now explain me the presentation that have been taught by you as excellent precise pdf.
Reading File
Reading File
Running Command
Running Command
Running Command
analyse_media
Running Command
Running Command
Running Command
Running Command
Running Command
I now have everything I need. Let me now compose a thorough explanation of the entire ARMD presentation, incorporating the feedback from the PDF.
ARMD Presentation — Full Explanation with Feedback Notes
This is a 76-slide presentation on Age-Related Macular Degeneration (ARMD/AMD) by Dr. Anisha Thapa, 3rd Year Resident, BEH/NAMS, dated 26th June 2026 (tomorrow's presentation). Below is a section-by-section explanation of everything covered, with the feedback from the "Excellent Precise" PDF woven in.
Your Feedback Score: 4/5 — SOLID. 1 Gap Filled (Tachyphylaxis)
The feedback states: "You are ready for tomorrow. Present confidently — you understand this topic deeply now, not just the slides."
Section 1 — Definition & Overview (Slides 1-3)
AMD is a degenerative disease of the central retina (macula) in patients aged 50 and above. Key facts you covered:
- Leading cause of irreversible legal blindness in developed countries (age ≥65)
- Affects ~3.5 million in the USA (2020); projected 5-9 million by 2050
- Two late forms: Geographic Atrophy (GA) = dry; Neovascular AMD (nAMD) = wet
- nAMD causes ~90% of severe vision loss despite being less common than GA
- WHO ranks AMD as the 3rd most common cause of global blindness after cataract and glaucoma
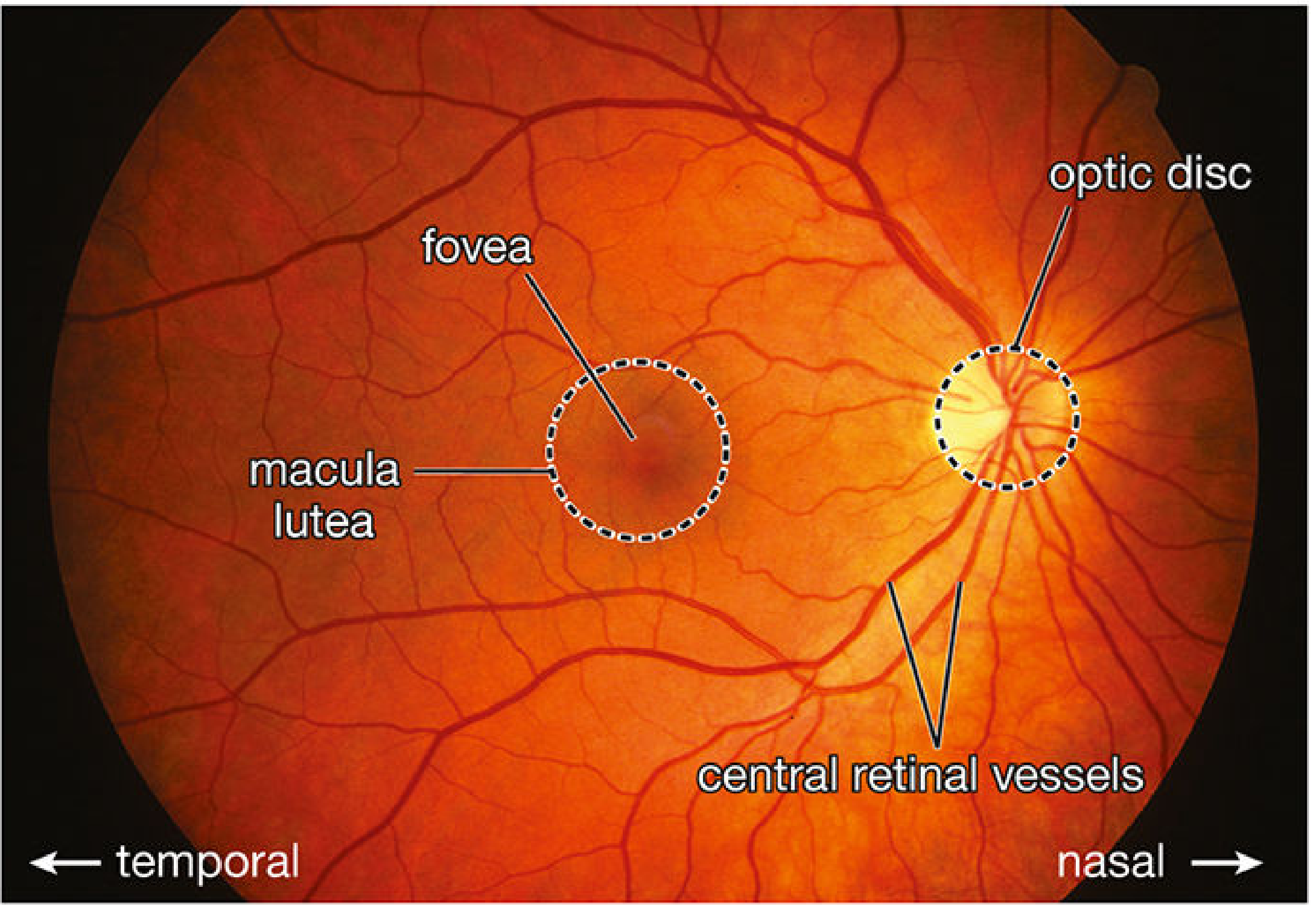
Section 2 — Anatomy of the Macula (Slide 4)
The macula is the central 5.5 mm of the retina responsible for all detailed central vision.
| Structure | Detail |
|---|---|
| Fovea centralis | 1.5 mm; contains only cones |
| Foveola | 0.35 mm - the densest cone zone |
| RPE | Single pigmented cell layer; phagocytoses 11-15% of outer segments daily |
| Bruch's membrane | 5-layered: collagen + elastin + two basement membranes |
| Choriocapillaris | Fenestrated capillary bed - primary nutrient source for RPE |
Section 3 — Epidemiology (Slides 5-7)
- Prevalence doubles each decade after age 50; >15% in Whites aged ≥80
- USA: Early AMD ~15.4 million; Late AMD ~2.1 million (NEI 2020)
- Nepal-specific data (a highlight of this presentation):
- AMD causes 8.7% of total blindness in Nepal
- 1 in 3 Nepalis aged ≥60 has some form of AMD (Thapa R et al., Clin Ophthalmol 2017; Bhaktapur district, n=1,860)
- BEH hospital data included with sex distribution
- 52.5% of AMD patients at KMCTH had VA 6/24-6/60; 15% had VA <3/60
Section 4 — Risk Factors (Slides 9-10)
Non-modifiable:
- Advanced age (strongest overall), family history (3-4× risk), White race, female sex, hyperopia (+1D = 13% increased odds), light iris colour
Modifiable:
- Cigarette smoking (2-4× risk - strongest modifiable factor; ~20% of cases in women)
- Systemic hypertension, high dietary fat/low omega-3, obesity/high BMI, low lutein/zeaxanthin, sedentary lifestyle
Section 5 — Genetics (Slide 11)
AMD is polygenic - GWAS has identified >40 susceptibility loci:
| Gene | Location | Effect |
|---|---|---|
| CFH (Y402H) | 1q32 | 2-4× risk; present in 35% of AMD cases; regulates alternative complement |
| ARMS2/HTRA1 | 10q26 | Major risk allele for both dry AND wet AMD |
| C3 | 19p13 | R102G variant increases risk |
| CFI | 4q25 | Loss-of-function increases risk |
| CFB/C2 | 6p21 | Protective haplotype |
Section 6 — Pathogenesis (Slides 12-15)
The pathogenesis flowchart (must-know):
Genetic susceptibility (CFH, ARMS2) + Environmental triggers → RPE dysfunction (↑lipofuscin/A2E, ↓phagocytosis) → Extracellular deposits in Bruch's (Basal Laminar Deposits → Drusen) → Complement activation + Oxidative stress + Inflammation → either GA (dry, late) or nAMD (wet, late)
Complement cascade:
- CFH normally inhibits the alternative pathway by cleaving C3b
- C3 convertase → C3a + C3b → C5 convertase → C5a + MAC (C5b-9)
- MAC deposition on RPE → cell lysis and photoreceptor death
- Drusen contain: vitronectin, complement C5b-9, C3d, CFH, immunoglobulins
Lipofuscin / A2E:
- A2E (N-retinylidene-N-retinylethanolamine) is the principal toxic fluorophore in RPE lysosomes
- Inhibits lysosomal enzymes, activates complement, induces RPE apoptosis
- Detectable on FAF as hyper-autofluorescence
- Therapeutic target: ALK-001 (deuterated Vitamin A) in Phase 2/3 GO-STAR trial
VEGF pathway:
- RPE hypoxia → HIF-1α → ↑VEGF-A mRNA (VEGF-A165 dominant isoform)
- VEGFR-2 (KDR/Flk-1) = main signalling receptor → endothelial proliferation + permeability
- Drug targets by receptor coverage: Pegaptanib (only VEGF-A165) → Ranibizumab/Bevacizumab (all VEGF-A) → Aflibercept (VEGF-A, VEGF-B, PlGF) → Faricimab (VEGF-A + Ang-2)
Section 7 — Drusen (Slides 16-17)
Drusen are the hallmark of AMD - multiple small yellow-white extracellular deposits at the RPE-Bruch's interface. The word comes from German ("geode" - a stone with crystal-lined cavity).
