I now have all the foundational material needed. Let me compose the complete, comprehensive learning note.
COMPLETE LEARNING NOTE: DRUG TREATMENT OF ANXIETY AND INSOMNIA
Based on Katzung's Basic & Clinical Pharmacology (16th Ed.), Goodman & Gilman's Pharmacological Basis of Therapeutics, Kaplan & Sadock's Comprehensive Textbook of Psychiatry, Kaplan & Sadock's Synopsis of Psychiatry, and Stahl's Essential Psychopharmacology
SECTION 1: BIG PICTURE OVERVIEW
What Problem Does This Drug Class Solve?
Imagine your brain has a volume dial. When you are calm and sleeping peacefully, the dial is turned down - the brain is quiet, not sending too many alarm signals. When you are anxious, that dial is turned up too high. When you have insomnia, the dial refuses to turn down at night, even though you desperately want it to.
Anxiety is the brain stuck in a state of excessive alarm - the "fight or flight" circuits are firing even when there is no real danger. The person feels constant dread, tension, a pounding heart, and an inability to relax.
Insomnia is the inability to fall asleep or stay asleep because the brain's arousal system is still active when it should be shutting down.
Both conditions arise because of an imbalance between the brain's excitatory systems (systems that rev the brain up) and inhibitory systems (systems that calm it down).
What the drugs are trying to achieve:
- Turn the brain's activity DOWN
- Reduce excessive nerve firing
- Allow the natural calming and sleep-initiating systems to take over
Where the drugs act:
- Mostly at the GABA-A receptor - the brain's main brake pedal
- At serotonin receptors - fine-tuning emotional tone
- At melatonin receptors - resetting the body clock
- At orexin receptors - blocking the wake-promoting system
Think of it this way: anxiety and insomnia both happen because the brain's brake system is too weak or the accelerator system is too strong. These drugs either strengthen the brakes or weaken the accelerator.
SECTION 2: BUILD THE FOUNDATION
2A. Normal Brain Chemistry - How the Brain Stays Balanced
The brain contains billions of nerve cells (neurons) that communicate by sending chemical messages called neurotransmitters. Some neurotransmitters are excitatory (they tell the next nerve cell to fire, like pressing the gas pedal) and some are inhibitory (they tell the next nerve cell to slow down or stop, like pressing the brake pedal).
GABA (Gamma-Aminobutyric Acid) - the brain's main brake pedal
- GABA is the most important inhibitory neurotransmitter in the brain
- When GABA is released, it binds to the GABA-A receptor, which opens a channel that lets negatively charged chloride (Cl-) ions flow into the nerve cell
- When Cl- enters, the inside of the nerve cell becomes more negatively charged (this is called hyperpolarization)
- A hyperpolarized nerve cell is harder to fire - it is effectively "quieter"
- GABA = braking signal. More GABA = quieter brain
Simple analogy: GABA is like a security guard at a nightclub. Every time a customer (excitatory signal) tries to enter, GABA tells them to slow down. When there are lots of GABA guards, the nightclub stays quiet and orderly.
Glutamate - the brain's main accelerator
- Glutamate is the most abundant excitatory neurotransmitter
- It fires neurons, promotes alertness and activity
- Balance between GABA and glutamate controls the overall tone of the brain
Serotonin (5-HT) - the mood stabilizer
- Serotonin modulates mood, emotion, and anxiety
- Low serotonin is linked to anxiety and depression
- Several anxiety pathways involve serotonin signals going wrong
Norepinephrine (NE) - the alarm chemical
- In anxiety disorders, the locus coeruleus (a brain region rich in NE neurons) fires too much
- This causes the physical symptoms of anxiety: racing heart, sweating, trembling
Orexin (Hypocretin) - the wake-keeping chemical
- Orexin is produced in the hypothalamus (a deep brain region)
- It promotes wakefulness and prevents falling asleep
- In insomnia, orexin may be overactive, keeping the person awake
Melatonin - the darkness hormone
- Produced by the pineal gland when it gets dark
- Signals the brain that it is nighttime and promotes sleep
- Acts on MT1 and MT2 receptors to regulate the sleep-wake cycle
2B. The GABA-A Receptor - The Star of This Topic
The GABA-A receptor deserves special attention because most drugs in this topic work here.
Structure:
- The GABA-A receptor is a pentameric structure (penta = five) - meaning it is made of 5 protein subunits arranged in a circle
- In the center of this circle is a channel (a pore) that chloride ions can pass through
- The most common version in the brain contains: 2 alpha (α) subunits + 2 beta (β) subunits + 1 gamma (γ) subunit
- There are multiple subtypes of each subunit (e.g., six types of α-subunit: α1 through α6)
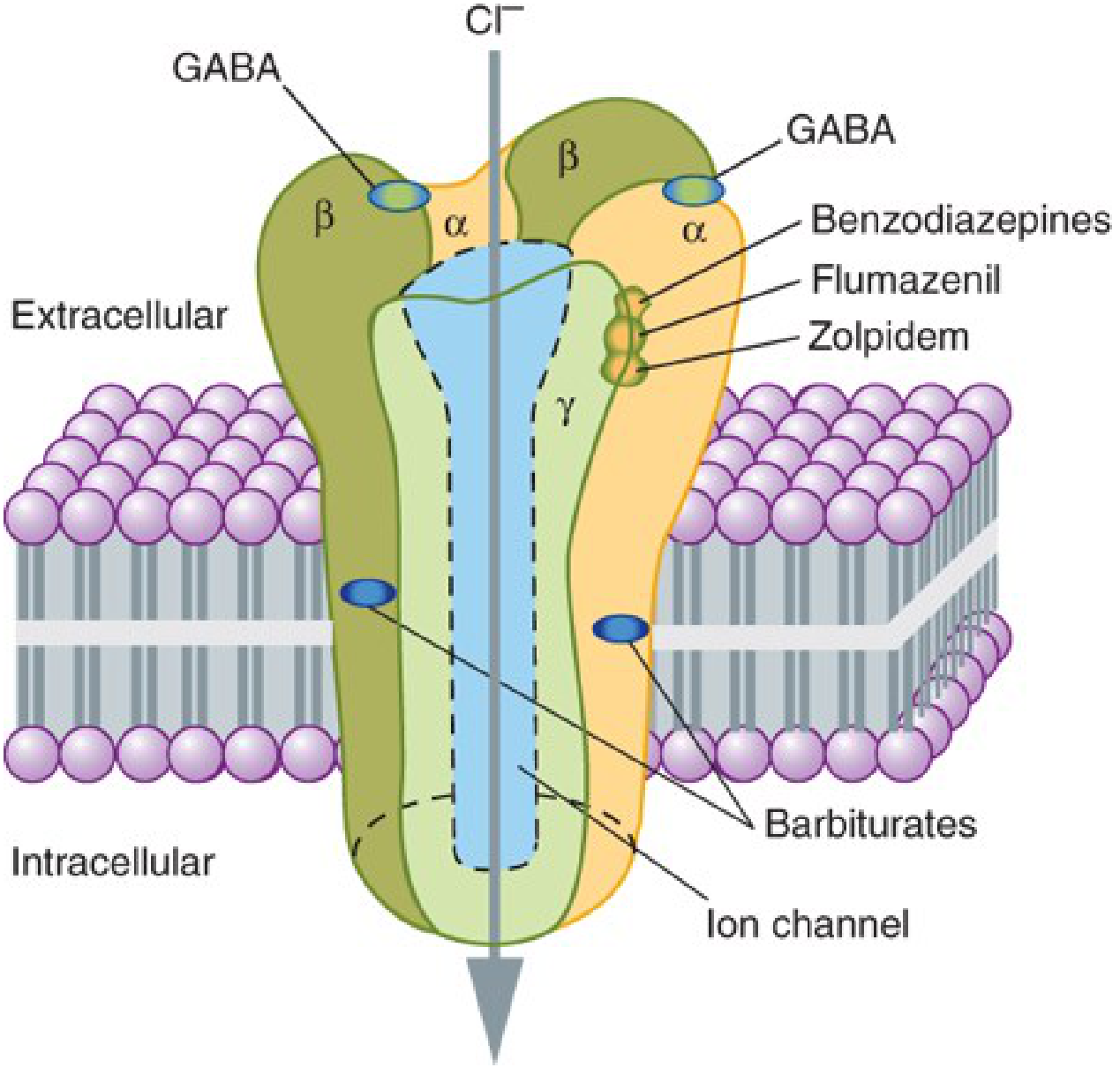
Binding sites (this is critical for exams):
| Drug Class | Where It Binds | Effect |
|---|
| GABA itself | Between α and β subunits (2 sites) | Directly opens Cl- channel |
| Benzodiazepines | Between α and γ subunits (1 site) | Increases frequency of Cl- channel opening |
| Barbiturates | Separate site on β subunit | Increases duration of Cl- channel opening |
| Z-drugs (zolpidem etc.) | Same site as benzodiazepines (α-γ interface) | Similar to benzodiazepines but more selective |
| Flumazenil (antidote) | Same site as benzodiazepines | Blocks benzodiazepine binding (competitive antagonist) |
The key difference between benzodiazepines and barbiturates:
- Benzodiazepines = increase FREQUENCY (the channel opens more often)
- Barbiturates = increase DURATION (the channel stays open longer)
- This difference explains why barbiturates are far more dangerous in overdose - prolonged channel opening causes deeper CNS depression and death from respiratory failure
Important rule: Neither benzodiazepines nor barbiturates open the chloride channel on their own. GABA must be present. They only make GABA work better. This is called positive allosteric modulation (allosteric = acting at a different site from GABA but affecting the same channel).
