notes on physiology of posture (I recommend you to use your source as guyton and hall textbook of physiology and Ganong's review of medical physiology)
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from both Guyton and Ganong. Let me compile the full notes.
Physiology of Posture
Sources: Guyton and Hall Textbook of Medical Physiology (14th ed.) and Ganong's Review of Medical Physiology (26th ed.)
1. Definition and Overview
Posture refers to the orientation and positioning of the body in space, maintained against the force of gravity. It is not a static phenomenon - it is an active, continuous process requiring coordinated input from the motor cortex, brainstem, spinal cord, cerebellum, basal ganglia, vestibular system, and proprioceptors. The primary goal is antigravity support and equilibrium maintenance.
2. Hierarchical Control of Posture
Posture is controlled at multiple levels of the neuraxis in a hierarchical, overlapping fashion:
| Level | Structure | Function |
|---|---|---|
| Spinal cord | Interneurons, motor neurons | Basic postural and locomotor reflexes |
| Brainstem | Reticular nuclei, vestibular nuclei, red nucleus | Antigravity support, righting reflexes, integration |
| Cerebellum | Spinocerebellum, flocculonodular lobe | Coordination, timing, error correction |
| Basal ganglia | Striatum, globus pallidus, SN | Programming and scaling of movements |
| Cortex | Motor cortex, premotor, SMA | Voluntary control, skilled movement |
3. Spinal Cord Postural Reflexes
3.1 Positive Supportive Reaction
Pressure on the footpad of a decerebrate animal causes the limb to extend against the applied pressure - the positive supportive reaction. This is so powerful that after full spinal cord healing, reflexes become exaggerated enough that the limbs can support body weight. Pressure on one side of the pad causes extension in that direction - the magnet reaction - helping prevent the animal from falling toward that side.
- Guyton & Hall, p. 684
3.2 Cord Righting Reflex
When a spinal animal is placed on its side, it makes uncoordinated movements to return to standing. This cord righting reflex demonstrates that relatively complex postural reflexes are integrated at the spinal level alone. Animals with thoracic cord transections can still right themselves and even walk with hindlimbs, though hindlimb movements are no longer synchronized with forelimb movements.
- Guyton & Hall, p. 684
3.3 Reciprocal Innervation and Stepping
The spinal cord controls stepping through mutually reciprocal inhibition circuits that oscillate between agonist and antagonist motor neurons. Even after sensory nerve section, rhythmic stepping can continue. Key spinal stepping mechanisms include:
- Rhythmical stepping of a single limb - forward flexion followed by backward extension, repeating
- Reciprocal stepping of opposite limbs - when one limb steps forward, the opposite steps backward
- Diagonal (mark time) stepping - the two forelimbs alternate with the two hindlimbs
- Stumble reflex - if the dorsum of the foot hits an obstacle during forward thrust, forward thrust stops, the foot lifts higher, and steps over the obstacle
- Guyton & Hall, p. 684-685
4. Brainstem Postural Control
4.1 Reticular Nuclei - Antigravity Support
The reticular nuclei in the brainstem are the primary controllers of antigravity muscles. They function in an antagonistic pair:
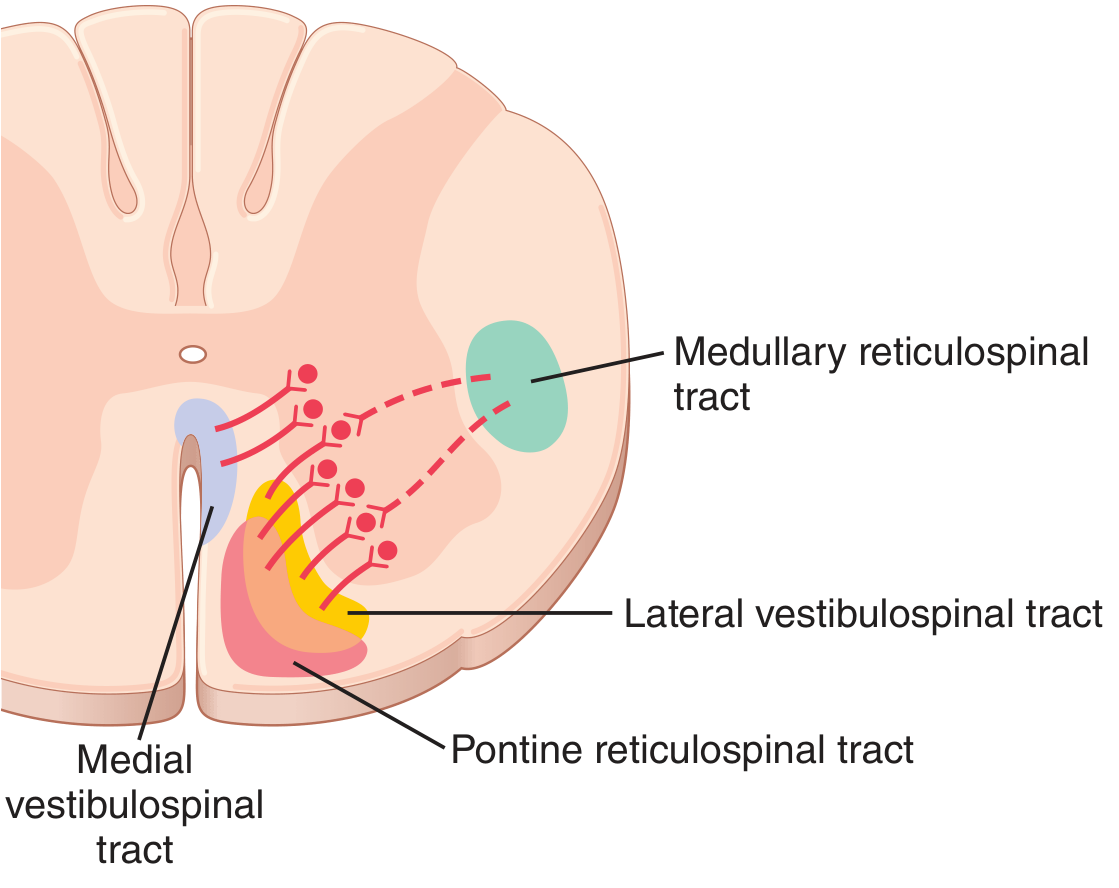
Pontine Reticular Nuclei (Excitatory)
- Located posterolaterally in the pons, extending into the mesencephalon
- Transmit excitatory signals via the pontine reticulospinal tract (anterior column of spinal cord)