Types covered in the slide (with table on Slide 17):
- Hard drusen (small, sharp edges - low risk)
- Soft drusen (large, indistinct - higher risk)
- Cuticular/basal laminar drusen
- Reticular pseudodrusen / SDD (above RPE - very high risk)
Section 8 — Types of MNV & Special Subtypes (Slides 18-23)
Macular Neovascularisation (MNV) classification:
- Type 1 MNV - sub-RPE (occult CNV); often quiescent; associated with PCV
- Type 2 MNV - sub-retinal (classic CNV); leaks early on FFA
- Type 3 MNV (RAP) - intraretinal origin (deep capillary plexus); three stages
Subretinal Drusenoid Deposits (SDD):
- Located ABOVE the RPE (unlike drusen which are sub-RPE)
- Appear yellow-white ~250 µm; best seen on NIR reflectance
- High-risk: linked to Type 3 MNV, GA progression
- Complement D localises here (unlike soft drusen) - distinct pathogenesis
PCV (Polypoidal Choroidal Vasculopathy):
- Branching inner-choroidal network + terminal aneurysmal polyps
- Now classified as pachychoroid aneurysmal Type 1 MNV
- More common in Asians (22-54% of nAMD) and Africans; female > male (5:1)
- Presents with serosanguineous PED + massive subretinal haemorrhage
- Up to 50% may resolve spontaneously
RAP (Type 3 MNV):
- Stage I = intraretinal neovascularisation (IRN); Stage II = subretinal (SRN); Stage III = retinal-choroidal anastomosis (RCA)
- 10-20% of nAMD in White patients; often bilateral and underdiagnosed
Section 9 — Classification (Slides 24-25)
AREDS/Beckman Classification:
- Normal (no features)
- Early AMD (small/medium drusen only)
- Intermediate AMD (at least 1 large druse ≥125 µm OR multiple medium drusen)
- Late AMD (GA or nAMD)
AMD Staging Systems Comparison (Slide 25 - detailed table comparing AREDS, Beckman, Rotterdam scales)
Section 10 — Clinical Features (Slides 26-32)
Dry AMD:
- Symptoms: Gradual central vision loss, Amsler grid changes, poor dark adaptation (earliest functional sign)
- Signs: Drusen, RPE pigmentary changes
- GA: Well-demarcated RPE loss; pericentral "horseshoe" pattern → concentric foveal sparing → eventual foveal involvement
- Rod dysfunction precedes visible photoreceptor loss by years
Wet AMD:
- Symptoms: Sudden central visual loss, metamorphopsia, central scotoma
- Signs: SRF, IRF, PED, subretinal haemorrhage, exudate, disciform scar
- Fellow eye risk: 10-12% per year develop CNV
Massive Subretinal Haemorrhage:
- ≥4 disc diameters; haemoglobin → iron → free radical toxicity within 24-72 hours
- Urgent treatment needed within 7-14 days
- Management algorithm: small/extrafoveal → anti-VEGF alone; large/subfoveal → intravitreal tPA (100 µg) + C3F8 gas + anti-VEGF OR vitrectomy + subretinal tPA
PED Types:
- Serous PED - dome-shaped, optically empty on OCT; treat if MNV notch present
- Fibrovascular PED - irregular, heterogeneous OCT; anti-VEGF
- Drusenoid PED - soft drusen confluence; AREDS2 + monitor
- Haemorrhagic PED - urgent anti-VEGF ± subretinal tPA
RPE Tear:
- Mechanism: Large fibrovascular PED under tension → RPE splits and scrolls
- Risk factors: PED height >500 µm, PED width >1500 µm; commonly after anti-VEGF
- OCT: Sharp RPE discontinuity + hyperreflective scroll; FAF: hyper-AF at tear edge
- Management: Continue anti-VEGF - do NOT stop
Disciform Scar (end-stage):
- Fibrocellular replacement of regressed CNV; VA typically ≤6/60
- OCT: Hyperreflective dome-shaped mass; absent EZ; retinal atrophy
- Two phenotypes: fibrovascular (active - continue anti-VEGF) vs fibrocellular (quiescent)
Section 11 — Investigations & Imaging (Slides 33-37)
Multimodal Imaging Algorithm (must-know flowchart):
- SD-OCT: Mandatory for ALL AMD patients - assess fluid compartments, drusen, EZ integrity
- Dry AMD: add FAF (GA boundaries, junctional zones) + NIR (SDD)
- Wet AMD: add FFA (CNV type, trial eligibility) + ICGA (if PCV suspected) + OCTA
FAF patterns in GA (Slide 34):
- GA = well-demarcated hypo-AF (no lipofuscin = no signal)
- Junctional zone patterns predict progression rate
Dark Adaptation - Earliest Functional Biomarker:
- Rod Intercept (RI) measured by AdaptDx (MacuLogix)
- Normal RI: <6.5 min; Abnormal AMD: >6.5 min
- Delay precedes visible drusen by months to years (Owsley et al.)
- FARM study: Eyes with delayed RI at baseline were 2× more likely to develop AMD at 2 years
Section 12 — Differential Diagnosis (Slide 38)
Central macular conditions mimicking AMD: Central Serous Chorioretinopathy, Vitelliform dystrophy (Best disease), Stargardt disease, myopic maculopathy, drusen from other causes (optic nerve head drusen), pattern dystrophies.
