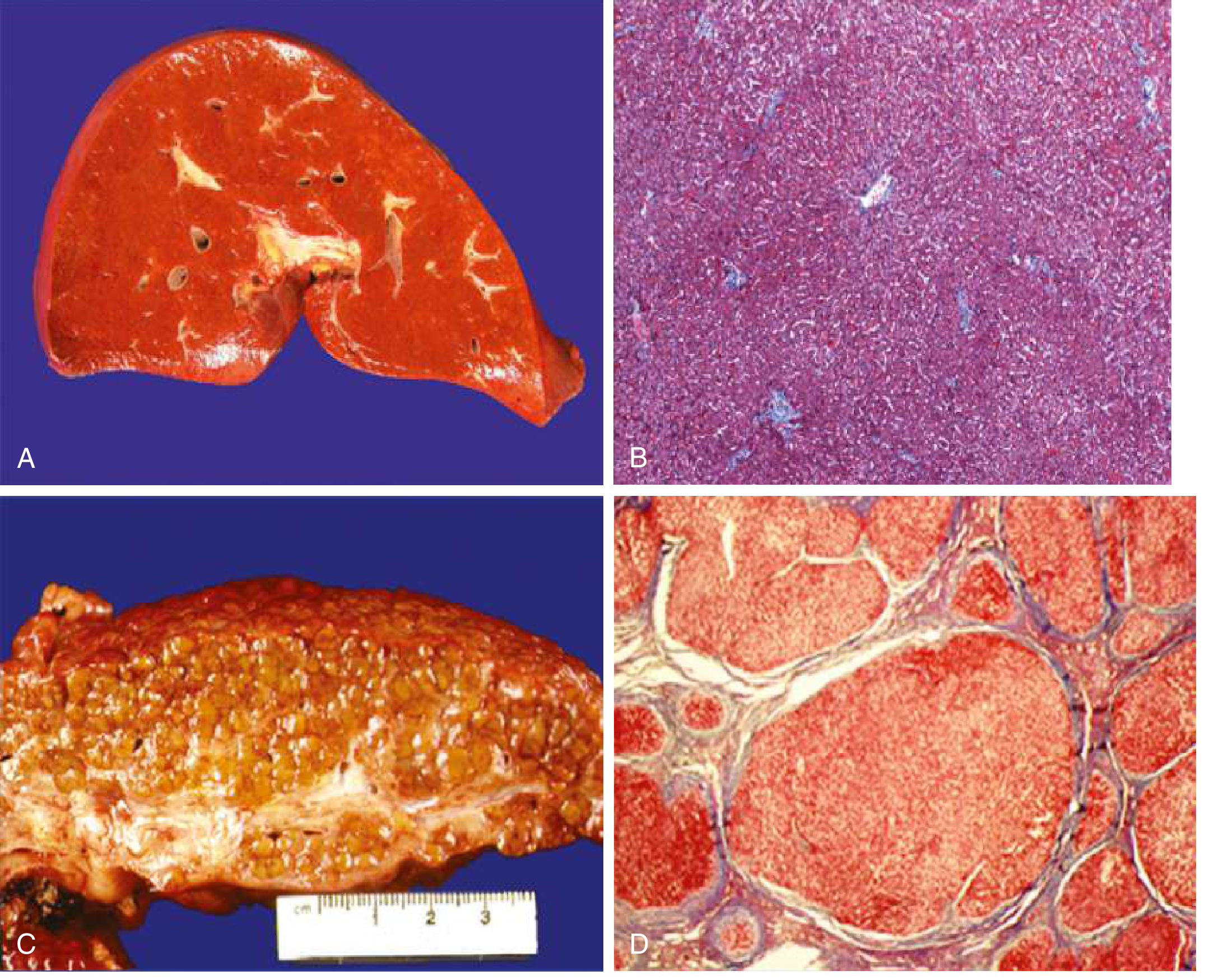
Key pathogenic mechanism: Hepatic stellate cells (Ito cells/perisinusoidal cells), normally quiescent and storing retinoids (Vitamin A) in the space of Disse, become activated by injury. Once activated, they lose their vitamin A stores, proliferate, develop prominent rough endoplasmic reticulum, and secrete extracellular matrix (collagen types I and III, sulfated proteoglycans, glycoproteins). They also become contractile myofibroblasts, leading to sinusoidal narrowing.