- Target: medial anterior motor neurons controlling axial and extensor (antigravity) muscles
- Have high intrinsic excitability and receive strong excitatory input from vestibular nuclei and deep cerebellar nuclei
- When unopposed, they can maintain standing posture in 4-legged animals without any cortical input
- Guyton & Hall, p. 693
Medullary Reticular Nuclei (Inhibitory)
- Transmit inhibitory signals via the medullary reticulospinal tract (lateral column)
- Receive input collaterals from: corticospinal tract, rubrospinal tract, and other pathways from higher brain centers
- Function: modulate and inhibit antigravity tone under higher control
- Guyton & Hall, p. 693
4.2 Vestibular Nuclei and Equilibrium
The vestibular nuclei work closely with the reticular nuclei. They:
- Receive input from utricle, saccule, and semicircular canals
- Project via the lateral vestibulospinal tract (ipsilateral excitation of extensor muscles) and medial vestibulospinal tract (bilateral effects on neck and upper trunk muscles)
- Provide continuous postural adjustments based on head position in space
Utricle and Saccule (Static Equilibrium)
The hair cells in the maculae of the utricle and saccule are oriented in all directions. With different head positions, different patterns of hair cells are stimulated, signaling head position relative to gravity. The vestibular, cerebellar, and reticular motor systems then excite the appropriate postural muscles. A person can detect as little as 0.5 degrees of body lean from vertical.
- Guyton & Hall, p. 695-696
Semicircular Ducts (Dynamic/Angular Equilibrium)
When the head rotates, endolymph lags behind due to inertia, causing relative fluid flow that deflects the cupula and stimulates hair cells. This signals angular acceleration in 3 planes of space, triggering rapid postural corrections.
- Guyton & Hall, p. 696
4.3 Brainstem Pathways - Medial vs. Lateral Systems (Ganong)
Spinal motor neurons are organized such that those innervating the most proximal muscles are located most medially in the ventral horn, and those innervating distal muscles are located more laterally.
- Medial brainstem pathways (reticulospinal, vestibulospinal): control proximal and axial muscles - primarily for posture and balance
- Lateral brainstem pathways (rubrospinal): control distal limb muscles - primarily for voluntary skilled movement
- Ganong's, p. 246
Rubrospinal Tract
The red nucleus (mesencephalon) receives input from motor cortex and gives rise to the rubrospinal tract, which crosses at the lower brainstem. It excites flexor motor neurons and inhibits extensor motor neurons in the dorsolateral ventral horn. It is not prominent in healthy humans but becomes significant in decorticate rigidity.
- Ganong's, p. 247
5. Posture-Regulating Systems - Decerebration and Decortication
These experimental and clinical states reveal the hierarchical nature of postural control.
5.1 Decerebrate Rigidity
A complete transection between the superior and inferior colliculi (midcollicular decerebration) disconnects:
- All cortical input (corticospinal + corticobulbar tracts)
- Red nucleus input (rubrospinal tract)
The result is that excitatory reticulospinal and vestibulospinal pathways dominate, producing hyperactivity of extensor muscles in all four extremities = decerebrate rigidity.
Mechanism: The excitatory reticulospinal drive activates gamma motor neurons, which indirectly activate alpha motor neurons via Ia spindle afferent activity - this is the gamma loop. Cutting dorsal roots to a limb immediately eliminates the rigidity (demonstrated experimentally). This resembles the posture seen clinically after uncal herniation from a supratentorial lesion.