Section 13 — Management of Dry AMD (Slides 39-40)
AREDS (2001): High-dose antioxidants + zinc reduced progression to advanced AMD by 25%
| Formula | Components |
|---|---|
| AREDS | Vit C 500mg + Vit E 400IU + Beta-carotene 15mg + Zinc 80mg + Copper 2mg |
| AREDS2 (2013) | Replace beta-carotene with Lutein 10mg + Zeaxanthin 2mg (safe in smokers) |
- Indicated for: Intermediate AMD (both eyes) OR advanced AMD/vision loss in one eye
- NOT indicated for early AMD or no drusen - no proven benefit
AREDS Simplified Severity Scale:
- 1 point per eye for large drusen (≥125 µm) OR any advanced AMD (max 4 points)
- Score ≥3 in at least one eye → start AREDS2 supplements
Section 14 — Management of Wet AMD (Slides 41-49)
Anti-VEGF = Gold Standard for nAMD
⚠ Q2 Feedback Correction:
The feedback flagged an error in your AFL loading description. Here is the precise table to memorise:
| Agent | Loading | Maintenance |
|---|---|---|
| Ranibizumab | 3 × monthly | PRN or T&E up to q12w |
| Bevacizumab | 3 × monthly | PRN or T&E |
| Aflibercept | 3 × monthly | q8w fixed or T&E |
| Faricimab | 4 × monthly | T&E up to q16w |
| Brolucizumab | 3 × monthly | q12w or q8w |
Key point: Faricimab has 4 loading doses, all others have 3. This is the distinction to not mix up.
Dosing strategies:
- Monthly (fixed): Best outcomes (CATT, ANCHOR, MARINA); high injection burden
- PRN (as needed): Less injections; risk of undertreatment
- T&E (Treat & Extend): Most widely used; extend by 2-week increments when dry; reduce when fluid recurs
Complications of intravitreal anti-VEGF (Slide 47): Endophthalmitis, traumatic cataract, RD, vitreous haemorrhage, IOP spike, RPE tear, retinal vasculitis (brolucizumab-specific concern)
Section 15 — Tachyphylaxis (Slide 49)
⚠ Q3 Feedback - Gap Filled:
This was the only topic you said you were unsure about. The feedback explains it fully:
Tachyphylaxis = reduced response to the same anti-VEGF drug after an initially good response, without disease progression.
- Incidence: ~10-14% of patients on ranibizumab or bevacizumab
- Mechanism: The eye upregulates alternative angiogenic pathways (PDGF, Ang-2, HIF-1α) not blocked by the current drug - the CNV "finds a way around the blockade"
- Switch criteria: Persistent/recurrent fluid despite ≥3 consecutive injections of current agent
- Evidence: GEFAL, BRAMD, Lucas trials - switching improves anatomical outcomes in 50-60% of refractory cases
- Switch sequence: Bevacizumab → Ranibizumab → Aflibercept → Brolucizumab → Faricimab
Why faricimab is attractive in tachyphylaxis: It blocks Ang-2, which is one of the very alternative pathways that gets upregulated when VEGF-A blockade alone stops working.
Section 16 — Faricimab (Slides 56, 63)
⚠ Q4 Feedback - "Correct, needs more depth"
You named both targets correctly. The mechanism to complete the answer:
- Ang-2 is elevated in wet AMD; it antagonises the Tie2 receptor on endothelial cells, destabilising vessels and increasing leakage/inflammation
- When you block VEGF-A alone, Ang-2 still destabilises vessels
- Faricimab blocks BOTH: VEGF-A blockade stops new vessel growth + Ang-2 blockade stabilises existing vessels via Tie2 activation
- This dual mechanism achieves more complete suppression → longer injection intervals (up to q16w)
- YOSEMITE (n=972) + LUCERNE (n=919): Non-inferior to aflibercept at 1 year (+5.5-6.7 letters); 45% of patients maintained q16w dosing at 2 years
- FDA approved January 2022 - ophthalmology's first dual-mechanism biologic
Section 17 — GA Treatments (Slide 58)
⚠ Q5 Feedback - "Correct and Honest"
Your GA treatment answer was marked perfect, and the patient communication script was praised:
GA grows at ~1.78 mm²/year. Two approved treatments:
| Agent | Mechanism | FDA Approval | Trial Result |
|---|---|---|---|
| Pegcetacoplan (Syfovre) | C3 inhibitor | Feb 2023 (1st GA treatment) | 20% reduction in GA growth at 12 months (FILLY) |
| Avacincaptad Pegol (Izervay) | C5 inhibitor | Aug 2023 (2nd GA treatment) | 35% reduction in GA growth (GATHER1, p=0.001) |
Both are monthly intravitreal injections. Main concern: risk of conversion to nAMD.
Patient communication script (feedback-praised):
"These injections cannot bring back the vision you have already lost, and they cannot cure the disease. What they can do is slow down the rate at which the bare patch grows - so you keep your useful central vision for longer. Without treatment, the patch grows about 1.78 mm² every year. With treatment, we can reduce that by about 22-35%. It is not a cure, but it is meaningful - every month of useful central vision matters."
Section 18 — Extended-Duration Agents & New Approvals (Slides 55-67)
- Brolucizumab (Beovu): Approved 2020; q12w dosing; superior fluid control (HAWK/HARRIER). Concern: rare retinal vasculitis/occlusion
- Eylea HD (Aflibercept 8 mg): FDA approved Aug 2023; 4× molar dose; PULSAR trial showed non-inferiority with q12w/q16w intervals; 78% maintained q12w
- Port Delivery System (PDS/Susvimo): Implantable reservoir; ~88% refill-free at 6 months (ARCHWAY trial); FDA approved Oct 2021
Section 19 — Emerging Therapies (Slides 60-61, 68-69)
- Gene therapy: RGX-314 (subretinal AAV8), ADVM-022 (intravitreal), 4D-150 (dual VEGF-A+C blockade) - all in Phase II/III
- Photobiomodulation (PBM): LumiThera Valeda system; LIGHTSITE III - +4.1 letters vs +1.0 sham at 13 months
- Stem cell/RPE transplantation: hESC-RPE and iPSC-RPE patches; Phase 1/2 showing safety; Phase 3 not yet started
- Biosimilars: Aflibercept biosimilars (Opuviz, Pavblu, Ahzantive) FDA approved 2025; 40-60% cost reduction
- AI: Google DeepMind/Moorfields - AI matches retinal specialists in AMD referral; Home OCT (Notal Orbis) for remote monitoring
Section 20 — Prognosis & Natural History (Slide 70)
- Dry AMD: Slow; most maintain reading vision for years while fovea is spared
- GA growth rate: 1.78 mm²/year (range 0.53-5.6)
- Wet AMD untreated: 50% lose ≥3 lines at 2 years; 90% by 5 years
- Wet AMD treated: 30-40% gain ≥3 lines at 1 year; 40% maintain at 5 years
- Fellow eye: 10% annual risk; cumulative 30% at 5 years in high-risk eyes
- AMD rarely causes total blindness - peripheral vision is always preserved
Section 21 — Patient Education & Low Vision (Slides 71-73)
- Amsler grid: Test each eye separately at 30 cm; report new changes within 24 hours; limitation = up to 50% false-negatives
- ForeseeHome (PHP): Sensitivity 83%, Specificity 82%; FDA-cleared; 3×/week use
- Low vision aids: Magnifiers, CCTV, IMT (2.2-2.7× magnification for end-stage bilateral disease), eccentric viewing training
- Psychosocial: Depression in 40% of AMD patients - refer for counselling
Three Things to Review Tonight (from feedback):
- The drug loading table - Faricimab has 4 loading doses, all others have 3
- Tachyphylaxis - the word, 10-14% incidence, switch sequence (Bevacizumab → Ranibizumab → Aflibercept → Brolucizumab → Faricimab)
- PCV vs RAP on ICGA - Branching network + polyps = PCV; hot spot near retinal vessel = RAP
AREDS2 Q1 - Perfect Answer Confirmed:
Your AREDS2 formula answer was rated perfect ("word for word correct"). The formula: Lutein 10 mg + Zeaxanthin 2 mg + Vitamin C 500 mg + Vitamin E 400 IU + Zinc 80 mg + Copper 2 mg.