Analogy: GABA is a key that opens a door. Benzodiazepines are like a locksmith's oil - they make the key work faster and more easily. But without the key (GABA), the oil does nothing. Barbiturates are like a doorstop that holds the door open longer once the key has been used.
Visual diagram of the GABA-A receptor complex:
From Katzung's Basic & Clinical Pharmacology, 16th Ed. - GABA-A receptor pentameric structure showing the α-γ binding interface where benzodiazepines, zolpidem, and flumazenil bind, and the separate barbiturate binding sites.
2C. Subunit Selectivity and Clinical Effects
This is exam-favorite material:
| GABA-A Subunit | When Activated, Mediates |
|---|
| α1 | Sedation, anterograde amnesia, anticonvulsant effect, some anxiolysis |
| α2, α3 | Anxiolytic effects, muscle relaxation |
| α5 | Memory and learning (hippocampus) |
| α4, α6 | Insensitive to benzodiazepines |
Benzodiazepines bind to receptors containing α1, α2, α3, and α5 subunits - they are non-selective, which is why they produce sedation, anxiolysis, muscle relaxation, and amnesia all at once.
Z-drugs (especially zolpidem) are selective for α1-containing receptors - this is why they are primarily sedating/hypnotic with less anxiolytic, muscle relaxant, and amnestic effect.
2D. Sleep Architecture - Why It Matters for Insomnia Drugs
Normal sleep moves through several stages in cycles:
Stage N1 (light sleep)
↓
Stage N2 (true sleep - sleep spindles, K-complexes)
↓
Stage N3/N4 (deep/slow wave sleep - restorative)
↓
REM sleep (dreaming, memory consolidation)
↓
Repeat cycle every ~90 minutes
- Normal adults spend about 20-25% of sleep in REM
- Deep sleep (N3/N4) is essential for physical restoration
- REM sleep is essential for emotional and memory processing
Drug effects on sleep architecture:
- Benzodiazepines and barbiturates suppress slow-wave sleep and suppress REM sleep
- This means patients sleep more but sleep less restoratively
- REM rebound occurs on withdrawal (excessive vivid dreams)
- Z-drugs have less effect on sleep architecture than benzodiazepines
2E. The Pathophysiology of Anxiety Disorders
In anxiety disorders, the brain's alarm system is hyperactive. The key structures involved are:
Prefrontal Cortex (thinks rationally)
↓ loses control over ↓
Amygdala (processes fear and threat)
↓ overactivates ↓
Hypothalamus → releases CRH → pituitary → cortisol (stress response)
Locus Coeruleus → releases norepinephrine → physical anxiety symptoms
Raphe nuclei (serotonin) → if dysregulated → emotional dysregulation
In anxiety:
- The amygdala fires excessively even without real threat
- Prefrontal cortex "top-down control" over the amygdala is impaired
- GABAergic inhibition of these circuits is insufficient
- The result: constant alarm, worry, physical tension, avoidance behavior
This is why drugs that enhance GABA work for anxiety - they restore the inhibitory tone in these circuits.
SECTION 3: DRUG CLASS FRAMEWORK
DRUG CLASS 1: BENZODIAZEPINES
Definition: Benzodiazepines are a class of drugs that share a chemical structure consisting of a benzene ring fused to a diazepine ring. They are positive allosteric modulators (PAMs) of the GABA-A receptor.
The name "benzodiazepine":
- "Benzo" = benzene ring
- "Diazepine" = a 7-membered ring containing 2 nitrogen atoms
- When you fuse these rings together and add specific substituents, you get a benzodiazepine
Mechanism of Action (Step by Step)
Step 1: A nerve cell in the brain is firing too rapidly (as in anxiety)
Step 2: GABA is released onto the nerve cell, trying to slow it down
Step 3: GABA binds to its site on the GABA-A receptor (between α and β subunits)
Step 4: This causes the Cl- channel to open briefly, letting Cl- in - the cell becomes less excitable
Step 5: A benzodiazepine molecule binds to the BZ site (between α and γ subunits)
Step 6: This binding changes the shape (conformation) of the receptor allosterically - it makes the channel more responsive to GABA
Step 7: Now, the same amount of GABA causes the channel to open MORE FREQUENTLY
Step 8: More Cl- enters the cell → greater hyperpolarization → cell fires less → brain activity decreases → anxiety/insomnia reduced
The one-sentence mechanism for MCQs: Benzodiazepines bind to the α-γ subunit interface of the GABA-A receptor and increase the FREQUENCY of chloride channel opening in response to GABA.
Pharmacological Effects (Dose-Dependent)
Benzodiazepines produce a spectrum of effects depending on dose:
Low dose → Anti-anxiety (anxiolysis)
→ Sedation (calm, drowsy feeling)
Medium → Hypnosis (sleep induction)
→ Muscle relaxation
High dose → Anticonvulsant effect
→ Anesthesia (with IV benzodiazepines like midazolam)
Very high → Unconsciousness but rarely fatal alone
(they reach a "ceiling" - they cannot open the channel
more than a maximum amount because GABA must be present)
Why benzodiazepines don't kill you in overdose (alone): Because they only work when GABA is present, there is a built-in ceiling to their CNS depressant effect. You cannot push the chloride channel beyond what GABA itself allows. This is their huge safety advantage over barbiturates.
Classification by Duration of Action
This is critical for clinical use:
| Duration | Half-life | Examples | Uses |
|---|
| Ultra-short | 2-6 hrs | Triazolam | Short-term insomnia |
| Short | 6-12 hrs | Oxazepam, Lorazepam, Temazepam | Anxiety, alcohol withdrawal, insomnia |
| Intermediate | 12-24 hrs | Alprazolam, Bromazepam | Panic disorder, GAD |
| Long | 24-72 hrs | Diazepam, Chlordiazepoxide, Clonazepam, Flurazepam | Anxiety, epilepsy, alcohol withdrawal, muscle spasm |
Mnemonic for SHORT-acting benzodiazepines (no active metabolites): "LOT"
- Lorazepam
- Oxazepam
- Temazepam
These are conjugated directly (glucuronidation) in the liver without going through oxidative metabolism. They are safe in liver disease, elderly, and neonates.
Long-acting benzodiazepines undergo hepatic CYP450 oxidation and often have active metabolites (e.g., diazepam → desmethyldiazepam → oxazepam). This prolonged action explains why hangover effects and accumulation occur, especially in elderly patients.
Pharmacokinetics
Absorption: Most benzodiazepines are well absorbed orally. Diazepam is rapidly absorbed (peak in 30-60 min). Some (lorazepam, midazolam) can be given IV, IM, or sublingually.
Distribution: Highly lipid-soluble → cross blood-brain barrier rapidly → rapid onset of action. They are highly protein-bound (85-99%).
Metabolism: Primarily hepatic. Short-acting ones (LOT) undergo glucuronidation. Long-acting ones undergo CYP450-mediated oxidation.
Elimination: Most are excreted in urine as glucuronide conjugates.
Volume of distribution: Large - they distribute extensively into fat stores. This is why obese patients and elderly patients may have prolonged effects.
Clinical Uses
| Clinical Use | Drug of Choice | Reasoning |
|---|
| Generalized Anxiety Disorder (GAD) | Diazepam, alprazolam | Broad anxiolysis |
| Panic Disorder | Alprazolam, clonazepam | High potency, anti-panic |
| Social Anxiety Disorder | Clonazepam, diazepam | Situational use |
| Insomnia (sleep onset) | Triazolam, temazepam | Short-acting, less hangover |
| Status Epilepticus | Diazepam IV, lorazepam IV | Rapid onset, anticonvulsant |
| Alcohol Withdrawal | Chlordiazepoxide, diazepam | Long-acting, prevents seizures |
| Muscle Spasm | Diazepam | Central muscle relaxant effect via α2/α3 |
| Preoperative sedation | Midazolam IV | Short-acting, causes anterograde amnesia (patient won't remember the procedure) |
| Acute agitation | Lorazepam IM | Reliable IM absorption |
| Eclampsia | Diazepam IV | Emergency anticonvulsant |
Adverse Effects (Linked to Mechanism)
| Adverse Effect | Why It Happens |
|---|
| Sedation, drowsiness | GABA enhancement in ascending arousal pathways |
| Impaired psychomotor coordination, ataxia (unsteady gait) | GABA enhancement in cerebellar and motor pathways (α2/α3 subunits) |
| Anterograde amnesia (cannot form new memories after taking the drug) | GABA enhancement in hippocampus (α5 subunits), impairing memory consolidation |
| Respiratory depression | GABA enhancement in brainstem respiratory centers - this is MILD with benzodiazepines alone but severe if combined with alcohol or opioids |
| Rebound anxiety/insomnia on stopping | The brain has adapted to more GABA signaling; when drug is removed, the now-sensitized excitatory systems take over |
| Paradoxical reactions (agitation, aggression) | Rare; seen especially in elderly and children; may involve disinhibition of frontal lobe control |
| Tolerance | Chronic use causes downregulation of GABA-A receptors and decreased sensitivity |
| Physical dependence | The brain compensates for GABA enhancement by reducing GABA sensitivity; when drug is removed, the brain is now GABA-deficient → withdrawal |
| Teratogenicity | Possible risk of cleft palate (Category D); avoid in first trimester |
| Fall risk in elderly | Sedation + ataxia + impaired reflexes |
Tolerance and Dependence - Explained in Full
Tolerance means the drug produces less effect over time, so you need more to achieve the same result.
