Ventilation perfusion inequality full details for md exams
Reading File
search_medical_text
ventilation perfusion inequality V/Q mismatch mechanisms causes effects
search_medical_text
V/Q ratio dead space shunt hypoxemia hypercapnia respiratory physiology
search_medical_image
ventilation perfusion V/Q ratio lung zones diagram
GradeResponse
GradeResponse
GradeResponse
search_medical_text
normal V/Q ratio lung apex base distribution West zones gravity
search_medical_text
alveolar dead space physiologic dead space Bohr equation shunt equation intrapulmonary shunt
Here is a comprehensive, exam-ready breakdown of Ventilation-Perfusion (V̇/Q̇) Inequality:
Ventilation-Perfusion (V̇/Q̇) Inequality
1. Fundamental Concepts
What is V̇/Q̇?
- Ventilation (V̇): Volume of gas reaching the alveoli per minute (~4 L/min at rest)
- Perfusion (Q̇): Pulmonary blood flow per minute (~5 L/min at rest)
- Overall V̇/Q̇ ratio = 0.8 (normal resting value)
- Efficient gas exchange requires that each alveolus receives ventilation matched to its perfusion
2. Normal Regional V̇/Q̇ Distribution (West's Zones)
Even in healthy lungs, V̇/Q̇ is not uniform — it varies from apex to base due to gravity:
| Region | Ventilation | Perfusion | V̇/Q̇ Ratio | Effect |
|---|---|---|---|---|
| Apex (Zone 1) | High relative to perfusion | Low (gravity-dependent low flow) | High (~3.3) | Wasted ventilation; high PO₂, low PCO₂ |
| Middle (Zone 2) | Intermediate | Intermediate | ~1.0 | Near-ideal gas exchange |
| Base (Zone 3) | Lower relative to perfusion | High (gravity-dependent) | Low (~0.6) | Relative overperfusion; lower PO₂, higher PCO₂ |
Gravity causes blood to preferentially flow to dependent zones. Intrapleural pressure is also less negative at the base, so basal alveoli sit on a steeper part of the compliance curve and expand more per breath — but they start more compressed, so at rest, ventilation is still higher at the base in absolute terms, yet perfusion rises even more steeply.
3. The Two Extremes of V̇/Q̇ Inequality
A. Dead Space (V̇/Q̇ → ∞)
- Alveolus is ventilated but not perfused
- Gas exchange is zero in that unit
- V̇/Q̇ ratio approaches infinity
- Examples: Pulmonary embolism, pulmonary hypertension, emphysema (destroyed capillaries), positive pressure ventilation
Types of Dead Space:
| Type | Definition |
|---|---|
| Anatomical dead space | Conducting airways (trachea to terminal bronchioles) ~150 mL |
| Alveolar dead space | Ventilated alveoli with no perfusion |
| Physiological dead space | Anatomical + Alveolar dead space (measured by Bohr equation) |
Bohr Equation:
V_D/V_T = (PaCO₂ − P_ECO₂) / PaCO₂
Where:
- V_D = dead space volume
- V_T = tidal volume
- PaCO₂ = arterial CO₂
- P_ECO₂ = mixed expired CO₂
Normal V_D/V_T ≈ 0.3 (30% of each tidal breath is wasted)
B. Shunt (V̇/Q̇ → 0)
- Alveolus is perfused but not ventilated
- Deoxygenated blood bypasses gas exchange and enters arterial circulation
- V̇/Q̇ ratio approaches zero
Types of Shunt:
| Type | Examples |
|---|---|
| Anatomical shunt | Bronchial veins draining into pulmonary veins, thebesian veins (~2–3% normal) |
| Intrapulmonary shunt | Consolidation (pneumonia), atelectasis, pulmonary edema, ARDS |
| Cardiac shunt | ASD, VSD, PFO (right-to-left) |
Shunt Equation (Fick principle):
Q_s/Q_t = (CcO₂ − CaO₂) / (CcO₂ − CvO₂)
Where:
- Q_s/Q_t = shunt fraction
- CcO₂ = end-capillary O₂ content (from ideal alveolus)
- CaO₂ = arterial O₂ content
- CvO₂ = mixed venous O₂ content
Normal shunt fraction < 5%
4. Pathophysiology of Hypoxemia in V̇/Q̇ Inequality
Effect on PaO₂ and PaCO₂
| Condition | PaO₂ | PaCO₂ | A-a Gradient |
|---|---|---|---|
| Pure dead space | Initially normal → ↓ if compensation fails | ↑ (if ventilation can't compensate) | Widened |
| Pure shunt | ↓↓ | ↓ (due to hyperventilation of other units) or normal | Widened |
| V̇/Q̇ mismatch (intermediate) | ↓ | Variable | Widened |
| Hypoventilation | ↓ | ↑ | Normal |
Why does low V̇/Q̇ reduce PaO₂ more than high V̇/Q̇ improves it?