The feedback confirms you have covered the entire AMD curriculum across all sections: anatomy, RPE functions, Bruch's, visual cycle/A2E, pathogenesis, genetics, clinical features, all imaging modalities, AREDS2, all anti-VEGF agents, dosing strategies, tachyphylaxis (now filled), GA treatments, Nepal epidemiology. You are well-prepared for tomorrow's presentation.
what layers of retina is absent in macula?
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
I have everything from the textbooks. Here is the complete, precise answer:
Retinal Layers Absent in the Macula (Fovea/Foveola)
The answer depends on exactly which part of the macula you are referring to, because the macula has concentric zones with progressively fewer layers as you move toward the centre.
At the Foveola (centre of the fovea, ~0.35 mm) — Most Layers Absent
This is the clinically important answer. The following layers are absent or markedly reduced:
| Layer | Status at Foveola |
|---|---|
| Nerve Fibre Layer (NFL) | Absent |
| Ganglion Cell Layer (GCL) | Absent (displaced laterally) |
| Inner Plexiform Layer (IPL) | Absent |
| Inner Nuclear Layer (INL) | Absent (displaced laterally) |
| Outer Plexiform Layer (OPL) | Absent / markedly reduced |
| Rods | Absent - only cones present |
| Retinal blood vessels | Absent - avascular zone |
What remains: Only the cone photoreceptors (outer and inner segments), the outer nuclear layer (ONL), external limiting membrane, RPE, and Bruch's membrane. The cones here are uniquely elongated, narrow, and densely packed (~4,000 cones in the foveola).
Why Are These Layers Displaced?
During foveal development and in the mature retina, the cell bodies of the ganglion cell layer and inner nuclear layer are physically pushed (displaced) centrifugally outward - away from the foveal pit. This lateral displacement creates the foveal depression (pit). The result is that incoming light travels in a straight line with no obstruction directly to the cone outer segments, maximising visual acuity.
"The fovea is a shallow depression within the retina where cells bodies of the ganglionic and INLs become dispersed peripherally, leaving primarily cone cells. Devoid of most conducting neurons as well as capillaries, the fovea allows light to fall directly on its cones with very little scatter." - Junqueira's Basic Histology, 17th ed.
"Except for the photoreceptor layer, most of the layers of the retina are markedly reduced or absent in this region." - Histology: A Text and Atlas (Ross), 9th ed.
Summary by Zone
| Zone | Diameter | Key Feature |
|---|---|---|
| Foveola | 0.35 mm | Only cones; all inner layers absent; avascular |
| Fovea centralis | 1.5 mm | Inner layers progressively thinned/absent centrally |
| Parafovea | ~2.5 mm | All 10 layers present; highest GCL density (up to 8 cell layers) |
| Macula lutea | ~5.5 mm | Contains both rods and cones; avascular but all layers present |
Quick Exam Memory Aid
At the foveola, the absent layers spell out the inner retina - everything from the GCL inward to the OPL is gone. Only the outer retina (photoreceptors = cones only + ONL) remains. No rods, no vessels, no inner layers = maximum acuity, minimum scatter.
What is the foveal avascular zone and its clinical significance?
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have the core textbook content from Kanski's. Now I'll compile a thorough answer combining that with my knowledge.
Foveal Avascular Zone (FAZ)
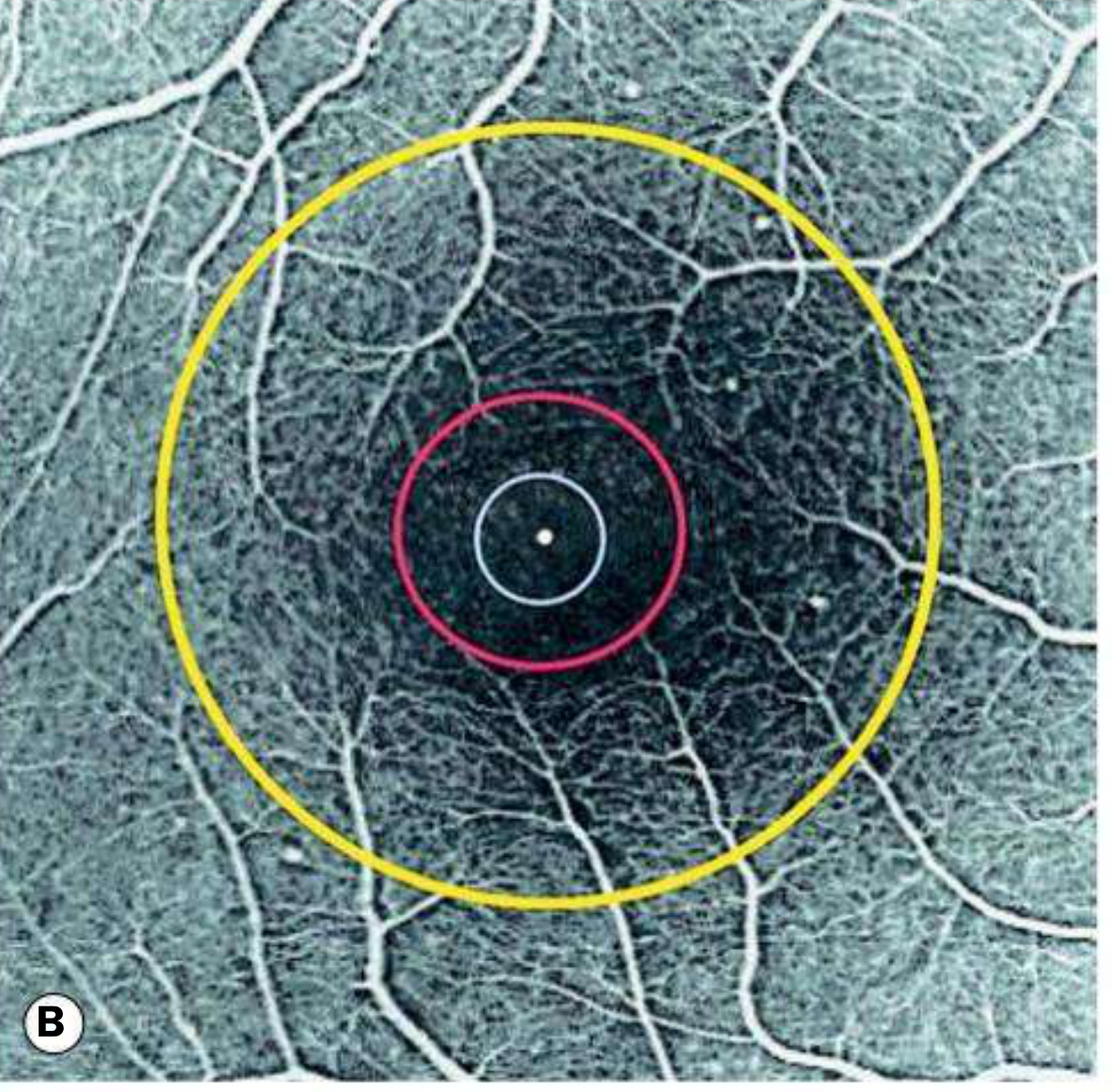
Fig. 14.1B from Kanski's Clinical Ophthalmology (10th ed): Fluorescein angiogram of the normal macula. Yellow circle = fovea (1.5 mm), red circle = FAZ boundary (~0.6 mm), white circle = foveola (0.35 mm), central white dot = umbo.
Definition
The FAZ is the central capillary-free region of the retina, located within the fovea but extending slightly beyond the foveola. It is surrounded by a continuous arcade of capillaries from the superficial and deep capillary plexuses.