Why tolerance develops:
Chronic benzodiazepine use leads to neuroadaptive changes:
- The brain senses that its GABA system is being boosted constantly
- It tries to compensate by downregulating (reducing the number of) GABA-A receptors
- It also changes subunit composition of GABA-A receptors to make them less sensitive to benzodiazepines
- Glutamate (excitatory) systems become upregulated to counterbalance
- The net result: you need more drug to get the same effect
Physical dependence:
When the drug is suddenly stopped after chronic use:
- The downregulated GABA system is now inadequate for normal inhibition
- The upregulated excitatory (glutamate) systems are now unopposed
- The result is a hyperexcitable brain state - the withdrawal syndrome
Benzodiazepine withdrawal syndrome:
Mild (first 1-3 days): rebound anxiety, insomnia, irritability, sweating
Moderate (days 2-7): tremors, nausea, palpitations
Severe (can occur): seizures, psychosis, delirium (rare but life-threatening)
- Short-acting benzodiazepines: withdrawal begins EARLIER and is more SEVERE
- Long-acting benzodiazepines: withdrawal begins LATER and is more GRADUAL
Treatment of withdrawal: Gradual tapering of the benzodiazepine dose, often with a long-acting benzodiazepine substituted for a short-acting one.
Important Drug Interactions
| Drug | Interaction | Result |
|---|
| Alcohol (ethanol) | CNS depressant synergy | Life-threatening respiratory depression |
| Opioids | CNS depressant synergy | Severe respiratory depression, death |
| Other CNS depressants | Additive depression | Enhanced sedation |
| Flumazenil | Competitive antagonist at BZ site | Reversal of benzodiazepine effects |
| CYP3A4 inhibitors (ketoconazole, ritonavir) | Reduced metabolism | Increased benzodiazepine levels and toxicity |
| CYP3A4 inducers (rifampicin, carbamazepine) | Increased metabolism | Reduced benzodiazepine effect |
| Cimetidine (H2 blocker) | Inhibits hepatic oxidation | Increased levels of oxidized benzodiazepines |
Critical exam point: The combination of benzodiazepines + opioids + alcohol is one of the most common causes of drug overdose death. Each drug alone can be survived; together they synergistically suppress the respiratory center.
Contraindications
- Myasthenia gravis - muscle weakness is worsened by muscle relaxation
- Sleep apnea - respiratory depression during sleep is dangerous
- Severe respiratory failure (COPD) - relative contraindication
- First trimester pregnancy - teratogenicity risk
- Acute narrow-angle glaucoma - some benzodiazepines increase intraocular pressure
- Acute alcohol intoxication - additive CNS depression
- History of drug abuse - high abuse potential
Benzodiazepine Overdose and Antidote: FLUMAZENIL
Flumazenil (Anexate, Romazicon):
- Competitive antagonist at the benzodiazepine binding site
- Does NOT have intrinsic agonist activity - just blocks BZ binding
- Reverses sedation, respiratory depression, and psychomotor impairment caused by benzodiazepines
- Also reverses Z-drug overdose (zolpidem, zaleplon)
- Given IV - works within 1-2 minutes
Half-life of flumazenil (~1 hour) is shorter than most benzodiazepines - patient may re-sedate after flumazenil wears off, requiring repeat dosing or monitoring
Critical warning: Do NOT use flumazenil in:
- Patients chronically on benzodiazepines for epilepsy → may precipitate seizures
- Patients who have co-ingested a pro-convulsant drug (e.g., tricyclic antidepressants) → same risk
- The reversal of benzodiazepine effect may unmask the convulsant effects of the co-ingestant
DRUG CLASS 2: BARBITURATES
Definition: Barbiturates are derivatives of barbituric acid (which is itself synthesized from urea and malonic acid). They are potent CNS depressants that work via GABA-A receptors.
Historical note: Barbiturates were the first class of synthetic sedative-hypnotics, introduced in the early 1900s (barbital 1903, phenobarbital 1912). They were widely used until benzodiazepines replaced them in the 1960s-1970s.
Mechanism of Action (Step by Step)
Step 1: Barbiturate binds to its own unique site on the GABA-A receptor (on β subunits - different from the BZ site)
Step 2: This makes the chloride channel stay open for a longer duration (prolongs channel opening time)
Step 3: More Cl- floods the cell → greater hyperpolarization → greater CNS depression
At high concentrations: Barbiturates can directly activate the chloride channel even without GABA being present. This is a critical difference from benzodiazepines.
Why barbiturates are more dangerous:
- No ceiling effect - they can independently open the Cl- channel
- At high enough doses, they cause fatal respiratory depression
- Therapeutic index is NARROW (small difference between therapeutic and lethal dose)
Classification
| Class | Duration | Examples |
|---|
| Ultra-short | 15-30 min | Thiopentone, methohexitone (IV anesthesia) |
| Short | 3-8 hrs | Pentobarbitone (discontinued in most countries) |
| Intermediate | 8-12 hrs | Amylobarbitone |
| Long | 12-24 hrs | Phenobarbitone (ONLY barbiturate still widely used clinically) |
Clinical Uses (Modern Day)
Barbiturates have largely been replaced by safer drugs. Current uses are limited:
- Phenobarbitone (phenobarbital): Epilepsy, especially in neonatal seizures and low-income settings where cost matters
- Thiopentone: IV induction of general anesthesia (rapid onset, ultra-short acting due to redistribution)
- Phenobarbitone: Neonatal jaundice (induces hepatic glucuronyl transferase → increases bilirubin conjugation)
Adverse Effects
| Adverse Effect | Mechanism |
|---|
| Profound CNS depression → coma, death | No ceiling effect, direct channel activation at high doses |
| Respiratory depression | Depression of brainstem respiratory center |
| Cardiovascular depression | Reduced myocardial contractility |
| Enzyme induction | Phenobarbitone is a potent CYP450 inducer (accelerates metabolism of many drugs including oral contraceptives, warfarin, phenytoin) |
| Tolerance and dependence (severe) | More severe than benzodiazepines; life-threatening withdrawal with seizures |
| Porphyria attack (CONTRAINDICATED in porphyria) | Induces ALA synthase → increases porphyrin synthesis |
| Hangover | Long-acting forms accumulate |
| Paradoxical excitement | In elderly, children, or pain conditions |
Benzodiazepines vs. Barbiturates - The Exam Table
| Feature | Benzodiazepines | Barbiturates |
|---|
| Mechanism at GABA-A | Increase frequency of Cl- channel opening | Increase duration of Cl- channel opening |
| Binding site | α-γ interface | β subunit (separate site) |
| Require GABA? | Yes (allosteric modulators only) | No (at high doses, act directly) |
| Therapeutic index | HIGH (safe in overdose alone) | LOW (dangerous in overdose) |
| Antidote | Flumazenil | No specific antidote (supportive only) |
| Dependence severity | Moderate | Severe |
| CYP450 induction | No | Yes (phenobarbitone) |
| Current clinical use | Anxiety, insomnia, epilepsy, alcohol withdrawal | Epilepsy (phenobarbitone only), anesthesia (thiopentone) |
| Analgesic properties | None | None |
DRUG CLASS 3: Z-DRUGS (Non-Benzodiazepine GABA-A Positive Allosteric Modulators)
Definition: Z-drugs are a group of chemically unrelated drugs that all bind to the same benzodiazepine binding site on the GABA-A receptor (the α-γ interface) but with relative selectivity for α1-containing receptor subunits. They are called "Z-drugs" simply because their generic names begin with the letter Z.
The main Z-drugs:
- Zolpidem (Ambien)
- Zaleplon (Sonata)
- Eszopiclone (Lunesta)
- Zopiclone (not available in the USA; racemic mixture)
Mechanism of Action
- Like benzodiazepines, Z-drugs bind to the BZ site (α-γ interface) on GABA-A receptors
- They increase the frequency of Cl- channel opening
- KEY DIFFERENCE: Z-drugs preferentially bind to GABA-A receptors containing the α1 subunit
- α1 subunits mediate primarily sedation and anterograde amnesia
- They have LESS effect on α2/α3 subunits (which mediate anxiolysis and muscle relaxation)
- Therefore: Z-drugs are primarily hypnotic with less anxiolytic and muscle-relaxant effect compared to benzodiazepines
- Like benzodiazepines, they are reversed by flumazenil
Pharmacokinetics Comparison
| Drug | Peak plasma (hrs) | Half-life | Active metabolites? | Feature |
|---|
| Zaleplon | 1 | 1 hour | No | Fastest; can be taken in the middle of the night if ≥4 hrs of sleep remain |
| Zolpidem | 1.6 | 2.6 hours | No | Standard hypnotic |
| Zolpidem CR | 1.5-3 | ~3 hours | No | Extended release; helps with both sleep onset and maintenance |
| Eszopiclone | 1 | ~6 hours | Weakly active | Longest acting; good for sleep maintenance insomnia |
Clinical Use
All Z-drugs are indicated only for insomnia - they are NOT used for anxiety, epilepsy, or muscle relaxation.
