Fracture healing
Reading File
Finding Sources
Searching PubMed
"fracture healing"[MeSH Terms] AND "bone regeneration"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Fracture Healing
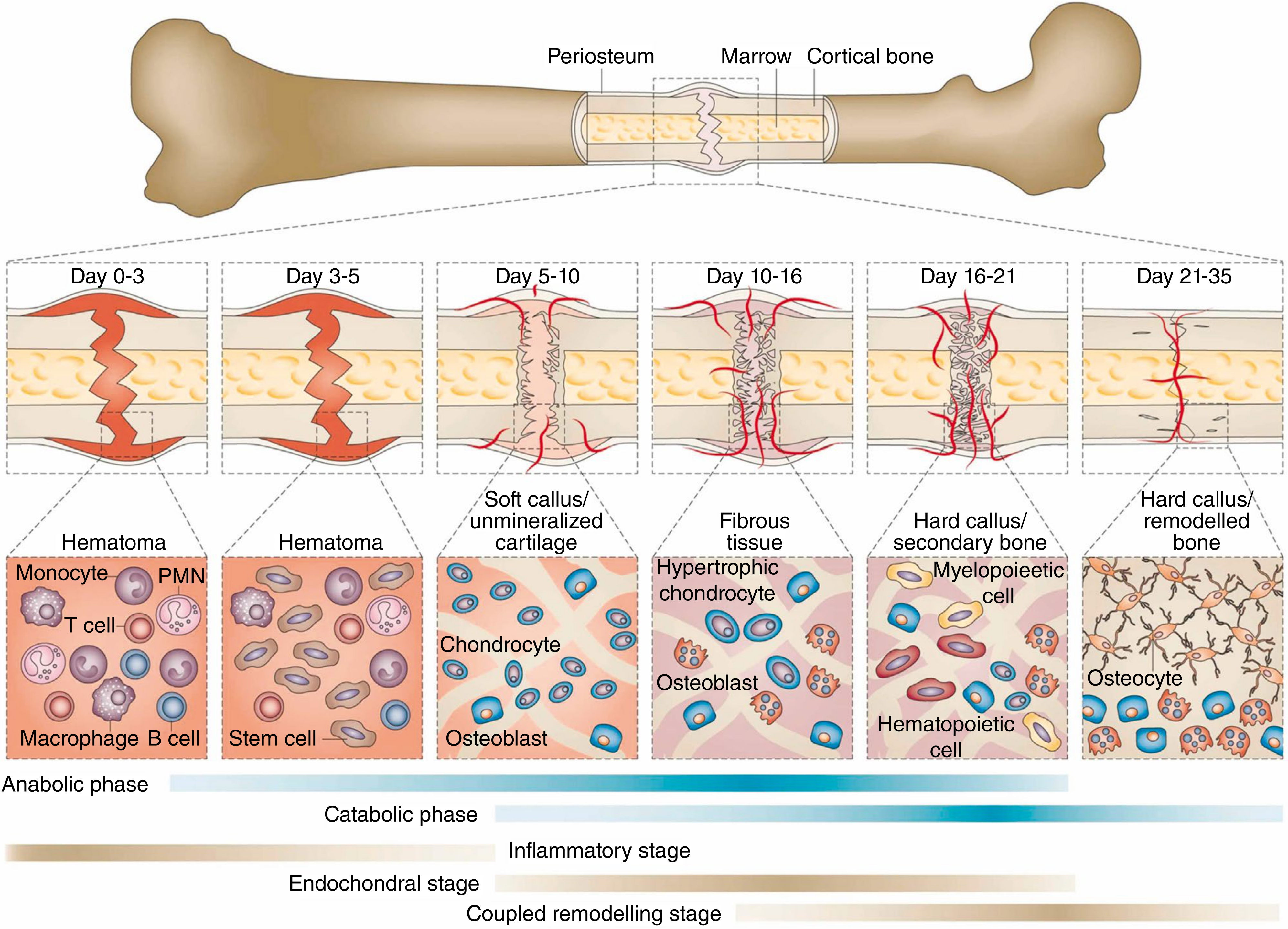
Fracture healing stages with cell types at each phase (Campbell's Operative Orthopaedics, 15th Ed. 2026)
Overview
Fracture healing is a complex biological process requiring the recruitment of appropriate cells (fibroblasts, macrophages, chondroblasts, osteoblasts, osteoclasts) and expression of genes controlling matrix production, growth factors, and transcription factors - at the right time and in the right anatomic location. It initiates a sequence of inflammation, repair, and remodeling that can restore injured bone to its original state within months if each stage proceeds undisturbed. - Campbell's Operative Orthopaedics, 15th Ed.
Two Mechanisms of Healing
Bone can heal by two distinct pathways, and the clinician can influence which pathway occurs through treatment decisions. - Bailey & Love's, 28th Ed.
