Vagotomy types
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent - I now have comprehensive textbook content and surgical diagrams. Here is the full answer:
Vagotomy - Types, Techniques, and Outcomes
Vagotomy divides vagal nerve fibers to reduce gastric acid secretion. It reduces peak acid output by approximately 50-70% (vagotomy plus antrectomy reduces it by ~85%). Three main types are recognized, differing in the extent of denervation.
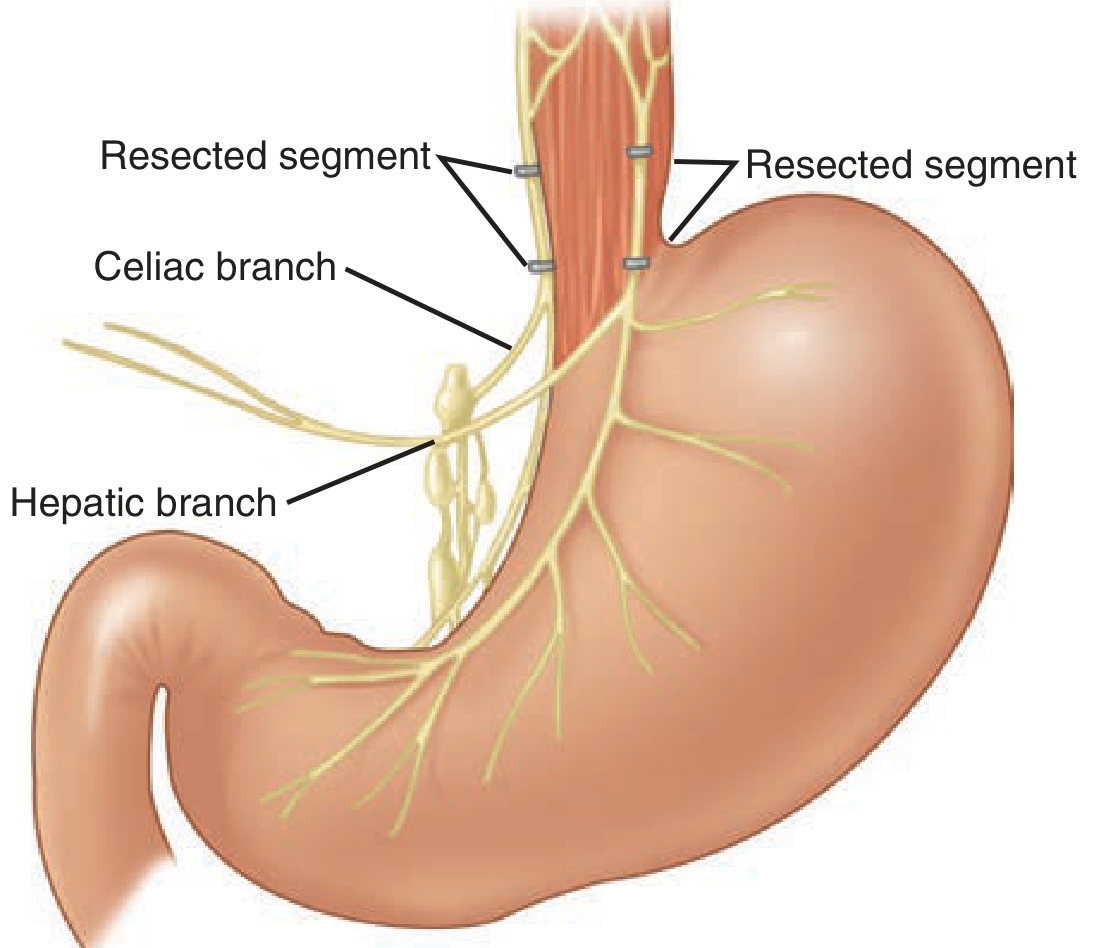
1. Truncal Vagotomy
Division level: Both vagal trunks are divided above the hepatic and celiac branches, at the level of the lower esophagus / gastroesophageal junction.