Important note: Cirrhosis regression can occur with disease remission or cure. Scars thin, compact, fragment, and adjacent nodules coalesce. All cirrhotic livers contain elements of both progression and regression.
- Goldman-Cecil Medicine, p. 1614-1615
- Robbins & Kumar Basic Pathology, p. 598
2. Etiology
| Main Causes | Other Causes (<2% of cases each) |
|---|---|
| Alcoholic liver disease | Chronic hepatitis C |
| Nonalcoholic/metabolic fatty liver disease (NAFLD/MASLD) | Primary biliary cirrhosis |
| Chronic hepatitis B | Primary sclerosing cholangitis |
| Autoimmune hepatitis | |
| Hemochromatosis, Wilson disease | |
| Alpha-1 antitrypsin deficiency | |
| Budd-Chiari syndrome | |
| Drugs/toxins | |
| Cryptogenic (no identifiable cause) |
- Goldman-Cecil Medicine, Table 139-1, p. 1615
3. Staging
Cirrhosis is classified into two main prognostic stages, now expanded to three:
| Stage | Definition | Annual Mortality |
|---|---|---|
| Compensated (Stage 1-2) | No decompensation; varices may or may not be present | 1.5-2% |
| Decompensated (Stage 3-6) | Presence of ascites, variceal hemorrhage, encephalopathy, or jaundice | 10-87% |
| Recompensated | Decompensated but improving after etiology treatment | Variable |
Decompensated cirrhosis is defined by the development of ascites, variceal hemorrhage, encephalopathy, or jaundice - all consequences of portal hypertension and/or liver insufficiency.
- Goldman-Cecil Medicine, p. 1615
4. Pathophysiology of Complications
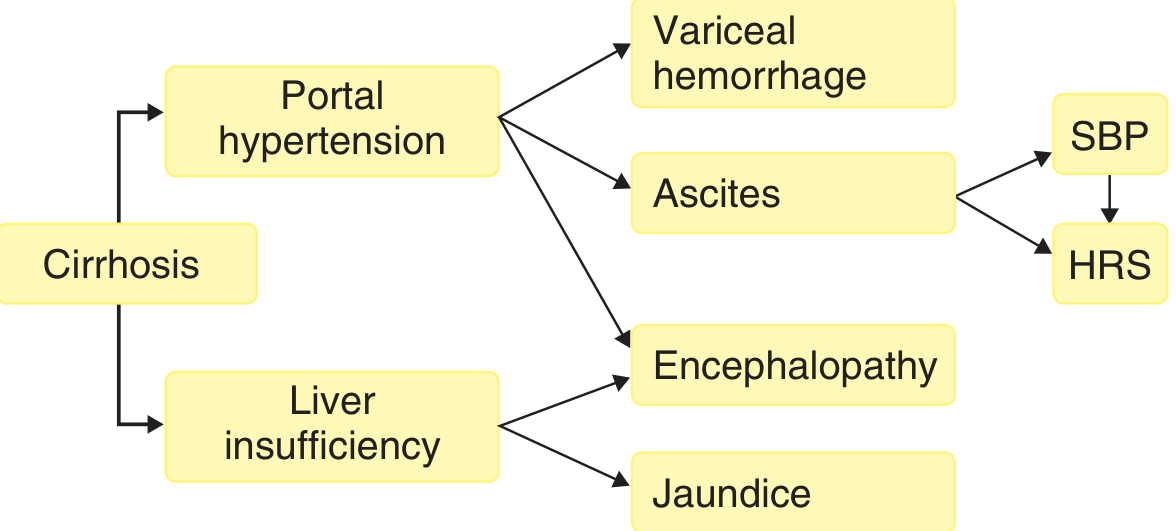
The two main consequences are:
A. Portal Hypertension + Hyperdynamic Circulatory State
- Fixed component: Deposition of fibrous tissue and compression by regenerative nodules
- Functional component: Active vasoconstriction due to intrahepatic nitric oxide (NO) deficiency
- Leads to splanchnic vasodilation, which maintains portal hypertension even as portosystemic collaterals develop
- Hepatic Venous Pressure Gradient (HVPG) >6 mmHg = portal hypertension; >10 mmHg = development of varices; >12 mmHg = risk of variceal bleeding
Consequences:
- Esophagogastric varices - develop in ~40% of advanced-stage patients; may cause fatal hematemesis
- Ascites - fluid transudate in peritoneal cavity (serum-to-ascites albumin gradient [SAAG] ≥1.1 g/dL); ~85% of all ascites is from portal hypertension due to cirrhosis
- Splenomegaly - leading to hypersplenism (thrombocytopenia, pancytopenia)
- Caput medusae - abdominal wall collateral vessels
B. Liver Insufficiency
- Jaundice - failure to excrete bilirubin
- Coagulopathy - reduced clotting factor synthesis
- Hypoalbuminemia - reduced albumin synthesis
- Hepatorenal Syndrome (HRS) - functional renal failure; vasodilators (nitric oxide) cause decreased renal perfusion, activating renin-angiotensin axis and renal sympathetic system
- Hyperestrogenemia (in men) - impaired estrogen metabolism leading to spider angiomas, palmar erythema, gynecomastia, testicular atrophy, hair loss
C. Hepatic Encephalopathy (both mechanisms)
- Neuropsychiatric manifestations; ~2-3% per year incidence