"A central area containing no blood vessels but surrounded by a continuous network of capillaries, located within the fovea but extends beyond the foveola. The exact diameter varies with age and in disease and its limits can be determined with accuracy only by fluorescein angiography (average 0.6 mm)." - Kanski's Clinical Ophthalmology, 10th ed.
Normal Dimensions
| Parameter | Normal Value |
|---|---|
| Average diameter | ~0.6 mm (range 0.3 - 1.0 mm) |
| Area | ~0.1 - 0.5 mm² |
| Shape | Roughly circular/elliptical |
| Best measured by | Fluorescein Angiography (FFA) or OCTA |
Normal size varies considerably between individuals, and the FAZ is larger in older people even without disease.
Why Does the FAZ Exist? (Anatomy)
The foveal cones are not supplied by retinal vessels. They rely entirely on:
- Choriocapillaris - the fenestrated capillary layer of the choroid, which delivers oxygen and nutrients by diffusion through Bruch's membrane and the RPE
- The avascular design is not a deficiency - it is purposeful. Retinal vessels would:
- Cast shadows on the photoreceptors
- Scatter and refract incoming light
- Reduce the cone packing density possible at the fovea
The FAZ is therefore a structural prerequisite for maximum visual acuity.
Clinical Significance
The FAZ is important in several clinical contexts:
1. Landmark for Laser Treatment
The FAZ defines the absolute exclusion zone for macular laser photocoagulation. Any thermal laser applied within the FAZ destroys the underlying cone photoreceptors permanently, causing a central scotoma. Clinicians must confirm the FAZ boundary on FFA before treating conditions like:
- Diabetic macular oedema (focal/grid laser)
- Extrafoveal CNV in AMD
- Central serous chorioretinopathy
2. Macular Ischaemia - FAZ Enlargement
Any condition causing capillary occlusion/dropout around the FAZ leads to FAZ enlargement - a marker of macular ischaemia. This directly correlates with visual acuity loss.
| Disease | FAZ Change | Clinical Effect |
|---|---|---|
| Diabetic retinopathy | Enlargement + irregular margins | Reduced VA; predicts poor anti-VEGF response |
| Retinal vein occlusion (BRVO/CRVO) | Focal or global FAZ enlargement | Vision loss proportional to FAZ area |
| Sickle cell retinopathy | Characteristic "sea-fan" neovascularisation adjacent to FAZ; FAZ enlargement | Macular ischaemia common even without proliferative disease |
| Radiation retinopathy | Progressive capillary closure; FAZ enlargement | Chronic vision loss post-radiotherapy |
| Purtscher's retinopathy | Capillary occlusion around FAZ | Acute vision loss after trauma/systemic disease |
3. OCTA - Non-Invasive FAZ Measurement
Optical Coherence Tomography Angiography (OCTA) has replaced FFA for FAZ assessment in many clinical scenarios. It allows:
- Precise measurement of FAZ area, perimeter, and circularity index
- Separate visualisation of the superficial vs deep capillary plexus FAZ
- Monitoring FAZ enlargement over time in diabetic retinopathy grading
- The deep capillary plexus FAZ is often enlarged earlier than the superficial one in diabetic macular ischaemia
4. Surgical Safety Margin
In macular surgery (epiretinal membrane peeling, ILM peeling for macular hole), the FAZ marks the central danger zone. Iatrogenic trauma within this zone causes permanent cone loss.
5. Parafoveal Telangiectasia (MacTel Type 2)
In Macular Telangiectasia Type 2, the temporal perifoveal capillaries are specifically abnormal, causing characteristic leakage and right-angle venules adjacent to the FAZ - a disease defined by its relationship to the FAZ perimeter.
6. Prognostic Marker
- FAZ area on OCTA is now used as a biomarker in diabetic retinopathy clinical trials
- A larger baseline FAZ predicts worse visual prognosis and poorer response to anti-VEGF in diabetic macular oedema
- FAZ irregularity index (how non-circular the FAZ is) correlates with severity of macular ischaemia
How the FAZ is Assessed
| Method | Details |
|---|---|
| FFA (Gold standard historically) | Dynamic leakage visible; FAZ boundary defined by capillary arcade; requires dye injection |
| OCTA (Current preferred method) | No dye; quantitative; separate superficial/deep plexus; reproducible measurements |
| Normal FFA appearance | Dark hypofluorescent central zone surrounded by continuous bright capillary arcade |
Quick Summary
The FAZ is a ~0.6 mm capillary-free zone at the foveal centre that exists to preserve maximum optical clarity for the foveal cones, which are instead nourished by the choriocapillaris. Its clinical importance comes from two directions: it is a no-go zone for laser treatment, and its enlargement = macular ischaemia in diseases like diabetic retinopathy, retinal vein occlusion, and sickle cell retinopathy, directly predicting visual outcome.
what is this in relation to ARMD?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
The library FTS isn't returning results for these combined terms. I have strong foundational content from Kanski's already retrieved, plus the full ARMD presentation content from earlier. I'll synthesise a thorough answer from both.
The FAZ in Relation to AMD
The FAZ is deeply relevant to AMD across both dry and wet forms, affecting classification, treatment decisions, prognosis, and the explanation of visual symptoms. Here is how they connect:
1. In Dry AMD / Geographic Atrophy (GA)
The FAZ is the Last Thing GA Spares - Until It Doesn't
GA spreads in a characteristic pericentral "horseshoe" pattern, expanding concentrically while the fovea and its avascular zone are paradoxically spared until late. This is why dry AMD patients often say "I can still read, but I have a dark ring around my central vision."
Why foveal sparing occurs:
The foveal cones are nourished exclusively by the choriocapillaris, not retinal vessels. As GA destroys the RPE and choriocapillaris in the perifoveal area, the foveola - being the most metabolically adapted zone - resists atrophy the longest. There is also evidence that the higher density of lutein and zeaxanthin at the fovea provides some antioxidant protection.
Clinical stages:
| Stage | FAZ relationship | Vision |
|---|---|---|
| Early/intermediate GA | Pericentral atrophy; FAZ intact | Reading vision preserved |
| Advanced GA (foveal sparing) | GA surrounds fovea - "horseshoe" | Patient still reads but has ring scotoma |
| End-stage GA (foveal involvement) | GA crosses into FAZ, destroys foveal cones | Severe central vision loss, <6/60 |
This is the rationale behind GA treatments (pegcetacoplan/avacincaptad pegol): the goal is to slow GA growth rate specifically to delay foveal involvement. Every month the FAZ is preserved = every month of useful central vision retained. This is exactly the patient communication script praised in your feedback PDF: "the bare patch grows 1.78 mm²/year...we can reduce that by 22-35%...every month of useful central vision matters."
2. In Wet AMD / Neovascular AMD (nAMD)
CNV Location Relative to the FAZ is the Most Important Prognostic Factor
The entire historical classification of CNV in AMD was built around its relationship to the FAZ. This came from the Macular Photocoagulation Study (MPS) group, which defined three positions:
| CNV Position | Definition | Treatment implication |
|---|---|---|
| Extrafoveal | CNV edge >200 µm from FAZ centre | Laser photocoagulation possible (pre-anti-VEGF era) |
| Juxtafoveal | CNV edge 1-199 µm from FAZ centre | Laser risky - high recurrence under FAZ |
| Subfoveal | CNV edge directly under FAZ / overlapping it | Laser absolutely contraindicated - destroys fovea; anti-VEGF only |
In the pre-anti-VEGF era, this classification completely determined treatment. Extrafoveal CNV could be lasered; subfoveal CNV had no good treatment, and patients were essentially told to expect severe central vision loss.