What is cut: The entire left and right vagus nerves, at least 2 cm of each nerve is resected after proximal and distal ligation.
Consequences:
- Denervates the entire stomach (including antrum and pylorus) + liver, gallbladder, biliary tree, pancreas, small bowel to the mid-transverse colon
- Abolishes pyloric relaxation → gastric stasis in a substantial proportion of patients
- Therefore always requires a drainage procedure (most commonly Heineke-Mikulicz pyloroplasty or gastrojejunostomy)
Drainage options:
- Heineke-Mikulicz pyloroplasty - longitudinal incision through the pyloric ring, closed transversely (most popular)
- Finney pyloroplasty - used when duodenal bulb is scarred
- Jaboulay gastroduodenostomy or gastrojejunostomy - when significant scarring/inflammation is present
2. Selective Vagotomy (Gastric Vagotomy)
Division level: Main right and left vagus nerves are divided just distal to the hepatic and celiac branches.
What is cut: All gastric vagal branches, but the hepatic (from the left vagus) and celiac (from the right vagus) fibers are spared.
Consequences:
- Denervates the entire stomach (including antrum and pylorus)
- Preserves hepatic and celiac innervation - less extragastric side effects than truncal vagotomy
- Still denervates the antrum/pylorus → still requires a drainage procedure
- Side effects (dumping, diarrhea) are similar in magnitude to truncal vagotomy
3. Highly Selective Vagotomy (HSV)