- Zaleplon: Sleep onset insomnia (very short half-life means no morning hangover)
- Zolpidem: Sleep onset insomnia (standard use); extended-release form for sleep maintenance
- Eszopiclone: Both sleep onset and sleep maintenance insomnia; can be used for up to 6 months
Advantages over benzodiazepines for insomnia:
- Less effect on sleep architecture (less REM and slow-wave sleep suppression)
- Less daytime sedation (shorter half-life)
- Less rebound insomnia on discontinuation
- Lower abuse potential (though still schedule IV controlled substances)
- No active metabolites (less accumulation in elderly)
Adverse Effects
| Adverse Effect | Notes |
|---|
| Somnolence, dizziness | Expected extension of pharmacological effect |
| Anterograde amnesia | Via α1 subunit effect on hippocampus |
| Complex sleep behaviors | Sleep-walking, sleep-driving, sleep-eating - patients have no memory of these; FDA black box warning |
| Bitter metallic taste | Classic with eszopiclone |
| Rebound insomnia on stopping | Milder than benzodiazepines |
| Dependence | Lower than benzodiazepines but possible with prolonged use |
DRUG CLASS 4: BUSPIRONE
Definition: Buspirone is an azapirone - a novel anxiolytic that works through serotonin receptors rather than GABA-A receptors. It is unique because it produces anxiolytic effects without sedation, dependence, or abuse potential.
Mechanism of Action
Buspirone does NOT bind to GABA-A receptors at all. This is a high-yield exam point.
Instead:
- Buspirone is a partial agonist at 5-HT1A receptors (serotonin receptors)
- It has high affinity for 5-HT1A receptors and moderate affinity for D2 (dopamine) receptors
- 5-HT1A receptors are found both on:
- Presynaptic neurons (where activation reduces serotonin release - autoreceptors)
- Postsynaptic neurons (where activation reduces anxiety responses)
- The net effect is a reduction in excessive serotonergic activity in anxiety circuits
Why the onset is slow: Because buspirone's effect on anxiety requires adaptive changes in serotonergic neurotransmission. This is NOT an immediate effect like a benzodiazepine. Onset takes 1-2 weeks (similar to antidepressants).
Key Features (The Exam Profile of Buspirone)
| Feature | Buspirone |
|---|
| Class | Azapirone |
| Mechanism | 5-HT1A partial agonist |
| Onset of anxiolysis | 1-2 weeks (delayed!) |
| Sedation | NO (non-sedating) |
| Muscle relaxation | NO |
| Anticonvulsant effect | NO |
| Dependence/abuse potential | NONE |
| Physical dependence | NONE |
| Withdrawal syndrome | NONE |
| Tolerance | NONE |
| Antidote | None needed (not a sedative) |
| Use in elderly | Safe (no fall risk) |
| Use in pregnancy | Relatively safer than benzodiazepines |
| Licensed indication | Generalized Anxiety Disorder (GAD) ONLY |
Clinical Use
- Generalized Anxiety Disorder (GAD) - first-line or second-line (after SSRIs)
- Particularly useful when: patient has history of substance abuse (no abuse potential), patient cannot tolerate sedation, long-term treatment is planned
- NOT effective for panic disorder, phobias, or acute anxiety (because of slow onset)
- Can be used as adjunctive treatment to SSRIs in depression
Adverse Effects
- Dizziness, nausea, headache (most common)
- Dysphoria (unpleasant feeling) in some patients
- Does NOT cause sedation, cognitive impairment, or psychomotor problems
- Does NOT interact with alcohol (very important point)
Why Buspirone Does Not Provide Immediate Relief
Analogy: Benzodiazepines are like a fire extinguisher - they immediately suppress the fire of anxiety. Buspirone is like fireproofing the walls - it takes time to remodel the building, but once done, the protection is more durable without side effects.
Patients who have previously taken benzodiazepines often feel that buspirone "doesn't work" because they are accustomed to the immediate sedative-anxiolytic effect. They must be counseled that the therapeutic effect takes 2 weeks.
DRUG CLASS 5: RAMELTEON (Melatonin Receptor Agonist)
Definition: Ramelteon is a selective agonist of melatonin MT1 and MT2 receptors. It is the only non-scheduled hypnotic drug in this class - meaning it has essentially NO abuse potential and is NOT a controlled substance.
Mechanism of Action
- Melatonin is produced by the pineal gland in response to darkness and signals the body that it is nighttime
- MT1 receptors: when activated, suppress neuronal firing in the suprachiasmatic nucleus (SCN) - the brain's master clock - promoting sleep onset
- MT2 receptors: involved in resetting circadian rhythms
- Ramelteon mimics melatonin by binding to MT1 and MT2 receptors
- It does NOT bind to GABA-A receptors at all
- This means: NO sedation, NO dependence, NO muscle relaxation, NO cognitive impairment
Key Features of Ramelteon
| Feature | Ramelteon |
|---|
| Mechanism | MT1/MT2 agonist |
| Indication | Sleep-onset insomnia |
| Effect on circadian rhythm | Yes (useful in jet lag, shift workers) |
| Controlled substance | NO |
| Dependence/abuse potential | None demonstrated |
| Withdrawal syndrome | None |
| Sedation | Minimal |
| Cognitive impairment | No |
| Dose | 8 mg at bedtime |
| Half-life | 1-2.6 hours |
| Metabolism | CYP1A2 (major) |
| Antidote | Not required |
Adverse Effects of Ramelteon
- Headache (most common)
- Somnolence, fatigue, dizziness (mild)
- Hormonal effects: increases prolactin, decreases testosterone and cortisol
- Monitor female patients for: loss of menstrual periods, galactorrhea (breast milk production), decreased libido
- Drug interaction: Fluvoxamine (a CYP1A2 inhibitor) dramatically increases ramelteon levels → increase in side effects
Contraindications
- Severe hepatic impairment (CYP1A2 metabolism impaired)
- Severe sleep apnea or severe COPD
- Pregnancy/lactation (insufficient safety data)
DRUG CLASS 6: SUVOREXANT (Orexin Receptor Antagonist)
Definition: Suvorexant is a dual orexin receptor antagonist (DORA) that blocks both orexin receptor subtypes (OX1R and OX2R). By blocking the wake-promoting orexin system, it allows sleep to naturally occur.
Mechanism of Action
- Orexin (also called hypocretin) is a neuropeptide produced in the lateral hypothalamus
- Orexin acts on OX1R and OX2R receptors throughout the brain's arousal centers:
- OX2R: strongly expressed in the histaminergic tuberomammillary nucleus (TMN) → promotes wakefulness via histamine
- OX1R: strongly expressed in the noradrenergic locus coeruleus → promotes alertness via NE
- Suvorexant blocks both OX1R and OX2R simultaneously
- Result: reduced arousal, facilitated transition to sleep
- This is a fundamentally different mechanism - instead of sedating the brain, it removes the wake drive
Analogy: Traditional hypnotics (benzodiazepines) press the "sleep" button forcibly. Suvorexant instead turns OFF the "wake" button. The result is more physiological sleep.
Key Features of Suvorexant
| Feature | Suvorexant |
|---|
| Brand name | Belsomra |
| Class | DORA (Dual Orexin Receptor Antagonist) |
| Indication | Insomnia (sleep onset AND sleep maintenance) |
| Schedule | IV controlled substance |
| Dose | 5-20 mg at bedtime |
| Half-life | ~12 hours |
| Mechanism | Blocks OX1R and OX2R |
| GABA involvement | None |
| Effect on sleep architecture | Preserves natural sleep stages |
| Contraindication | Narcolepsy (orexin is already deficient in narcolepsy - blocking it worsens symptoms) |
DRUG CLASS 7: SSRIs AND SNRIs AS FIRST-LINE ANXIOLYTICS
This is perhaps the most clinically important concept for modern practice that students miss on exams.
While benzodiazepines produce immediate anxiety relief, SSRIs (Selective Serotonin Reuptake Inhibitors) and SNRIs (Serotonin-Norepinephrine Reuptake Inhibitors) are now the first-line pharmacotherapy for most anxiety disorders due to their superior long-term safety profile.
Mechanism: SSRIs block the serotonin transporter (SERT), preventing serotonin reuptake. Over 2-4 weeks, this produces adaptive downregulation of 5-HT receptors and reduced activity in anxiety circuits.
| Anxiety Disorder | First-Line Drug(s) |
|---|
| GAD | SSRIs (sertraline, escitalopram), SNRIs (venlafaxine, duloxetine) |
| Panic Disorder | SSRIs (sertraline, paroxetine), SNRIs |
| Social Anxiety Disorder | SSRIs, SNRIs |
| PTSD | SSRIs (sertraline, paroxetine) - only FDA-approved for PTSD |
| OCD | SSRIs (fluvoxamine, fluoxetine) at HIGH doses |
Why SSRIs/SNRIs are preferred over benzodiazepines for long-term anxiety:
- No dependence or withdrawal syndrome
- No abuse potential
- Address depressive comorbidity (very common in anxiety disorders)
- Safe for long-term use
Disadvantage: Slow onset (2-4 weeks). Benzodiazepines are often used short-term while waiting for SSRI to work.