Anti-VEGF changed everything: Because anti-VEGF is injected intravitreally and acts systemically on the vitreous cavity, subfoveal CNV can now be treated regardless of its FAZ relationship. This is what made anti-VEGF revolutionary - for the first time, patients with CNV directly under the FAZ had a realistic chance of visual gain.
3. Why Subfoveal CNV Causes Acute Severe Vision Loss
When CNV grows under or through the FAZ:
- The neovascular membrane lifts the RPE and neurosensory retina off Bruch's membrane directly beneath the foveal cones
- Subretinal fluid (SRF) accumulates under the foveola - even 50-100 µm of fluid separating cones from the RPE causes immediate vision distortion (metamorphopsia) and blur
- Intraretinal fluid (IRF) within the foveal layers causes cystic changes that disrupt cone packing
- Subretinal haemorrhage into the FAZ zone is directly toxic to cones within 24-72 hours (haemoglobin → iron → free radical damage)
- Fibrovascular PED directly under the FAZ pushes the foveal cones upward, creating a PED detachment that distorts the visual image
This is why wet AMD classically presents with sudden metamorphopsia and central vision loss - the FAZ is being disrupted from below.
4. Treatment Endpoint and the FAZ - "Fluid Under the Fovea"
In anti-VEGF treatment monitoring, whether fluid is within or immediately adjacent to the FAZ determines the urgency and aggressiveness of retreatment:
- IRF touching the foveal centre = treat immediately; even small amounts cause vision loss
- SRF under the foveola = treat; though some studies (FLUID trial) suggest small amounts of SRF may be tolerable in T&E protocols
- Dry fovea (no fluid in FAZ zone) = extend interval (T&E protocol)
The OCT measurement of central subfield thickness (CST) - the 1 mm central circle directly corresponding to the FAZ area - is the primary anatomical endpoint in all AMD anti-VEGF trials.
5. End-Stage nAMD - Disciform Scar Over the FAZ
When CNV is not treated (or fails treatment), the neovascular membrane undergoes fibrocellular replacement - the disciform scar. When this scar sits over the FAZ:
- Cone photoreceptors overlying the scar are permanently destroyed
- The ellipsoid zone (EZ line) on OCT is absent centrally
- VA is typically ≤6/60; a dense central scotoma replaces the FAZ
- The patient loses reading vision, face recognition, and driving ability permanently
- Peripheral vision is preserved (the rest of the retina outside the macula is unaffected) - this is why AMD rarely causes total blindness
6. OCTA and the FAZ in AMD Monitoring
OCTA can now image the FAZ in AMD without dye injection, and shows:
- Type 1 MNV (sub-RPE CNV): Abnormal flow signals beneath the RPE layer adjacent to the FAZ - often present for years before symptoms
- Type 2 MNV (subretinal CNV): Neovascular fronds visible above RPE, often extending into or through the FAZ
- Type 3 MNV / RAP: Intraretinal vessels originating from deep capillary plexus adjacent to the FAZ, with anastomosis eventually reaching the FAZ
- GA monitoring: OCTA shows choriocapillaris flow deficit at the FAZ margins, predicting where GA will spread next
Summary: The FAZ in AMD
| Aspect | Dry AMD (GA) | Wet AMD (nAMD) |
|---|---|---|
| FAZ involvement | Late; foveal sparing is protective | Early; subfoveal CNV = immediate threat |
| Visual significance | Foveal involvement = end of reading vision | Any fluid under FAZ = metamorphopsia + VA loss |
| Treatment relevance | Goal = delay GA reaching FAZ | FAZ location determines treatment urgency/type |
| Imaging | OCT - central EZ line integrity | OCT CST; OCTA for CNV under FAZ |
| Prognosis | Good if FAZ spared; poor once involved | Poor if subfoveal scar forms; good if treated early |
The bottom line: in AMD, preserving the FAZ = preserving central vision. Everything in AMD management - from AREDS2 supplements to anti-VEGF timing to GA treatment - is ultimately aimed at keeping the ~0.6 mm avascular zone and its underlying cone photoreceptors functioning for as long as possible.
does the macula consists of all the 10 layers? only fovea is devoid of inner layer?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
The textbooks confirm this precisely. Here is the clear answer:
Yes - Your Understanding is Correct
The macula does have all 10 retinal layers, and it is specifically only the fovea (and foveola at its centre) where the inner layers are absent/displaced. But the story is richer than a simple yes/no - the macula is actually thicker and more complex than the peripheral retina in most of its area.
Layer-by-Layer Breakdown Across Macular Zones
| Layer | Peripheral Retina | Macula (parafovea) | Fovea (slopes) | Foveola (centre) |
|---|---|---|---|---|
| 1. ILM (Inner Limiting Membrane) | ✓ | ✓ | ✓ | ✓ |
| 2. NFL (Nerve Fibre Layer) | ✓ | ✓ (thick) | Thinning | Absent |
| 3. GCL (Ganglion Cell Layer) | ✓ (1 cell layer) | ✓ (up to 8 layers deep) | Displaced laterally | Absent |
| 4. IPL (Inner Plexiform Layer) | ✓ | ✓ | Thinning | Absent |
| 5. INL (Inner Nuclear Layer) | ✓ | ✓ | Displaced laterally | Absent |
| 6. OPL (Outer Plexiform Layer) | ✓ | ✓ | Reduced | Absent |
| 7. ONL (Outer Nuclear Layer) | ✓ | ✓ | ✓ | ✓ (cone nuclei only) |
| 8. ELM (External Limiting Membrane) | ✓ | ✓ | ✓ | ✓ |
| 9. Photoreceptors (IS/OS) | Rods + Cones | Mostly cones | Cones only | Cones only (no rods) |
| 10. RPE | ✓ | ✓ (taller, thinner cells) | ✓ | ✓ |
The Key Histological Fact That Defines the Macula
"Histologically, it [the macula] shows more than one layer of ganglion cells, in contrast to the single ganglion cell layer of the peripheral retina." - Kanski's Clinical Ophthalmology, 10th ed.
"Over most of the retina, the ganglion cells are only a single layer of cells. At the macula, however, they are piled as many as eight deep, although they are absent over the fovea itself." - Histology: A Text and Atlas (Ross), 9th ed.
This is actually the histological definition of the macula - the area where the GCL is more than one cell thick. It is not defined by the visible yellow colour or the 5.5 mm measurement alone - histologically, having multiple GCL layers IS what makes it the macula.
Visual Summary: Thickness Profile Across the Macula
Peripheral Parafovea Fovea rim Foveola
retina (macula) (slopes) (centre pit)
─────────────────────────────────────────────────────
10 thin → 10 layers, → Layers Only outer
layers THICKER, thinning, retina
GCL up to inner remains
8 layers displacing (cones + ONL
deep laterally + RPE)
On OCT, you can see this as:
- The macula is the thickest region of the retina outside the optic disc
- The fovea is a depression/pit (thinner than surrounding macula)
- The foveola at the bottom of the pit is the thinnest point of the entire retina
Why This Matters Clinically in AMD
- In AMD, when people say "macular degeneration affects the macula," they mean all of this thick, multi-layered, cone-rich region
- But the functional impact is most devastating when the disease reaches the foveola - the thinned, inner-layer-free cone-only zone at the centre
- That is why GA "spares the fovea" for so long - the pericentral macula (parafovea, with all its layers) degenerates first, while the structurally distinct foveola resists longest
In one sentence: The macula has all 10 layers and is actually thicker than peripheral retina (GCL up to 8 layers deep); it is only at the fovea/foveola that inner layers disappear as they are pushed sideways to allow direct light access to cone photoreceptors.
modest association with blue or grey iris in AMD. why?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
iris color melanin AMD macular degeneration risk
Finding Sources
The library FTS isn't matching these specific terms. I already retrieved the RPE functions from Kanski's earlier in this session (line 2436: "The dense RPE pigment serves to absorb stray light"). I'll now give a thorough explanation using that plus my knowledge of the mechanism.