Also called: parietal cell vagotomy, proximal gastric vagotomy, or super-selective vagotomy.
Division level: Only the vagal branches (crow's feet) to the acid-secreting fundus and body of the stomach are divided. The nerves of Latarjet (anterior and posterior) are identified and preserved, along with their antral branches ("crow's feet" to the antrum are preserved).
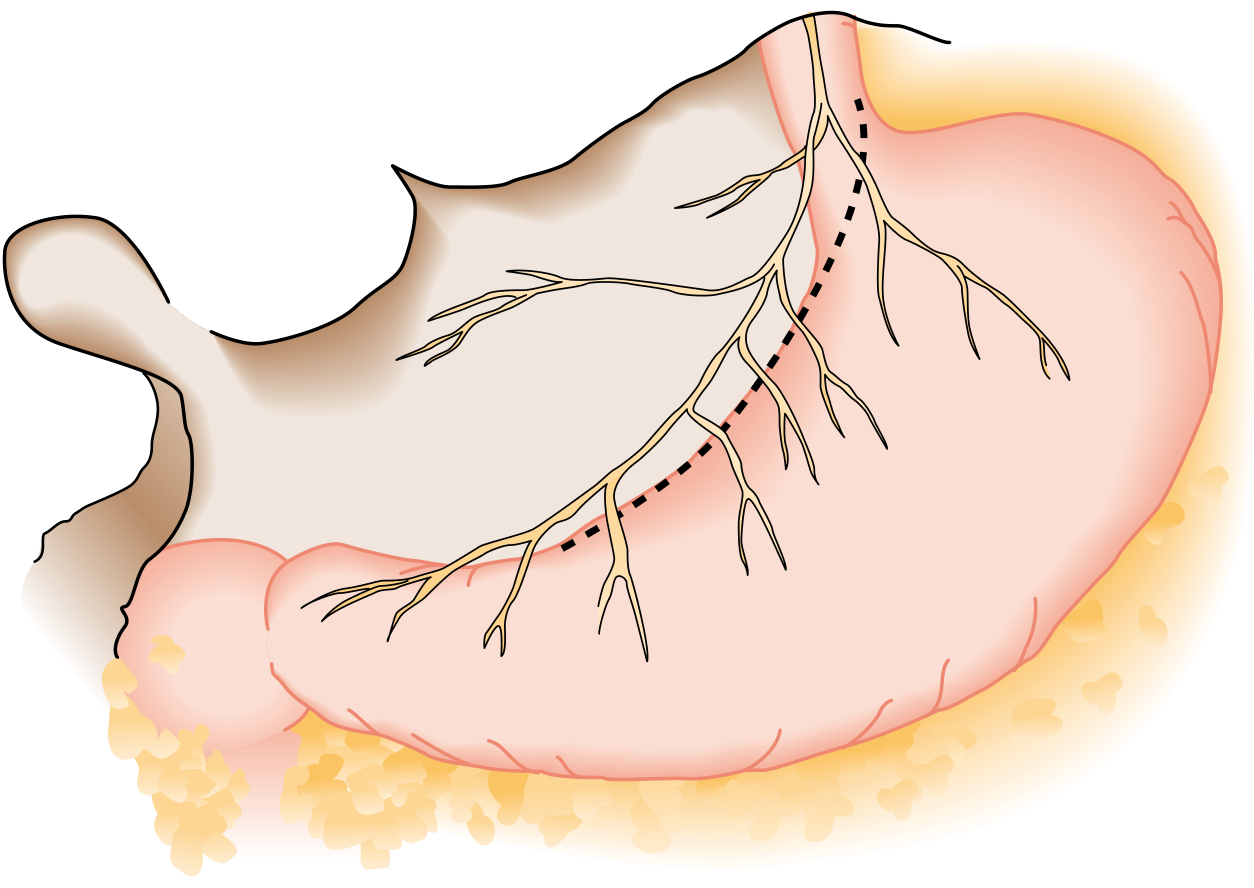
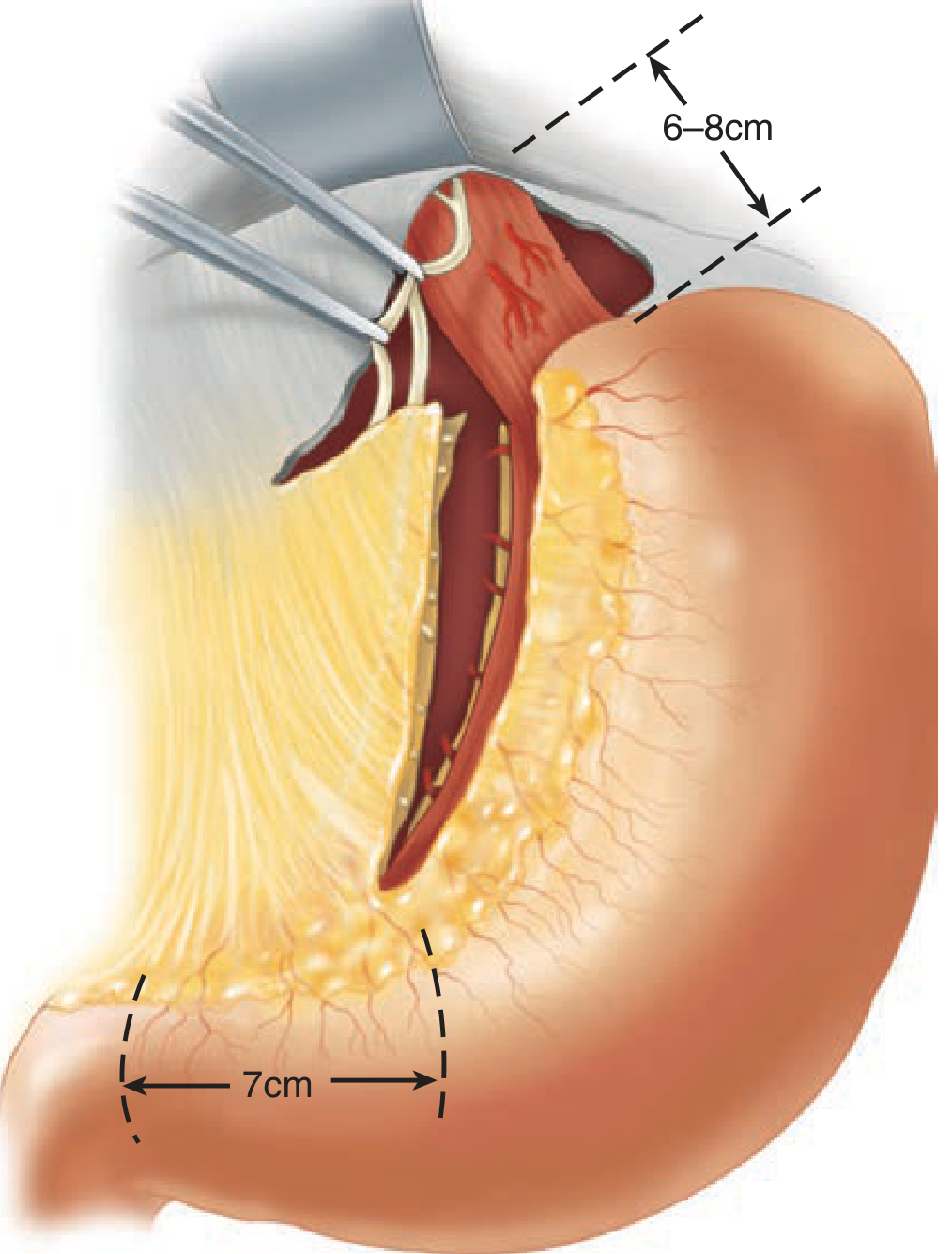
Technical landmarks:
- Dissection begins 7 cm proximal to the pylorus (antral-body junction)
- Continues superiorly to at least 5-6 cm proximal to the GE junction on the esophagus
- The criminal nerve of Grassi (most proximal branch of the posterior vagal trunk) must be identified and divided - if missed, it is a major cause of ulcer recurrence
Advantages:
- Preserves antral/pyloric innervation → no drainage procedure required
- Lowest rates of dumping syndrome and diarrhea
- Lowest operative mortality (<0.2%)
Disadvantage:
- Higher ulcer recurrence rates (10-15%), skill-dependent
- Technically demanding and time-consuming
Comparison Table
| Feature | Truncal Vagotomy + Drainage | Selective Vagotomy + Drainage | Highly Selective Vagotomy |
|---|---|---|---|
| Level of division | Above hepatic/celiac branches | Below hepatic/celiac branches | Crow's feet only (fundus/body) |
| Hepatic/celiac fibers | Cut | Preserved | Preserved |
| Antral innervation | Cut | Cut | Preserved |
| Drainage needed | Yes | Yes | No |
| Operative mortality | <1% | <1% | <0.2% |