Clinical appearance (decerebrate posturing):
- Upper extremities: extended, pronated forearms, fingers flexed
- Lower extremities: extended, toes pointed inward
- Head and neck: extended
- Ganong's, p. 248-249
5.2 Decerebellate Rigidity
If the anterior lobe of the cerebellum is also removed in a decerebrate animal, extensor hyperactivity is further exaggerated (decerebellate rigidity). Mechanism: loss of cortical inhibition of the cerebellar fastigial nucleus, which secondarily increases excitation to vestibular nuclei. Notably, dorsal root section does NOT reverse this rigidity - meaning alpha motor neurons are being directly activated, independent of the gamma loop.
- Ganong's, p. 249
5.3 Decorticate Rigidity
Injury to the cerebral cortex (decortication) produces a different pattern:
- Upper extremities: FLEXED at the elbow (rubrospinal excitation of flexors in upper extremities is preserved)
- Lower extremities: EXTENDED (same mechanism as decerebration)
- Head: extended
The key difference from decerebration is upper-limb flexion, because the rubrospinal tract (arising below the cortex) excites upper-limb flexors when cortical inhibition is lost.
Clinical appearance (decorticate posturing):
- Arms flexed at elbows, wrists, and fingers
- Legs extended
- Ganong's, p. 249
6. Higher Centers in Postural Control
6.1 Cerebellum
The spinocerebellum (vermis and intermediate hemispheres) receives proprioceptive, vestibular, and motor cortex input and plays a major role in postural correction. The flocculonodular lobe is specifically dedicated to vestibular input and equilibrium. Cerebellar output adjusts ongoing movements and posture in real time by modulating brainstem and cortical motor commands.
6.2 Basal Ganglia
Neurons in the basal ganglia discharge before movements begin, involved in planning and programming. They influence the motor cortex via the thalamus, and GPi projects to brainstem nuclei to modulate motor neurons. Though primarily associated with movement programming, they contribute to postural readiness and set - the background tone of motor preparation.
- Ganong's, p. 251
6.3 Motor Cortex
The motor cortex does not micromanage posture but sets the overall "level" of excitability and voluntary override. The premotor area and supplementary motor area (SMA) are especially important for programming postural adjustments that precede voluntary movement (anticipatory postural adjustments). Corticospinal input to the medullary reticular nuclei modulates the inhibitory reticulospinal drive on antigravity muscles.
7. Sensory Inputs for Postural Control
Three main sensory systems contribute:
| System | Receptors | Role |
|---|---|---|
| Vestibular | Otoliths (utricle/saccule), semicircular canals | Head position, linear and angular acceleration |
| Proprioceptive | Muscle spindles (Ia, II), Golgi tendon organs (Ib), joint receptors | Limb position, load, muscle length and tension |
| Visual | Retina | Spatial orientation, visual vertical reference |
Any two of these three systems are generally sufficient to maintain normal posture. Clinical tip: patients with peripheral vestibular loss can compensate well if vision and proprioception are intact (but fall with eyes closed on an unstable surface = positive Romberg).
8. Summary of Descending Motor Tracts Relevant to Posture
| Tract | Origin | Column in Cord | Primary Target | Effect |
|---|---|---|---|---|
| Pontine reticulospinal | Pontine reticular nuclei | Anterior | Medial anterior motor neurons (axial/extensors) | Excitatory (antigravity) |
| Medullary reticulospinal | Medullary reticular nuclei | Lateral | Same | Inhibitory |
| Lateral vestibulospinal | Lateral vestibular nucleus (Deiters) | Anterior | Extensor motor neurons | Excitatory |
| Medial vestibulospinal | Medial vestibular nucleus | Anterior (bilateral) | Neck/upper trunk | Position correction |
| Rubrospinal | Red nucleus (midbrain) | Lateral | Distal limb flexors | Excites flexors, inhibits extensors |
| Corticospinal | Motor cortex | Lateral + anterior | All levels | Fine voluntary control |
9. Key Clinical Correlations
| Finding | Localization | Mechanism |
|---|---|---|
| Decerebrate posturing | Lower midbrain / upper pons lesion | Excitatory reticulospinal and vestibulospinal pathways unopposed |
| Decorticate posturing | Upper midbrain lesion / cortical damage | Rubrospinal (flexion of arms) + vestibulo/reticulospinal (extension of legs) |
| Spasticity (UMN lesion) | Corticospinal tract damage | Loss of inhibitory modulation of pontine reticular excitatory drive |
| Hypotonia (LMN/cerebellar) | LMN or cerebellum | Loss of stretch reflex arc or loss of cerebellar facilitation |
| Positive Romberg | Proprioceptive / vestibular loss | Loss of two of three postural sensory inputs |
References
- Guyton and Hall Textbook of Medical Physiology, 14th Edition - Chapters 55 (Spinal reflexes) and 56 (Cortical and brainstem motor control), pp. 684-696
- Ganong's Review of Medical Physiology, 26th Edition - Chapter 12 (Reflex arc and control of movement), pp. 246-251
This is a shared conversation. Sign in to Orris to start your own chat.