- Grades: 1 (sleep-wake inversion, forgetfulness) → 2 (confusion, disorientation) → 3 (lethargy, profound disorientation) → 4 (coma)
- Hallmark sign: asterixis (flapping tremor)
- Sweet-smelling breath = fetor hepaticus
D. Spontaneous Bacterial Peritonitis (SBP)
- Complication of ascites; infection without apparent surgical source
E. Pulmonary Complications
-
Hepatopulmonary syndrome - exertional dyspnea, clubbing, cyanosis, vascular spiders; present in 5-10% awaiting transplant
-
Portopulmonary hypertension - exertional dyspnea, syncope, chest pain
-
Goldman-Cecil Medicine, p. 1616-1618
-
Robbins & Kumar Basic Pathology, p. 598-600
5. Diagnosis
Clinical Presentation
- ~40% of cirrhotic patients are asymptomatic until advanced stages
- Early/nonspecific: anorexia, weight loss, weakness
Physical Examination Signs
| Sign | Significance |
|---|---|
| Muscle atrophy (bitemporal, thenar/hypothenar) | Liver insufficiency |
| Spider angiomas (trunk, face, upper limbs) | Hyperdynamic circulation |
| Palmar erythema | Vasodilation |
| Jaundice + pruritus | Cholestasis, liver insufficiency |
| Small right liver lobe (<7 cm on percussion) | Pathognomonic |
| Nodular, firm palpable left lobe | Pathognomonic |
| Splenomegaly | Portal hypertension |
| Caput medusae | Portal hypertension |
| Ascites | Portal hypertension |
| Gynecomastia, testicular atrophy | Hyperestrogenemia (males) |
| Dupuytren contracture | Alcoholic cirrhosis |
| Asterixis | Hepatic encephalopathy |
| Petechiae/ecchymoses | Thrombocytopenia/coagulopathy |
Laboratory Tests
| Test | Finding in Cirrhosis |
|---|---|
| Platelet count | <150,000/μL (most sensitive/specific; due to hypersplenism) |
| Albumin | Low |
| Bilirubin | Elevated |
| INR/PT | Prolonged |
| AST, ALT | Elevated |
| GGT | Elevated |
| Hyaluronic acid | Elevated |
| Alpha-2 macroglobulin | Elevated |
| Haptoglobin | Low |
Imaging Studies
- Ultrasound: nodular liver contour, splenomegaly, ascites, collateral vessels
- CT scan: nodular contour, small liver (±caudate/left lobe hypertrophy), collaterals (portal hypertension sign)
- MRI: detailed characterization of liver architecture and vasculature
- Transient elastography (FibroScan)/Acoustic Radiation Force Impulse (ARFI): measures liver stiffness - excellent noninvasive tool for diagnosing and excluding cirrhosis (AASLD-endorsed, supported by 2025 systematic review [PMID: 38489521])
- MR elastography: highly accurate for staging fibrosis
Portal Pressure Measurement
- Hepatic venous pressure gradient (HVPG): via hepatic vein catheterization (wedged minus free pressure)
- Normal: 3-5 mmHg
- Portal hypertension: ≥6 mmHg
- Clinically significant: ≥10 mmHg (varices develop)
- Variceal bleeding risk: >12 mmHg
- HVPG is normal in prehepatic causes (portal vein thrombosis) and in presinusoidal intrahepatic causes (schistosomiasis)
Liver Biopsy
-
Gold standard for definitive diagnosis and determining degree of inflammation
-
Invasive; subject to sampling error
-
Not required when decompensated cirrhosis is evident (ascites + variceal bleeding + encephalopathy in context of chronic liver disease essentially establishes diagnosis)
-