DRUG CLASS 8: HYDROXYZINE
Hydroxyzine (an antihistamine H1 blocker) has genuine anxiolytic properties:
- Mechanism: H1 receptor antagonism in limbic areas → sedation and anxiolysis
- Also has anticholinergic properties
- Used for short-term anxiety, especially procedural anxiety
- Advantage: No dependence, not a controlled substance
- Disadvantage: Sedating, anticholinergic side effects (dry mouth, urinary retention, constipation)
DRUG CLASS 9: BETA-BLOCKERS FOR SITUATIONAL ANXIETY
Propranolol (non-selective beta-blocker) is used for performance anxiety (stage fright):
- Does NOT reduce psychological anxiety
- Blocks peripheral adrenergic symptoms: tremor, palpitations, sweating
- Taken 30-60 minutes before a performance/examination
- Not used for continuous anxiety treatment
DRUG CLASS 10: BARBITURATES AND OLDER DRUGS (Historical/Comparison)
Chloral hydrate:
- Reduces rapidly to trichloroethanol (active)
- Barbiturate-like effects on GABA-A
- Historical use: "knockout drops" (Mickey Finn)
- Now rarely used; may be used for paradoxical benzodiazepine reactions
Meprobamate:
- First "minor tranquilizer" marketed (1955)
- Replaced by benzodiazepines
- Still a schedule IV drug
- Low therapeutic index; abuse potential
Clomethiazole (chlormethiazole):
- GABA-A modulator
- Used for alcohol withdrawal delirium in hospitalized patients
- Risk of respiratory depression; must be used in hospital setting
SECTION 4: TEACH USING ANALOGIES
Analogy 1: Benzodiazepines - The Dimmer Switch
Your brain's electrical activity is like the lighting in a room. Normally, there is an optimal level of brightness. In anxiety, the lights are on full blast. In insomnia, the lights refuse to dim.
The GABA system is the dimmer switch. GABA turns down the brightness. But in anxiety, the dimmer switch doesn't respond well enough.
Benzodiazepines are like an engineer who makes the dimmer switch 10 times more sensitive. Now, when you barely touch the switch (GABA is released), the room dims dramatically. The brain becomes quiet, and the person relaxes and sleeps.
But here's the catch: if you always use this supercharged dimmer switch, the room's electrical system adapts by installing brighter bulbs (the brain's excitatory systems upregulate). Now you NEED the engineer (benzodiazepine) just to get back to normal. That's dependence.
Analogy 2: Barbiturates - The Override Switch
Benzodiazepines only make the dimmer switch more sensitive - they still need someone to use the switch (GABA must be present). Barbiturates are different - at high doses, they can just physically force the switch off themselves, even with no hand on it (they directly activate the channel). This makes them far more dangerous - there's no built-in safety limit.
Analogy 3: Buspirone - The Long-Term Renovation
Imagine your anxiety is caused by an alarm system that triggers unnecessarily. Benzodiazepines are like cutting the power to the whole building - immediate silence, but now nothing works properly. Buspirone is like calling an electrician who carefully rewires the alarm system over 2 weeks, so it no longer gives false alarms. Slower, but much more targeted.
Analogy 4: Suvorexant - The Off Switch for Wakefulness
Your brain has both a "go to sleep" button and a "stay awake" button. Most hypnotics press the "go to sleep" button harder. Suvorexant removes the battery from the "stay awake" button. Both approaches help you sleep, but suvorexant's approach feels more natural because it's not forcing sleep - it's just removing the obstacle to sleep.
Analogy 5: Z-drugs - The Precision Tool vs. the Sledgehammer
Benzodiazepines are like a sledgehammer - they affect every GABA-A receptor subtype (α1, α2, α3, α5) and produce sedation, anxiolysis, muscle relaxation, amnesia all at once. Z-drugs (like zolpidem) are like a precision screwdriver that only fits the α1-containing receptors - you get the sleep effect with less of the other effects. Better for insomnia, but not useful for anxiety.
Analogy 6: Tolerance and Dependence - The Thermostat Analogy
Your brain is like a house with a thermostat set to 70°F (normal anxiety level). Benzodiazepines are like turning on the air conditioning (adding GABA). The house cools down (patient is less anxious). But if the air conditioning runs constantly for months, the thermostat adjusts itself to work at 70°F WITH the air conditioning. Now if you suddenly turn off the air conditioning, the thermostat has no idea what to do - the house overheats catastrophically (withdrawal syndrome - anxiety, seizures, panic).
SECTION 5: STEP-BY-STEP CLINICAL REASONING
Case 1: The Anxious Professional
Patient: 35-year-old lawyer presenting with 6 months of excessive worry about work, difficulty concentrating, muscle tension, irritability, and sleep difficulties. No substance use. No history of depression. Requests "something for nerves."
Step 1: What type of anxiety is this?
The 6-month duration, generalized nature, and multiple somatic symptoms (muscle tension, sleep disturbance, concentration difficulties) point to Generalized Anxiety Disorder (GAD).
Step 2: What is the first-line treatment?
For GAD, first-line pharmacotherapy = SSRI or SNRI (e.g., sertraline 50 mg daily or venlafaxine 37.5-75 mg daily).
Cognitive Behavioral Therapy (CBT) should also be recommended.
Step 3: Can I use a benzodiazepine?
Benzodiazepines can be used SHORT-TERM (2-4 weeks maximum) while waiting for the SSRI to take effect. They are NOT appropriate as sole long-term treatment due to dependence risk.
Step 4: What if SSRIs are not tolerated?
Buspirone 5-10 mg three times daily is an alternative - no dependence, no sedation, but takes 2 weeks.
Step 5: What about sleep difficulties?
If sleep is a dominant complaint: a low-dose benzodiazepine (temazepam at night) or a Z-drug (zolpidem 5-10 mg at night) can be added short-term. Long-term: sleep hygiene, CBT for insomnia (CBT-I) are preferred.
Case 2: The Acute Panic Attack
Patient: 28-year-old woman brought to emergency department with sudden onset of pounding heart, shortness of breath, sweating, dizziness, and feeling of impending doom. Medical causes excluded. Previous episodes documented.
Step 1: What is this?
Panic Disorder - recurrent panic attacks with anticipatory anxiety about future attacks.
Step 2: Acute management?
For an acute panic attack: Lorazepam (1-2 mg oral or IM) or diazepam (5-10 mg) - rapid anxiolytic relief.
Step 3: Long-term pharmacotherapy?
SSRIs are first-line for panic disorder. Paroxetine and sertraline are FDA-approved for panic disorder. Begin at low dose (start low, go slow - SSRIs can temporarily worsen anxiety in the first 1-2 weeks of treatment due to initial serotonin surge - a "jitteriness syndrome").
Step 4: Role of benzodiazepines long-term in panic?
High-potency benzodiazepines (alprazolam, clonazepam) can be used as adjuncts but not as monotherapy long-term. The risk of dependence in panic disorder is notable.
Case 3: The Insomniac Elderly Patient
Patient: 72-year-old man with difficulty falling asleep and frequent nighttime awakenings for 3 months. History of mild COPD. Takes multiple medications.
Step 1: What type of insomnia?
Mixed - both sleep onset and sleep maintenance insomnia.
Step 2: Non-pharmacological first?
CBT-I (Cognitive Behavioral Therapy for Insomnia) is the FIRST-LINE treatment for chronic insomnia in any patient, regardless of age. This includes: sleep restriction therapy, stimulus control, relaxation training, sleep hygiene education.
Step 3: If pharmacotherapy needed - which drug?
- Avoid long-acting benzodiazepines (diazepam, flurazepam) in elderly - accumulate, increase fall risk, cognitive impairment
- Ramelteon 8 mg - safest option; no dependence, no cognitive impairment, no respiratory depression, not a controlled substance
- Doxepin 3-6 mg (low-dose tricyclic antidepressant) - FDA-approved for sleep maintenance insomnia; minimal side effects at low doses
- Suvorexant - option for both onset and maintenance; avoid due to 12-hour half-life causing morning hangover in elderly
- Avoid benzodiazepines and Z-drugs in elderly due to fall risk, cognitive impairment (Beers Criteria)
Step 4: COPD consideration?
Avoid benzodiazepines and barbiturates - respiratory depression risk. Ramelteon is preferred.
Case 4: Alcohol Withdrawal
Patient: 50-year-old chronic alcohol user admitted with tremors, agitation, sweating, and elevated blood pressure 24 hours after stopping alcohol.
Step 1: Why is this happening?
Alcohol (like benzodiazepines) enhances GABA-A receptor function. Chronic use leads to GABA-A downregulation and glutamate (NMDA receptor) upregulation. When alcohol is stopped, the now-hyperexcitable brain causes the withdrawal syndrome.
Step 2: First-line treatment?