Why Blue/Grey Iris = Modest Increased AMD Risk
This is all about melanin - its quantity, location, and protective roles in the eye.
The Core Principle: Iris Colour = Proxy for Ocular Melanin Content
Iris colour is determined by the amount of melanin in the iris stroma:
- Brown iris = high melanin content
- Blue/grey iris = low melanin content (the blue colour is actually a structural/Tyndall scattering effect from a melanin-poor stroma, not from blue pigment)
Critically, iris melanin content correlates with melanin content throughout the uveal tract - including the choroid and, to a degree, the RPE. People with blue eyes tend to have less total ocular melanin, including in the choroidal melanocytes.
Where Melanin Matters in the Eye (and Why)
There are two distinct melanin-containing compartments relevant to AMD:
1. RPE Melanosomes
The RPE cells contain abundant melanosomes in their apical pigmented section. Their functions directly relevant to AMD:
- Absorb stray and scattered light - prevents photons from bouncing back and damaging photoreceptors a second time
- Quench reactive oxygen species (ROS) - melanin acts as a free radical scavenger; without it, photo-oxidative damage accumulates in the RPE
- Protect against phototoxicity - especially short-wavelength (blue) light, which is the most energetic and damaging portion of the visible spectrum
"The dense RPE pigment serves to absorb stray light." - Kanski's Clinical Ophthalmology, 10th ed.
2. Choroidal Melanocytes
The choroidal stroma is rich in melanocytes. People with lightly pigmented eyes have fewer/less active choroidal melanocytes, resulting in a blonde/amelanotic choroid (visible on fundoscopy as the choroidal vessels show through clearly). This means:
- Less light absorption within the choroid
- More light back-scatter reaching the RPE from behind
- Greater cumulative phototoxic load on the RPE over a lifetime
The Mechanistic Chain Linking Blue Iris → AMD
Blue/grey iris
↓
Low melanin in iris stroma → Low melanin in uveal tract (choroid + RPE)
↓
Less light absorption in choroid → More back-scattered photons hitting RPE
Less RPE melanin → Less ROS quenching per photon absorbed
↓
Greater cumulative oxidative stress on RPE over decades
↓
↑ Lipofuscin (A2E) accumulation in RPE lysosomes
↑ Oxidative damage to Bruch's membrane
↑ Complement activation
↓
Accelerated drusen formation → Earlier/more severe AMD
Why Short-Wavelength (Blue) Light is the Key Culprit
Blue light (wavelength ~400-500 nm) is particularly relevant because:
- It carries the most energy of all visible wavelengths (E = hc/λ - shorter wavelength = higher energy)
- It is specifically absorbed by A2E (the toxic bis-retinoid in RPE lipofuscin), which then generates singlet oxygen and ROS
- The RPE of lightly pigmented eyes has less melanin to intercept and neutralise these photons before they reach A2E
This is also why lutein and zeaxanthin (the yellow macular pigments in AREDS2) are protective - they act as a short-wavelength filter in the inner retina, absorbing blue light before it reaches the RPE. People with blue irises and low choroidal melanin essentially have less of this natural UV/blue light defence throughout the eye.
Why the Association is Only "Modest"
This is an important nuance from your presentation slide. The association is real but not strong for several reasons:
-
Confounding with race: Blue eyes predominantly occur in White/European populations, who already have higher AMD risk from genetic factors (CFH Y402H, ARMS2 variants). It is difficult to separate the iris colour effect from the underlying genetic susceptibility of that population.
-
RPE melanin is not perfectly correlated with iris colour: RPE melanin content varies somewhat independently of iris colour, especially with age - RPE melanin decreases with ageing in everyone regardless of iris colour, which may dilute the difference.
-
Melanin is dual-natured: Young melanin is photoprotective. But aged/oxidised melanin (particularly in the RPE) can actually generate ROS rather than quench them - so the relationship is not simply "more melanin = always better." This complexity weakens the epidemiological signal.
-
Other risk factors dominate: Smoking (2-4× risk), CFH genetics, age, and diet have far larger effect sizes than iris colour. The iris colour effect gets diluted in multivariate models.
Clinical Relevance in AMD Context
- This is why UV-protective sunglasses are recommended in AMD prevention guidelines - even if the evidence is described as "uncertain" (from your presentation), the rationale is sound: reducing phototoxic load on the RPE, especially in lightly pigmented eyes
- It also explains part of the racial disparity in AMD prevalence: White populations (predominantly lighter irides, lower total ocular melanin) have higher AMD rates than African Americans (predominantly darker irides, higher melanin)
- It connects to the A2E/lipofuscin pathway in AMD pathogenesis: A2E accumulation is driven by photo-oxidative stress, and less melanin = more unchecked blue-light-driven A2E generation
In short: Blue/grey irises signal low total ocular melanin. Melanin in the RPE and choroid absorbs back-scattered light and quenches free radicals. Less melanin → more cumulative oxidative stress on the RPE over a lifetime → accelerated AMD pathogenesis. The association is modest because iris colour is only a proxy for ocular melanin, and other risk factors (genetics, smoking) have far larger effects.
basal laminar deposit inn AMd?
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
I have everything needed. Here is the full answer:
Basal Laminar Deposits (BLamD) in AMD
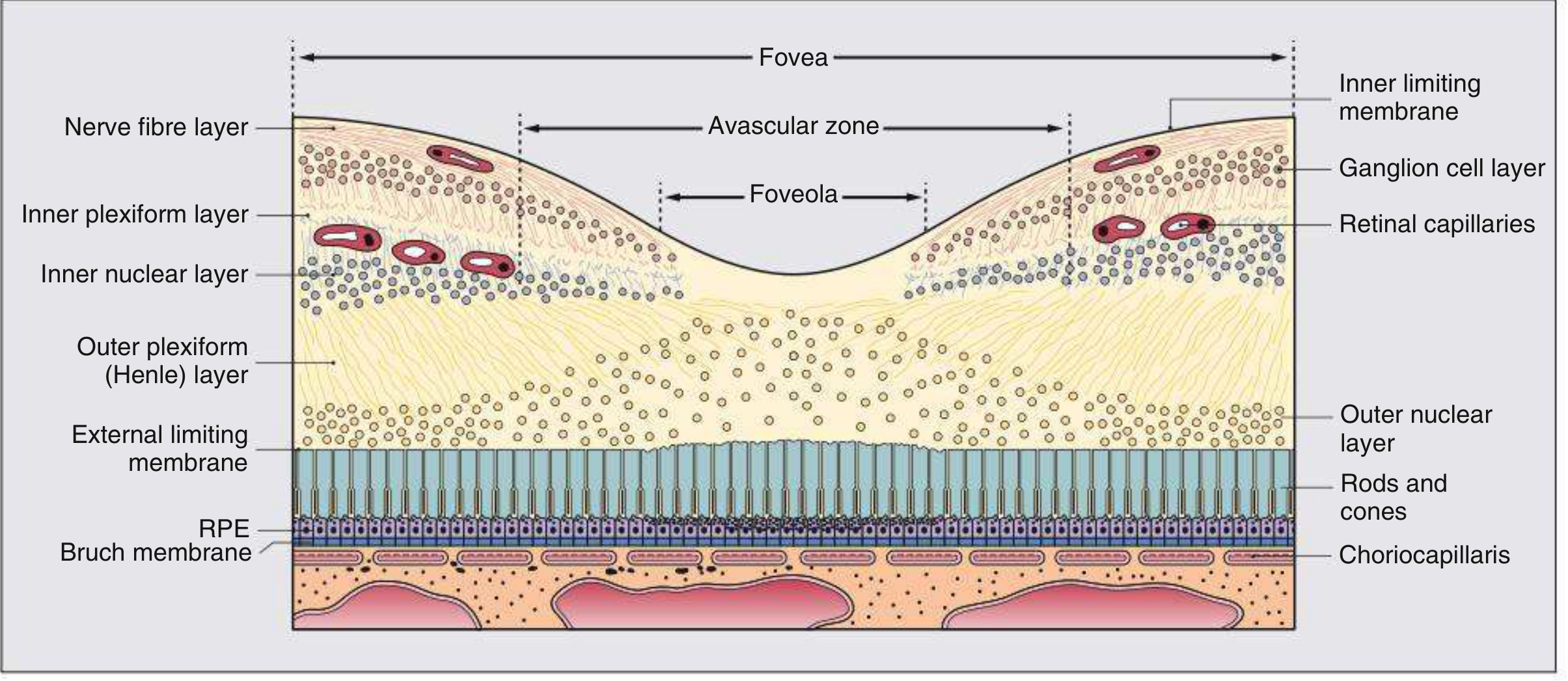
Fig. 14.2 from Kanski's Clinical Ophthalmology (10th ed): Cross-section of the fovea. Note the RPE layer sitting directly on Bruch's membrane, with the choriocapillaris below. Deposits accumulate within and below this RPE-Bruch's interface.