Indicated when: diagnosis uncertain, degree of inflammation unclear, or etiology undetermined
-
Goldman-Cecil Medicine, p. 1617-1620
Prognostic Scoring Systems
- Child-Pugh score (bilirubin, albumin, PT/INR, ascites, encephalopathy): Class A (compensated), B, C (advanced)
- MELD score (creatinine, bilirubin, INR): used for liver transplant prioritization
6. Treatment
Treatment targets both etiology (to prevent progression) and complications (to reduce morbidity and mortality).
A. Etiology-Specific Treatment
| Cause | Treatment |
|---|---|
| Alcohol-related | Complete alcohol abstinence |
| Chronic hepatitis B | Antiviral therapy (tenofovir, entecavir) - can halt/reverse fibrosis |
| Chronic hepatitis C | Direct-acting antivirals (DAAs) - cure leads to fibrosis regression, even in cirrhosis |
| NAFLD/MASLD | Weight loss, metabolic syndrome management; GLP-1 agonists (semaglutide, liraglutide) show benefit for fibrosis regression (PMID: 40736113) |
| Autoimmune hepatitis | Corticosteroids ± azathioprine |
| Primary biliary cirrhosis | Ursodeoxycholic acid (UDCA) ± obeticholic acid |
| Hemochromatosis | Phlebotomy |
| Wilson disease | D-penicillamine or trientine |
B. General Management
- Nutrition: 25-35 kcal/kg/day and 1.2-1.5 g protein/kg/day (compensated); 30-35 kcal/kg/day and 2.0 g/kg/day protein (decompensated)
- Exercise: Aerobic (3 days/week) + resistance training (2 days/week) - improves muscle mass and cardiovascular fitness
- Avoid NSAIDs, nephrotoxins, hepatotoxic drugs
- Vaccinations: Hepatitis A, B, influenza, pneumococcal
C. Management of Complications
Portal Hypertension / Varices
- Non-selective beta-blockers (NSBBs) - propranolol or carvedilol: primary prevention of first variceal bleed (if HVPG >10 mmHg or varices present)
- Endoscopic variceal ligation (EVL): alternative to NSBBs or combined for secondary prophylaxis
- Acute variceal hemorrhage: IV terlipressin or octreotide + EVL + antibiotics (norfloxacin or ceftriaxone for 7 days)
- TIPS (Transjugular Intrahepatic Portosystemic Shunt): for refractory bleeding or recurrent hemorrhage
Ascites
- Sodium restriction (<2 g/day)
- Diuretics: spironolactone (first-line, 50-400 mg/day) ± furosemide (40-160 mg/day)
- Large-volume paracentesis (LVP): for tense/refractory ascites (replace with albumin 8 g/L of fluid removed)
- TIPS: for refractory ascites in selected patients
Spontaneous Bacterial Peritonitis (SBP)
- Diagnosis: Ascitic fluid PMN count ≥250 cells/mm³
- Treatment: IV cefotaxime (or ceftriaxone) + IV albumin (1.5 g/kg at diagnosis, 1.0 g/kg on day 3) to prevent HRS
- Prophylaxis: norfloxacin 400 mg/day (long-term, after first SBP episode or if ascitic protein <1.5 g/dL + renal/hepatic impairment)
Hepatorenal Syndrome (HRS)
- Vasoconstrictors: terlipressin (first-line) or noradrenaline + albumin infusion
- TIPS as bridge to transplant
- Definitive treatment: liver transplantation
Hepatic Encephalopathy
- Lactulose (reduce ammonia via acidification of gut): first-line, titrate to 2-3 soft stools/day
- Rifaximin (non-absorbable antibiotic): added for recurrent/refractory encephalopathy or as secondary prophylaxis