Long-acting benzodiazepines - typically chlordiazepoxide (Librium) or diazepam:
- Stabilize the GABA system
- Prevent progression to delirium tremens (DT) and withdrawal seizures
- Dose is titrated based on severity (CIWA-Ar score)
Step 3: Why long-acting?
Long-acting benzodiazepines provide a smooth, self-tapering effect as they are metabolized slowly. Short-acting ones require more frequent dosing and carry more breakthrough seizure risk.
Step 4: Alternative in liver disease?
If hepatic function is severely impaired, use lorazepam or oxazepam (undergo glucuronidation only, not oxidative metabolism → safer in liver failure).
SECTION 6: MEMORY TOOLS
Mnemonic 1: SHORT-ACTING BENZODIAZEPINES - "LOT"
Lorazepam - Oxazepam - Temazepam
These three are conjugated directly (not oxidized), making them safe in hepatic impairment, elderly, and neonates.
Mnemonic 2: BENZODIAZEPINE CLINICAL USES - "ASAM"
A - Anti-Anxiety (GAD, panic, social phobia)
S - Seizures (status epilepticus, epilepsy - clonazepam)
A - Alcohol withdrawal (chlordiazepoxide, diazepam)
M - Muscle relaxation / anesthesia premedication
Mnemonic 3: BUSPIRONE FEATURES - "NO SLAM"
Not sedating
Onset delayed (1-2 weeks)
Serotonin 5-HT1A partial agonist
Long-term use is safe
Absolutely no dependence
Mostly for GAD
Mnemonic 4: BARBITURATE VS BENZODIAZEPINE MECHANISM
"Barbiturates make the door STAY open (Duration)"
"Benzodiazepines make the door open more FREQUENTLY (Frequency)"
- Barbiturate = Duration (B-D)
- Benzodiazepine = Frequency (B-F)
Mnemonic 5: CONTRAINDICATIONS TO BENZODIAZEPINES - "MAPS"
M - Myasthenia gravis
A - Acute narrow-angle glaucoma
P - Porphyria (well, that's barbiturates - note the difference!)
S - Sleep apnea
Mnemonic 6: RAMELTEON - "3 No's"
- No GABA (doesn't touch GABA-A receptors)
- No dependence
- No scheduled status (not a controlled substance)
Mnemonic 7: Z-DRUGS Half-Lives (Shortest to Longest)
"Zaleplon is Zapping fast" (t½ = 1 hour)
"Zolpidem is somewhere in the Zone" (t½ = 2.6 hours)
"Eszopiclone goes the Extra mile" (t½ = 6 hours)
Memory Story: The Brain's Peace Treaty
Once upon a time, the brain was in a constant war between the EXCITATORY forces (Glutamate's army) and the INHIBITORY forces (GABA's army). In anxiety, Glutamate was winning.
The King (prefrontal cortex) called in reinforcements. He hired:
- The BENZODIAZEPINE mercenaries - they went straight to GABA's headquarters and made every GABA soldier open fire 3x more often (frequency of Cl- channel opening). Peace returned quickly. But the mercenaries were addictive - they stayed too long and the army became dependent on them.
- The BARBITURATE heavy artillery - they made GABA's doors stay open forever (duration). Effective, but so powerful they sometimes destroyed their own side (no ceiling effect - deaths in overdose).
- BUSPIRONE, the diplomat - he didn't fight directly. Instead, he went to the Serotonin Department and negotiated a long-term peace treaty. It took 2 weeks to sign, but it was more durable.
- SUVOREXANT, the peace-keeper - he didn't increase GABA but instead dismantled OREXIN's weapons (wake-promoting signals). Without Orexin's alarm sirens, the brain naturally settled into sleep.
- RAMELTEON, the night watchman - he simply rang the melatonin bell signaling nighttime, and the brain's master clock set itself to sleep mode.
Drug Comparison Table: All Hypnotics at a Glance
| Drug/Class | Mechanism | Onset | Duration | Dependence | Main Use |
|---|
| Diazepam | GABA-A (BZ site) - frequency ↑ | Fast | Long | Moderate | Anxiety, alcohol withdrawal |
| Lorazepam | GABA-A (BZ site) - frequency ↑ | Fast | Short | Moderate | Acute anxiety, status epilepticus |
| Midazolam | GABA-A (BZ site) - frequency ↑ | Very fast | Ultra-short | Low | IV sedation, anesthesia |
| Phenobarbitone | GABA-A (β site) - duration ↑ | Slow | Long | Severe | Epilepsy |
| Thiopentone | GABA-A (β site) - duration ↑ | IV: seconds | Ultra-short | Moderate | Anesthesia induction |
| Zolpidem | GABA-A α1 (BZ site) | Fast | Short | Low-moderate | Insomnia (onset) |
| Zaleplon | GABA-A α1 (BZ site) | Fast | Very short | Low | Insomnia (onset) |
| Eszopiclone | GABA-A α1 (BZ site) | Fast | Intermediate | Low | Insomnia (onset+maintenance) |
| Buspirone | 5-HT1A partial agonist | Slow (2 weeks) | - | NONE | GAD only |
| Ramelteon | MT1/MT2 agonist | Fast | Short | NONE | Insomnia (onset, circadian) |
| Suvorexant | OX1R/OX2R antagonist | Fast | Intermediate | Low | Insomnia (onset+maintenance) |
| SSRIs | SERT blockade | Slow (2-4 weeks) | - | None | All anxiety disorders (1st line) |
| Propranolol | β-adrenergic blockade (peripheral) | Fast | Short | None | Performance anxiety |
| Hydroxyzine | H1 antagonist | Fast | Intermediate | None | Short-term anxiety |
SECTION 7: EXAMINER'S CORNER
Most Tested Facts
- Benzodiazepine mechanism: Increases frequency of Cl- channel opening via GABA-A BZ site (α-γ interface)
- Barbiturate mechanism: Increases duration of Cl- channel opening via GABA-A β subunit site
- Why benzodiazepines are safer than barbiturates in overdose: Benzodiazepines require GABA to be present (ceiling effect); barbiturates can directly activate the channel at high doses
- Antidote for benzodiazepine overdose: Flumazenil (competitive antagonist at BZ site)
- Flumazenil caution: Do NOT give in patients chronically on benzodiazepines for epilepsy → seizures
- Buspirone: 5-HT1A partial agonist; no GABA activity; no sedation; no dependence; slow onset 2 weeks; GAD only
- Z-drugs: Selective for α1 subunit → primarily sedative-hypnotic only; reversed by flumazenil
- Eszopiclone side effect: Bitter metallic taste
- Ramelteon: MT1/MT2 agonist; not a controlled substance; no dependence; metabolized by CYP1A2; fluvoxamine increases its levels
- Suvorexant: Orexin (OX1/OX2) antagonist; contraindicated in narcolepsy
- Short-acting benzodiazepines (LOT): Lorazepam, Oxazepam, Temazepam - undergo glucuronidation, safe in liver disease
- Benzodiazepine withdrawal: Hyperexcitable state - anxiety, tremors, seizures (can be fatal); treat with gradual taper
- Alcohol withdrawal treatment: Chlordiazepoxide or diazepam; use lorazepam/oxazepam in liver disease
- First-line for anxiety disorders (long-term): SSRIs/SNRIs, not benzodiazepines
Most Likely Essay Questions
-
"Classify benzodiazepines. Describe the mechanism of action, pharmacological effects, therapeutic uses, and adverse effects of benzodiazepines. Compare them with barbiturates."
-
"Discuss the pharmacological management of anxiety. What is the role of benzodiazepines, buspirone, and SSRIs?"
-
"Write a note on: GABA-A receptor and its modulation by sedative-hypnotic drugs."
-
"A 45-year-old chronic alcoholic is admitted with agitation, tremors, and autonomic instability 36 hours after his last drink. Discuss the pharmacological management."
-
"Discuss the pharmacology of buspirone. How does it differ from benzodiazepines?"
Most Likely Short Notes
- Flumazenil
- Buspirone
- Ramelteon
- Z-drugs (non-benzodiazepine hypnotics)
- Benzodiazepine withdrawal
- Pharmacology of zolpidem
- Tolerance and dependence to benzodiazepines
- Comparison of barbiturates and benzodiazepines
Most Likely Viva Questions
- "What is the mechanism of action of benzodiazepines at a molecular level?"
- "Why are benzodiazepines safer than barbiturates in overdose?"
- "What is flumazenil? Why must you be careful using it?"
- "Why does buspirone take 2 weeks to work?"
- "Name three benzodiazepines safe to use in liver disease and why."
- "What is the difference between suvorexant and zolpidem?"
- "Why is ramelteon not a controlled substance?"
- "Explain benzodiazepine tolerance at a receptor level."
Most Likely MCQs (with answers and traps)
MCQ 1: A drug increases the frequency of chloride channel opening at the GABA-A receptor. It is:
A) Barbiturate
B) Benzodiazepine ← CORRECT
C) Flumazenil
D) Buspirone
Trap: Students confuse frequency (benzodiazepines) with duration (barbiturates).
MCQ 2: A 26-year-old man with epilepsy on clonazepam takes an overdose of diazepam. Which drug must NOT be used to reverse the effects?