1. Direct (Primary) Bone Healing
- Occurs under absolute stability with cortical apposition and no movement/gap between fragments
- No callus formation
- Osteoclastic cutting cones cut directly across the fracture line; following osteoblasts lay down lamellar bone across the fracture
- Analogous to normal skeletal remodeling/homeostasis
- Achieved by: compression plating, lag screws
2. Indirect (Secondary) Bone Healing
- The most common form of bone healing
- Involves callus formation - a transition from one tissue type to another
- Requires some movement (strain) at the fracture site - "a little movement is good, too much movement is bad"
- Perren's strain theory: the tissue that differentiates depends on the amount of strain at the fracture site:
- Strain < 100% → fibrous tissue
- Strain < 10% → soft callus
- Strain < 2% → hard callus and progressive mineralization
Stages of Indirect Fracture Healing
| Stage | Timeframe | Key Events | Cell Types |
|---|---|---|---|
| 1. Hematoma Formation | Day 0-3 | Rupture of blood vessels; hematopoietic cells & clots form the initial framework; inflammatory cells invade, initiating lysosomal degradation of necrotic tissue | Monocytes, PMNs, T cells, macrophages, B cells |
| 2. Soft Callus (Granulation Tissue) | Day 3-10 | Pluripotential mesenchymal stem cells invade and differentiate into fibroblasts, chondroblasts, and osteoblasts; angiogenesis occurs; soft cartilaginous callus forms | Stem cells, chondrocytes, osteoblasts |
| 3. Hard Callus (Bony Callus) | Day 10-21 | Cartilaginous callus undergoes endochondral ossification → replaced by woven bone; hypertrophic chondrocytes and osteoblasts are active | Hypertrophic chondrocytes, osteoblasts, hematopoietic cells |
| 4. Remodeling | Day 21+ (months to years) | Woven bone replaced by lamellar bone; medullary canal restored; bone returns to near-normal morphology and mechanical strength; increased bone scan activity long after clinical union | Osteocytes, osteoclasts, osteoblasts |
Four types of new bone formation during repair: osteochondral ossification, intramembranous ossification, appositional new bone formation, and osteonal migration (creeping substitution). - Campbell's
Growth Factors in Fracture Healing
(From Miller's Review of Orthopaedics, 9th Ed.)
| Growth Factor | Key Actions | Notes |
|---|---|---|
| BMP (Bone Morphogenetic Protein) | Osteoinductive; induces metaplasia of mesenchymal cells into osteoblasts | Target = undifferentiated perivascular mesenchymal cells; signals via serine-threonine kinase receptors; intracellular SMADs serve as mediators |
| TGF-β | Induces mesenchymal cells to produce type II collagen & proteoglycans; induces osteoblasts to synthesize collagen | Found in fracture hematomas; regulates cartilage and bone formation in callus; coating implants with TGF-β enhances bone ingrowth |
| IGF-2 | Stimulates type I collagen, cellular proliferation, cartilage matrix synthesis, and bone formation | Signals through tyrosine kinase receptors |
| PDGF (Platelet-Derived Growth Factor) | Chemotactic - attracts inflammatory cells to the fracture site | Released from platelets; signals through tyrosine kinase receptors |
Collagen Types at Each Biochemical Step
| Step | Collagen Type |
|---|---|
| Mesenchymal | I, II, III, V |
| Chondroid | II, IX |
| Chondroid-osteoid | I, II, X |
| Osteogenic | I |
Endocrine Effects on Fracture Healing
| Hormone | Effect | Mechanism |
|---|---|---|
| Cortisone | Negative (-) | Decreased callus proliferation |
| Thyroid hormone, PTH | Positive (+) | Bone remodeling |
| Growth hormone | Positive (+) | Increased callus volume |
| Calcitonin | Possibly positive (+?) | Unknown |
Factors Affecting Fracture Healing
Systemic Factors
- Age, activity level, nutritional status, hormonal factors
- Diseases: diabetes, peripheral vascular disease, malignancy, immunodeficiency
- Vitamin deficiencies (especially D and C)
- Smoking - the most notable inhibitor: delays healing, increases nonunion risk, decreases callus strength, increases pseudarthrosis risk after spinal fusion by up to 500%
Local Factors
- Blood supply and periosteal integrity
- Severity of soft-tissue injury (especially open fractures)
- Neurovascular disruption
- Bone loss, comminution
- Infection
Treatment Factors
- Degree of surgical trauma
- Type of fixation (rigid vs. flexible)
- Fracture distraction/overdistraction
- Load-induced deformation
Drug Effects
- NSAIDs: inhibit COX-2, which is required for normal endochondral ossification - have adverse effects on healing
- Quinolone antibiotics: toxic to chondrocytes, inhibit fracture healing
- Bisphosphonates: theoretically delay healing (suppress bone resorption), but clinical evidence does NOT support harm when started early post-fracture
Terminology of Bone Healing Outcomes
- Union: Fracture has healed sufficiently to withstand physiological loads with minimal pain; radiologically, bone trabeculae cross the fracture site
- Delayed union: Union that takes longer than expected for a particular fracture location
- Malunion: Union occurs but with a residual deformity
- Nonunion: Failure of the fracture to heal
Radioisotope studies show increased activity at fracture sites long after clinical and radiographic union - confirming remodeling continues for years. - Campbell's Operative Orthopaedics
Sources: Campbell's Operative Orthopaedics 15th Ed. 2026 | Bailey & Love's Short Practice of Surgery 28th Ed. | Miller's Review of Orthopaedics 9th Ed. | Rockwood & Green's Fractures in Adults 10th Ed. 2025
This is a shared conversation. Sign in to Orris to start your own chat.