- Identify and treat precipitating causes: infection, GI bleeding, electrolyte disturbances, constipation, medications
Hepatocellular Carcinoma (HCC) Surveillance
- All cirrhotic patients (Child-Pugh A or B) should undergo ultrasound ± AFP every 6 months
- Screening not indicated for Child-Pugh C (unless listed for transplant) or those with <12-month life expectancy
D. Liver Transplantation
-
Only definitive cure for end-stage liver disease
-
Indications: MELD score ≥15, refractory complications (HRS type 1, refractory ascites, recurrent SBP, hepatopulmonary syndrome), HCC within Milan criteria
-
Contraindications: active alcoholism/drug use (typically 6-month abstinence required), extrahepatic malignancy, severe cardiopulmonary disease
-
Post-transplant: immunosuppression (tacrolimus-based regimens), HCC surveillance
-
Goldman-Cecil Medicine, p. 1618-1625
7. Recent Evidence Updates (2024-2026)
- Noninvasive liver staging (PMID: 38489521): A 2025 AASLD-supporting systematic review confirmed that imaging-based tools (transient elastography, MR elastography) are now validated for staging liver fibrosis, reducing the need for liver biopsy.
- GLP-1 receptor agonists for MASH/fibrosis (PMID: 40736113): A 2025 meta-analysis of RCTs found that GLP-1 agonists (semaglutide, liraglutide) significantly improve MASH resolution and liver fibrosis - an important emerging treatment option.
- Pharmacological therapy for MASH (PMID: 39903735): A 2025 network meta-analysis compared multiple agents for fibrosis regression and MASH resolution, helping guide treatment selection.
- Chinese 2025 cirrhosis guidelines introduced the concept of "recompensated cirrhosis" as a third clinical category and reinforced the EASL 6-stage classification system.
Summary Table
| Domain | Key Points |
|---|---|
| Definition | Diffuse nodular fibrosis; end stage of chronic liver disease |
| Leading causes | Alcohol, NAFLD/MASLD, Hepatitis B |
| Stages | Compensated → Decompensated → Recompensated |
| Diagnosis | Clinical + labs + imaging + elastography; biopsy if uncertain |
| Most sensitive lab sign | Thrombocytopenia (<150k) |
| Gold standard diagnosis | Liver biopsy (often unnecessary in decompensated cirrhosis) |
| Key noninvasive test | Transient elastography (FibroScan) |
| Complication driver | Portal hypertension + liver insufficiency |
| Core complications | Varices, ascites, SBP, HRS, encephalopathy, HCC |
| Definitive treatment | Liver transplantation |
Clinical note: Regression of established cirrhosis is possible with effective treatment of the underlying cause (e.g., HCV cure, alcohol abstinence). Even patients with documented cirrhosis may achieve functional recovery with adequate etiology-directed therapy.
Sources:
- Goldman-Cecil Medicine International Edition, pp. 1614-1625
- Robbins & Kumar Basic Pathology, pp. 597-601
- Chinese Guidelines for Clinical Diagnosis, Treatment, and Management of Cirrhosis (2025)
- AASLD Systematic Review on Noninvasive Liver Staging, Hepatology 2025 [PMID: 38489521]
- GLP-1 RA Meta-Analysis, Liver Int 2025 [PMID: 40736113]
This is a shared conversation. Sign in to Orris to start your own chat.