This is the key concept behind the asymmetry of V̇/Q̇ inequality:
- The oxygen-haemoglobin dissociation curve is sigmoid (flat at the top)
- A high V̇/Q̇ unit cannot add extra O₂ to already-saturated haemoglobin
- A low V̇/Q̇ unit significantly desaturates haemoglobin
- Net result: mixing low-V̇/Q̇ blood with high-V̇/Q̇ blood still yields low PaO₂
For CO₂, the dissociation curve is nearly linear, so high-V̇/Q̇ units can compensate for low-V̇/Q̇ units → CO₂ is usually normal or even low (from hyperventilation).
5. Response to Supplemental Oxygen — Distinguishing Shunt vs. V̇/Q̇ Mismatch
This is a high-yield exam distinction:
| Feature | V̇/Q̇ Mismatch (low but non-zero) | True Shunt (V̇/Q̇ = 0) |
|---|---|---|
| Response to 100% O₂ | PaO₂ rises markedly | PaO₂ rises minimally (<50 mmHg) |
| Mechanism | O₂ can reach and dissolve in poorly ventilated alveoli | No ventilation → O₂ cannot reach shunted blood |
| A-a gradient on 100% O₂ | Narrows | Remains wide |
| Clinical example | COPD, pulmonary fibrosis | ARDS, lobar consolidation, intracardiac shunt |
According to Harrison's Principles (p. 7866): "Inhalation of supplemental oxygen raises the PaO₂ even in relatively underventilated low V̇/Q̇ regions, and so the arterial hypoxemia induced by V̇/Q̇ heterogeneity is typically responsive to oxygen therapy."
6. Alveolar-Arterial (A-a) Oxygen Gradient
Formula:
A-a gradient = PAO₂ − PaO₂
Alveolar gas equation:
PAO₂ = FiO₂ × (Patm − PH₂O) − (PaCO₂ / RQ) PAO₂ = (0.21 × 713) − (PaCO₂ / 0.8) [on room air at sea level]
| Normal A-a gradient | Interpretation |
|---|---|
| < 10 mmHg (young) | Normal |
| Increases ~3 mmHg per decade | Normal aging |
| > 15–20 mmHg | Pathological V̇/Q̇ mismatch or shunt |
Normal A-a gradient causes of hypoxemia (no V̇/Q̇ inequality):
- Hypoventilation (e.g., CNS depression, neuromuscular disease)
- Low FiO₂ (high altitude)
Widened A-a gradient causes:
- V̇/Q̇ mismatch (COPD, asthma, ILD, pulmonary embolism)
- Shunt (ARDS, pneumonia, atelectasis)
- Diffusion impairment (rare, mainly exercise at high altitude)
7. Causes of V̇/Q̇ Inequality — Clinical Classification
High V̇/Q̇ (Dead Space–Type) Disorders:
| Condition | Mechanism |
|---|---|
| Pulmonary embolism | Obstructed pulmonary arteries → unperfused alveoli |
| Emphysema | Destruction of alveolar-capillary units |
| Pulmonary hypertension | Reduced capillary perfusion |
| Positive pressure ventilation | Over-distension reduces capillary blood flow |
| Haemorrhagic shock | Greatly reduced cardiac output |
Low V̇/Q̇ (Shunt-Type) Disorders:
| Condition | Mechanism |
|---|---|
| Pneumonia / consolidation | Alveoli filled with exudate, not ventilated |
| Atelectasis | Collapsed alveoli continue to be perfused |
| ARDS | Diffuse alveolar damage, flooded alveoli |
| Pulmonary oedema | Fluid-filled alveoli |
| Asthma / COPD | Airway narrowing reduces ventilation to perfused units |
| Mucus plugging | Obstructs ventilation to perfused regions |