| Ulcer recurrence | 2-7% | 5-10% | 2-10% |
| Significant side effects | 10-20% | 10-20% | <5% |
| Dumping (severe) | ~1% | ~1% | ~0% |
| Diarrhea (severe) | ~2% | ~2% | ~0% |
(Source: Bailey and Love's Short Practice of Surgery, 28th ed.; Sabiston Textbook of Surgery; Schwartz's Principles of Surgery, 11th ed.)
Taylor Procedure (Variant)
A posterior truncal vagotomy + anterior seromyotomy (or anterior HSV) - a laparoscopic-friendly alternative to HSV with similar results. Simpler technically than full HSV.
Combined Procedure: Truncal Vagotomy + Antrectomy
When maximum acid suppression is required (e.g., severe refractory PUD, Zollinger-Ellison syndrome), truncal vagotomy is combined with antrectomy:
- Reduces peak acid output by ~85%
- Ulcer recurrence rate: 0-2% (lowest of all procedures)
- Cost: 20% postgastrectomy/postvagotomy syndromes, longer operative time, higher morbidity
Key Points for Exams
- Truncal vagotomy - simplest, quickest, most commonly performed; denervates everything; always needs drainage
- Selective vagotomy - preserves hepatic + celiac branches; still needs drainage; no practical advantage over truncal in clinical outcomes
- HSV - most physiologic; no drainage needed; highest recurrence; lowest morbidity; technically hardest
- Criminal nerve of Grassi = major cause of failed HSV
- Pathologic confirmation of resected vagal trunks should always be performed
This is a shared conversation. Sign in to Orris to start your own chat.