A) Activated charcoal
B) Flumazenil ← CORRECT - must NOT use
C) IV fluids
D) Airway support
Trap: Flumazenil is the antidote for BZ overdose BUT is contraindicated in epileptic patients on chronic benzodiazepines as it precipitates seizures.
MCQ 3: Which benzodiazepine is safest in a patient with cirrhosis?
A) Diazepam
B) Chlordiazepoxide
C) Lorazepam ← CORRECT
D) Flurazepam
Trap: Only LOT drugs (Lorazepam, Oxazepam, Temazepam) are safe in liver disease.
MCQ 4: A new anxiolytic has been prescribed. The patient calls 10 days later saying it isn't working. The most likely drug is:
A) Diazepam
B) Buspirone ← CORRECT
C) Lorazepam
D) Alprazolam
Trap: Students forget buspirone's 1-2 week onset. Patient needs counseling that this is expected.
MCQ 5: Which insomnia drug is NOT a controlled substance?
A) Zolpidem
B) Zaleplon
C) Temazepam
D) Ramelteon ← CORRECT
Trap: All GABA-A modulators are scheduled; only ramelteon (melatonin receptor agonist) is non-scheduled.
MCQ 6: Bitter metallic taste is a classic side effect of:
A) Zolpidem
B) Zaleplon
C) Eszopiclone ← CORRECT
D) Ramelteon
MCQ 7: Which drug directly activates GABA-A chloride channel at high doses WITHOUT requiring GABA?
A) Benzodiazepine
B) Barbiturate ← CORRECT
C) Z-drug
D) Buspirone
MCQ 8: The antidote to benzodiazepine overdose is:
A) Naloxone (opioid antidote)
B) N-acetylcysteine (paracetamol antidote)
C) Flumazenil ← CORRECT
D) Atropine
MCQ 9: Which drug is used for alcohol withdrawal in a patient with severe hepatic cirrhosis?
A) Diazepam
B) Chlordiazepoxide
C) Oxazepam ← CORRECT
D) Flurazepam
MCQ 10: A 52-year-old male with narcolepsy develops insomnia. Which drug is CONTRAINDICATED?
A) Zolpidem
B) Ramelteon
C) Suvorexant ← CORRECT - CONTRAINDICATED in narcolepsy
D) Temazepam
Trap: Suvorexant blocks orexin. Narcolepsy is caused by orexin deficiency. Blocking orexin further would worsen narcolepsy catastrophically.
Common Traps Students Fall Into
| Trap | Correct Fact |
|---|
| "Benzodiazepines open the Cl- channel directly" | NO - they only enhance GABA's effect on the channel |
| "Barbiturates have the same mechanism as benzodiazepines" | NO - different binding sites; barbiturates can directly activate channel |
| "Buspirone is a fast-acting anxiolytic" | NO - onset is 1-2 weeks |
| "Flumazenil can always be used in benzodiazepine overdose" | NO - contraindicated in epileptic patients on chronic BZ |
| "Z-drugs have no abuse potential" | They are Schedule IV controlled substances; abuse is possible |
| "Ramelteon is like a benzodiazepine but better" | NO - completely different mechanism (melatonin receptors, not GABA-A) |
| "Benzodiazepines are the first-line for chronic anxiety" | NO - SSRIs/SNRIs are first-line; benzodiazepines are adjuncts only |
| "Diazepam is safe in liver disease" | NO - it requires oxidative metabolism; use LOT drugs instead |
| "Suvorexant works by enhancing GABA" | NO - it blocks orexin receptors (completely different mechanism) |
SECTION 9: HIGH-YIELD REVISION SHEET
╔══════════════════════════════════════════════════════════════╗
║ DRUG TREATMENT OF ANXIETY & INSOMNIA - RAPID REVIEW ║
╠══════════════════════════════════════════════════════════════╣
║ GABA-A RECEPTOR: Pentameric (2α + 2β + 1γ); Cl- channel ║
║ BZ SITE: α-γ interface; Benzodiazepines + Z-drugs bind here ║
║ BARBITURATE SITE: β subunit; separate from BZ site ║
╠══════════════════════════════════════════════════════════════╣
║ BENZODIAZEPINES ║
║ • Mechanism: ↑ FREQUENCY of Cl- channel opening (+ GABA) ║
║ • Uses: Anxiety, insomnia, epilepsy, alcohol withdrawal, ║
║ muscle spasm, anesthesia premedication ║
║ • LOT = Safe in liver disease (glucuronidation only) ║
║ L=Lorazepam, O=Oxazepam, T=Temazepam ║
║ • Antidote: Flumazenil (BZ competitive antagonist) ║
║ • CAUTION: Flumazenil → seizures in epileptic/BZ-dependent ║
║ • Contraindicated: Sleep apnea, myasthenia gravis ║
╠══════════════════════════════════════════════════════════════╣
║ BARBITURATES ║
║ • Mechanism: ↑ DURATION of Cl- channel opening ║
║ (at high doses: DIRECT activation, no GABA needed) ║
║ • No ceiling effect → DANGEROUS in overdose ║
║ • No antidote (supportive care only) ║
║ • Phenobarbitone: strong CYP450 inducer ║
║ • Contraindicated: Porphyria ║
╠══════════════════════════════════════════════════════════════╣
║ Z-DRUGS (Zolpidem, Zaleplon, Eszopiclone) ║
║ • Mechanism: Selective α1-GABA-A → sedation > anxiolysis ║
║ • Reversed by flumazenil ║
║ • Half-lives: Zaleplon(1h) < Zolpidem(2.6h) < Eszo(6h) ║
║ • Eszopiclone: bitter taste ║
║ • Complex sleep behaviors (FDA black box warning) ║
╠══════════════════════════════════════════════════════════════╣
║ BUSPIRONE ║
║ • 5-HT1A partial agonist ║
║ • NO GABA activity; NO sedation; NO dependence ║
║ • Onset: 1-2 WEEKS ║
║ • Use: GAD only; NOT panic, NOT phobias ║
╠══════════════════════════════════════════════════════════════╣
║ RAMELTEON ║
║ • MT1/MT2 agonist ║
║ • Not scheduled (no abuse potential) ║
║ • Insomnia + circadian rhythm disorders ║
║ • Metabolized by CYP1A2; fluvoxamine ↑ its levels ║
║ • ADR: ↑ prolactin, ↓ testosterone ║
╠══════════════════════════════════════════════════════════════╣
║ SUVOREXANT ║
║ • Dual orexin receptor antagonist (OX1 + OX2) ║
║ • Contraindicated in NARCOLEPSY ║
║ • Schedule IV controlled substance ║
╠══════════════════════════════════════════════════════════════╣
║ SSRIs/SNRIs = FIRST-LINE for most chronic anxiety disorders ║
║ Propranolol = Performance anxiety (peripheral symptoms only) ║
║ Hydroxyzine = Short-term anxiety (H1 blocker, not scheduled) ║
╠══════════════════════════════════════════════════════════════╣
║ ALCOHOL WITHDRAWAL: Diazepam/Chlordiazepoxide ║
║ ALCOHOL WITHDRAWAL + LIVER DISEASE: Lorazepam/Oxazepam ║
╚══════════════════════════════════════════════════════════════╝
SECTION 10: SELF-ASSESSMENT
10 Short-Answer Questions (with Full Explanations)
Q1. Explain the molecular mechanism by which benzodiazepines exert their anxiolytic effect. How does this differ from barbiturates?
Answer:
Benzodiazepines bind to a specific allosteric site on the GABA-A receptor located at the interface between the α and γ subunits (the "benzodiazepine site"). This binding does not open the chloride channel itself but rather changes the shape of the receptor in a way that makes it more responsive to GABA. When GABA binds (at its own α-β interface sites), the chloride channel now opens more frequently than it would without the benzodiazepine present. More frequent Cl- entry causes greater neuronal hyperpolarization and reduced firing, producing CNS depression, anxiolysis, and sedation.
Barbiturates bind to a completely different site on the GABA-A receptor (on β subunits). Rather than increasing the frequency of channel opening, barbiturates increase the duration of each channel opening event. At high concentrations, barbiturates can even activate the channel directly without GABA being present. This lack of a ceiling effect makes barbiturates far more dangerous in overdose than benzodiazepines.
Q2. Why is flumazenil contraindicated in a patient with epilepsy who has overdosed on benzodiazepines?
Answer:
Flumazenil is a competitive antagonist at the benzodiazepine binding site on GABA-A receptors. In a patient with epilepsy who is chronically dependent on benzodiazepines (e.g., clonazepam for seizure control), their brain has adapted to the constant presence of benzodiazepine activity. If flumazenil is administered, it competitively displaces the benzodiazepine from the receptor, suddenly removing the enhanced GABA inhibitory tone. The now-hyperexcitable brain (which has down-regulated its own GABA responses to compensate for chronic benzodiazepine use) may not have adequate inhibitory reserve, resulting in withdrawal seizures. Therefore, flumazenil is contraindicated (or used with extreme caution) in epileptic patients chronically on benzodiazepines.
Q3. A patient who has been taking diazepam for 6 months for anxiety wants to stop. Explain the withdrawal syndrome and how you would manage it.