8. Compensatory Mechanisms
Hypoxic Pulmonary Vasoconstriction (HPV)
- Unique to pulmonary circulation (opposite of systemic)
- Low alveolar PO₂ → local pulmonary arteriolar constriction → diverts blood away from poorly ventilated units
- Optimizes V̇/Q̇ matching by reducing perfusion to hypoxic regions
- Mediated by inhibition of K⁺ channels in smooth muscle → depolarization → Ca²⁺ influx → vasoconstriction
- Abolished by: hypoxic vasodilators, volatile anaesthetics, high altitude chronic exposure → pulmonary hypertension
Ventilatory Response
- Low V̇/Q̇ regions → ↑ local CO₂ → bronchoconstriction (minor effect) and stimulation to increase ventilation
- Hyperventilation of well-ventilated units compensates for CO₂ retention but cannot compensate for O₂ deficit (due to sigmoid HbO₂ curve)
9. V̇/Q̇ Scan (Scintigraphy) — Clinical Application
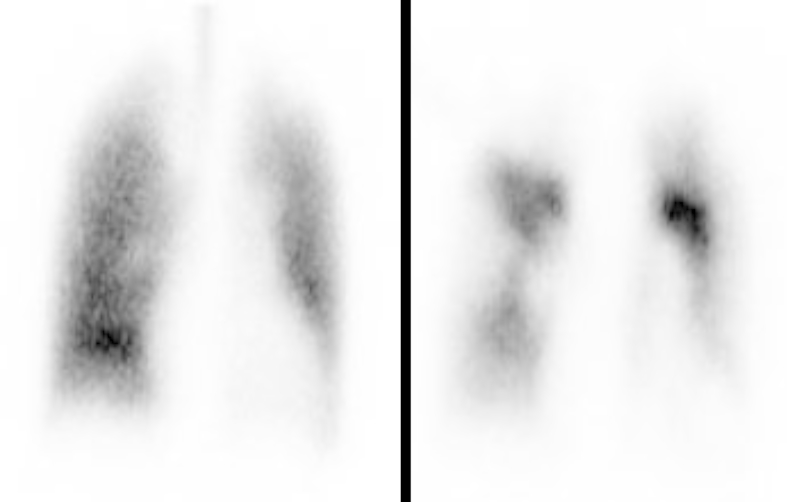
High-probability V/Q scan: Normal ventilation (left panel) with multiple segmental perfusion defects (right panel) — classic pattern for pulmonary embolism (Hugging Face ROCO-Radiology)
PIOPED Criteria:
| Probability | V/Q Pattern |
|---|---|
| High probability (≥80%) | ≥2 large segmental perfusion defects with normal ventilation |
| Intermediate probability | 1 large or 2 moderate V̇/Q̇ mismatches |
| Low probability | Small defects, matched defects |
| Normal | No perfusion defects |
10. High-Yield Summary Table for Exams
| Parameter | Dead Space (High V̇/Q̇) | Shunt (Low V̇/Q̇ = 0) | V̇/Q̇ Mismatch (Low but >0) |
|---|---|---|---|
| V̇/Q̇ ratio | →∞ | →0 | 0.01–0.5 |
| PaO₂ | ↓ | ↓↓ | ↓ |
| PaCO₂ | ↑ (if not compensated) | ↓ (hyperventilation) | ↓ or normal |
| A-a gradient | Widened | Widened | Widened |
| O₂ therapy response | Improves PaO₂ | Minimal improvement | Improves PaO₂ |
| Bohr/Shunt equation used | Bohr | Shunt equation | — |
| Key examples | PE, emphysema | ARDS, consolidation | COPD, asthma, ILD |
11. Key Exam Points (Must-Know)
- Normal V̇/Q̇ = 0.8 overall; apex = ~3.3, base = ~0.6
- V̇/Q̇ mismatch is the most common cause of hypoxemia in clinical disease
- True shunt does NOT respond to 100% O₂ — the gold-standard distinguishing test
- CO₂ is more easily corrected than O₂ in V̇/Q̇ inequality (linear vs. sigmoid dissociation curve)
- A-a gradient is normal in hypoventilation and high altitude (V̇/Q̇ is preserved)
- Hypoxic pulmonary vasoconstriction is the lung's primary defence against V̇/Q̇ mismatch
- Bohr equation measures dead space; shunt equation measures shunt fraction
- ARDS = refractory hypoxia (shunt-predominant) not responsive to O₂ → requires PEEP
- V̇/Q̇ inequality widens both the A-a gradient and the V_D/V_T ratio
- In PE: ventilation normal, perfusion absent → mismatched defect on V/Q scan → high probability
Sources: Harrison's Principles of Internal Medicine, 21st Edition (pp. 7864, 7866); West's Respiratory Physiology; ROCO Radiology Dataset
This is a shared conversation. Sign in to Orris to start your own chat.