First - The Crucial Terminology Distinction
There are three distinct types of deposits in AMD, and confusion between them is very common in exams. They differ by their precise anatomical location within the Bruch's membrane complex:
Recall Bruch's membrane has 5 layers (inner to outer):
- Basement membrane of RPE ← innermost
- Inner collagenous layer
- Elastic fibre layer
- Outer collagenous layer
- Basement membrane of choriocapillaris ← outermost
The Three Types of Sub-RPE Deposits
| Deposit | Location | Material | Relationship to Drusen |
|---|---|---|---|
| Basal Laminar Deposit (BLamD) | Between RPE plasma membrane and RPE basement membrane (i.e., inside/beneath the RPE cell, above its own basement membrane) | Fibrous long-spacing collagen, fibronectin, wide-spaced collagen (electron microscopy) | Does NOT directly form drusen; diffuse; present in almost all eyes >50 yrs |
| Basal Linear Deposit (BLinD) | Between the RPE basement membrane and the inner collagenous layer of Bruch's | Membranous debris, vesicular/lamellar material, lipids | The direct precursor to soft drusen; focally thickens to form soft drusen |
| Drusen | Between the RPE basement membrane and inner collagenous layer of Bruch's (same plane as BLinD, but focally mounded) | Complement proteins (C3d, C5b-9, CFH), vitronectin, lipids, immunoglobulins | Drusen = focal mound of BLinD material |
"Basal laminar deposit [is] a layer that accumulates between the RPE and the RPE basement membrane (the inner layer of Bruch membrane) in AMD. Basal linear deposit is a distinct finding consisting of membranous debris laid down between the RPE basement membrane and the inner collagenous layer of Bruch membrane that may progress focally to form drusen." - Kanski's Clinical Ophthalmology, 10th ed.
Basal Laminar Deposit (BLamD) - In Detail
Location (Precise)
BLamD sits above the RPE's own basement membrane, i.e., between the basal plasma membrane of the RPE cell and the basal lamina of the RPE. It is intra-RPE-basement-complex material.
RPE cell body
↓ ← BLamD sits HERE (between cell and its own basement membrane)
RPE basement membrane (= innermost layer of Bruch's)
↓ ← BLinD and drusen sit HERE
Inner collagenous layer of Bruch's
Elastic fibre layer
Outer collagenous layer
Choriocapillaris basement membrane
Choriocapillaris
Composition
- Wide-spaced collagen (periodicity ~100 nm on electron microscopy - characteristic)
- Fibronectin
- Laminin
- Abnormal basement membrane material secreted by dysfunctional RPE cells
How It Forms
Dysfunctional RPE cells, under oxidative stress and with age, secrete abnormal extracellular matrix material that cannot be cleared. This accumulates between the cell's basal surface and its own basement membrane. It represents a failure of normal RPE basement membrane turnover.
Key Features
- Seen on electron microscopy (not visible on light microscopy or clinical imaging easily)
- Present in virtually all eyes over 50 years to some degree - so it is part of normal ageing as well as AMD
- In AMD, it is thicker and more abnormal in composition
- It is diffuse (spreads under the entire RPE) rather than focal like drusen
- On OCT, BLamD corresponds to the recently described finding of "outer retinal corrugations" - an undulating hyper-reflective layer beneath the RPE band
Clinical Significance in AMD
- Barrier to nutrition: BLamD thickens the space between the RPE cell and its nutrient supply (choriocapillaris), impairing oxygen/glucose diffusion to the RPE
- Impairs RPE adhesion: Normal RPE adhesion to Bruch's membrane depends on direct cell-basement membrane contact. BLamD physically separates them, predisposing to RPE detachment
- Promotes drusen formation: BLamD disrupts normal RPE function, leading to increased secretion of BLinD material which then forms drusen
- Complement activation: Components within BLamD trigger the complement cascade, driving the AMD inflammatory cycle
- Precedes visible drusen: BLamD is often the earliest histological change detectable in AMD eyes, appearing before drusen are visible clinically
Basal Linear Deposit (BLinD) - Why It Matters More for Drusen
BLinD is the clinically more important precursor to drusen formation:
- Sits in the same sub-RPE-basement-membrane space as drusen
- When BLinD accumulates focally and mounds up, it creates what we clinically call a soft druse
- BLinD contains membrane fragments and lipid-rich material derived from partial degradation of photoreceptor outer segments that the RPE could not fully process
- The lipid in BLinD is derived from RPE lysosomes - it is essentially undigested outer segment material
This is why soft drusen (arising from BLinD) carry higher AMD risk than hard drusen (which arise by a different calcification/deposit mechanism).
Simple Memory Diagram
AMD deposit hierarchy (inner → outer relative to RPE):
[RPE cell]
↑
BLamD (between cell body and its own basement membrane)
= Wide-spaced collagen; diffuse; earliest change
[RPE BASEMENT MEMBRANE] ← this is the inner layer of Bruch's
↑
BLinD (between RPE basement membrane and inner collagenous layer)
= Membranous/lipid debris; focal accumulation
↓
Focal mounding of BLinD = SOFT DRUSEN (clinically visible)
[INNER COLLAGENOUS LAYER OF BRUCH'S]
On OCT in AMD
| Finding | Histological Correlate |
|---|---|
| Outer retinal corrugations (undulating hyper-reflective layer beneath RPE) | BLamD |
| Sub-RPE hyperreflective material (flat, diffuse) | BLinD |
| Focal sub-RPE dome-shaped elevation | Soft druse |
| RPE elevation with overlying photoreceptor loss | Late BLamD + GA |
Summary
BLamD is the earliest ultrastructural lesion in AMD - abnormal fibrous material secreted by dysfunctional RPE that accumulates between the RPE cell and its own basement membrane. It impairs RPE nutrition, promotes detachment, drives complement activation, and precedes visible drusen. It is distinct from BLinD (which sits below the RPE basement membrane and directly forms soft drusen) and from drusen themselves (which are focal mounds of BLinD). The three are part of the same pathological continuum: RPE dysfunction → BLamD → BLinD → soft drusen → AMD progression.
This is a shared conversation. Sign in to Orris to start your own chat.