Answer:
Chronic benzodiazepine use causes neuroadaptation: the GABA-A receptors are downregulated (fewer receptors, reduced sensitivity) and the opposing glutamate (NMDA) excitatory system is upregulated. When diazepam is abruptly stopped, the brain has insufficient GABA inhibitory capacity to counterbalance the now-dominant excitatory system. This produces a hyperexcitable withdrawal state characterized by:
- Rebound anxiety, insomnia, irritability (early)
- Tremors, sweating, palpitations, nausea
- Seizures (severe cases)
- Rarely: delirium tremens-like picture
Management:
- Never abruptly stop - this is dangerous
- Gradual tapering of diazepam (10% dose reduction every 1-2 weeks)
- If the patient was on a short-acting benzodiazepine, switch to diazepam (long-acting) first, then taper diazepam more smoothly
- Adjunct: propranolol for autonomic symptoms; anticonvulsants if seizure risk is high
- Psychological support and CBT are essential
Q4. Compare and contrast buspirone with diazepam for the treatment of GAD. In what clinical situations would you prefer one over the other?
Answer:
| Feature | Diazepam | Buspirone |
|---|
| Mechanism | GABA-A BZ site agonist | 5-HT1A partial agonist |
| Onset | Immediate (minutes) | 1-2 weeks |
| Sedation | Yes | No |
| Muscle relaxation | Yes | No |
| Dependence | Yes | No |
| Abuse potential | Yes | No |
| Antidote | Flumazenil | Not needed |
Choose diazepam when:
- Rapid relief is needed (acute anxiety episode)
- Short-term use only (max 2-4 weeks)
- Patient needs muscle relaxation (e.g., associated muscle tension)
Choose buspirone when:
- Long-term treatment is planned
- Patient has history of substance abuse or dependence
- Patient cannot tolerate sedation (e.g., operates machinery, drives)
- Patient requires a non-sedating option
- Elderly patient (no fall risk with buspirone)
Q5. A 68-year-old woman with mild COPD and chronic insomnia asks for a sleeping tablet. She is on no other medications. What would you prescribe and why? What would you avoid and why?
Answer:
Prescribe: Ramelteon 8 mg at bedtime.
Reasoning:
- No respiratory depression (no effect on GABA-A; melatonin receptor agonist)
- No dependence or abuse potential (not a controlled substance)
- No fall risk (no sedation, no psychomotor impairment)
- Safe for elderly
- Appropriate for sleep-onset insomnia
Avoid:
- Benzodiazepines - respiratory depression in COPD; fall risk in elderly; dependence
- Barbiturates - severe respiratory depression, dangerous narrow therapeutic index
- Z-drugs (zolpidem) - still have some respiratory depression potential, fall risk, cognitive impairment in elderly (Beers Criteria)
- Suvorexant - 12-hour half-life; morning sedation; fall risk
Also note: Before ANY pharmacotherapy, CBT-I (Cognitive Behavioral Therapy for Insomnia) should be the first-line recommendation.
Q6. What is the significance of GABA-A receptor subunit composition in determining the clinical effects of benzodiazepines vs. Z-drugs?
Answer:
The GABA-A receptor exists in multiple isoforms depending on the combination of subunits assembled. The α subunit type is particularly important:
- α1 subunits → mediate sedation, anterograde amnesia, and some anticonvulsant effects
- α2 and α3 subunits → mediate anxiolytic effects, muscle relaxation
- α5 subunits → mediate memory (hippocampal) effects
Benzodiazepines are non-selective - they bind to GABA-A receptors containing α1, α2, α3, and α5 subunits. This produces the full spectrum of effects: sedation, anxiolysis, muscle relaxation, anticonvulsant action, and amnesia simultaneously.
Z-drugs (especially zolpidem and zaleplon) are selective for α1-containing GABA-A receptors. Since α1 primarily mediates sedation and hypnosis, Z-drugs are primarily hypnotic agents with:
- Less anxiolytic effect (α2/α3 not engaged)
- Less muscle relaxation (α2/α3 not engaged)
- Less anticonvulsant effect
- Primarily sedative/sleep-promoting effect
This is why Z-drugs are used for insomnia but not for anxiety or epilepsy.
Q7. A patient presents in status epilepticus. Which benzodiazepine would you use and by which route? Explain your choice.
Answer:
First-line: Intravenous lorazepam (0.1 mg/kg, maximum 4 mg IV) - OR diazepam IV (0.15-0.2 mg/kg)
Choice reasoning:
- IV route ensures rapid onset (reaches brain in 1-2 minutes)
- Lorazepam: High potency, intermediate duration (less likely to cause prolonged respiratory depression than diazepam), more predictable kinetics for IV use
- Diazepam IV: Also effective and widely available; however, has a long active metabolite chain (desmethyldiazepam) which prolongs sedation
- If IV access unavailable: diazepam rectally (rectal diazepam solution) or midazolam intramuscularly/intranasally/buccally is an alternative
Mechanism in status epilepticus:
Seizures involve excessive synchronized neuronal firing. Benzodiazepines enhance GABA inhibition throughout the brain, including in the seizure focus and in secondary generalization pathways, rapidly stopping the seizure.
Q8. Explain why phenobarbitone is still used in clinical practice despite being replaced by safer drugs for most indications. What are the specific clinical scenarios where it remains the drug of choice?
Answer:
Phenobarbitone remains clinically relevant for specific reasons:
Clinical scenarios where it is still used:
-
Neonatal seizures: Phenobarbitone is the drug of choice for neonatal seizures (first 28 days of life). It can be given IV rapidly and has well-established safety data in neonates.
-
Epilepsy in resource-limited settings: Phenobarbitone is highly effective, extremely inexpensive, and widely available. The WHO includes it on the Essential Medicines List for epilepsy.
-
Neonatal jaundice: Phenobarbitone induces hepatic CYP450 enzymes AND uridine-glucuronyl transferase, increasing conjugation and clearance of bilirubin. Used as a preventive measure in certain cases of neonatal hyperbilirubinemia.
-
Febrile convulsions (prophylaxis): No longer recommended routinely, but historically used.
-
Induction of anesthesia: Thiopentone (ultra-short barbiturate) is still used for rapid sequence induction of anesthesia where propofol is unavailable.
Q9. Describe the pharmacological basis of why the combination of benzodiazepines + opioids + alcohol is potentially fatal.
Answer:
Each of these three substances independently depresses the central nervous system, particularly the respiratory centers in the brainstem. However, their combination produces synergistic (greater than additive) CNS depression:
Mechanism of each:
- Benzodiazepines → enhance GABA-A receptor activity → increase inhibitory tone in brainstem respiratory neurons → reduce respiratory drive
- Opioids → act at mu-opioid receptors on brainstem pre-Bötzinger complex neurons (the respiratory rhythm generator) → directly suppresses the rate and depth of breathing
- Alcohol (ethanol) → enhances GABA-A (similar mechanism to benzodiazepines) AND inhibits NMDA glutamate receptors → dual suppression of brainstem activity
Combined effect:
All three converge on brainstem respiratory centers via different but complementary mechanisms. The inhibitory signaling becomes overwhelming → respiratory rate drops below the threshold needed for survival → hypoxia → death.
Additionally, all three suppress protective airway reflexes, increasing the risk of aspiration pneumonia, which further compromises oxygenation.
This combination is the leading cause of prescription drug overdose deaths globally.
Q10. A patient tells you "I've heard that if you take sleeping tablets every night for a month, they stop working - is that true?" Explain the pharmacological basis of tolerance to benzodiazepines and suggest a management approach.
Answer:
The patient is correct - pharmacological tolerance does develop with chronic benzodiazepine (and Z-drug) use.
Pharmacological basis:
- Receptor downregulation: The brain senses chronically elevated GABA-A receptor activity (from the drug's presence) and responds by:
- Reducing the total number of GABA-A receptors (receptor downregulation)
- Changing the subunit composition of receptors to make them less responsive to benzodiazepines
- Receptor uncoupling: The link between the benzodiazepine binding site and the chloride channel becomes less efficient
- GABA subsensitivity: The amount of Cl- that flows in per channel opening decreases
- Excitatory upregulation: To compensate, glutamate (NMDA receptor) systems upregulate
Net result: The patient needs higher doses to achieve the same sleep effect, and eventually the drug barely works at all for sleep (though some tolerance develops faster for hypnotic effects than for anxiolytic effects - the "dissociation of tolerance").
Management approach:
- Explain that this is expected pharmacology, not a personal failure
- Advocate CBT-I as the most effective long-term strategy for insomnia
- Do NOT simply increase the benzodiazepine dose - this perpetuates the cycle and increases dependence
- Begin a gradual tapering program
- Consider substituting with a non-GABA hypnotic (ramelteon or low-dose doxepin) for sleep
- Address underlying causes of insomnia (mood disorder, sleep apnea, pain, etc.)
This complete learning note was compiled from Katzung's Basic & Clinical Pharmacology (16th Ed.), Goodman & Gilman's The Pharmacological Basis of Therapeutics (13th Ed.), Kaplan & Sadock's Comprehensive Textbook of Psychiatry (10th Ed.), Kaplan & Sadock's Synopsis of Psychiatry (12th Ed.), and Stahl's Essential Psychopharmacology (5th Ed.).