Diffusion capacity of lungs full details for md exams
Reading File
search_medical_text
diffusion capacity of lungs DLCO measurement physiology
search_medical_text
DLCO decreased increased conditions clinical interpretation obstructive restrictive
search_medical_image
diffusion capacity DLCO lung diagram alveolar capillary membrane
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive breakdown of Diffusion Capacity of the Lungs (DLCO) for MD exam preparation:
Diffusion Capacity of the Lungs (DLCO)
1. Definition
DLCO (Diffusing Capacity of the Lung for Carbon Monoxide) measures the ability of the lungs to transfer gas from the alveolar space into the pulmonary capillary blood. It specifically quantifies the rate of gas transfer per unit of driving pressure (partial pressure gradient).
Formula: D = V̇gas / (P1 − P2)
- D = Diffusing capacity (mL/min/mmHg)
- V̇gas = Volume of gas transferred per minute
- P1 − P2 = Partial pressure gradient across the membrane
2. Why Carbon Monoxide (CO) is Used
| Property | Significance |
|---|---|
| CO has very high affinity for Hb (210× > O₂) | Capillary PCO ≈ 0, so back-pressure is negligible |
| Entire gradient is across the alveolar membrane | Makes diffusion the rate-limiting step (not perfusion) |
| Safe in trace amounts | Can be used clinically |
CO is therefore a pure diffusion-limited gas — ideal for measuring membrane transfer capacity.
3. Technique — Single-Breath DLCO (Most Common)
- Patient exhales to RV
- Inhales a test gas mixture (0.3% CO + 10% He + 21% O₂ + N₂) to TLC
- Breath-hold for 10 seconds
- Exhales; alveolar sample is collected
- CO disappearance is measured to calculate DLCO
Normal DLCO: ~25 mL/min/mmHg (varies with age, sex, body surface area, Hb)
4. Components of DLCO — Fick's Law Applied
DLCO depends on:
| Component | Factor |
|---|---|
| Membrane diffusing capacity (Dm) | Thickness, surface area of alveolar-capillary membrane |
| Capillary blood volume (Vc) | Volume of blood in pulmonary capillaries |
| θ (Theta) | Reaction rate of CO with Hb |
1/DLCO = 1/Dm + 1/(θ × Vc) (Roughton-Forster equation — high-yield for exams)
5. Factors Affecting DLCO
✅ Physiological Determinants
| Factor | Effect on DLCO |
|---|---|
| Large body/BSA | ↑ (more lung surface area) |
| Exercise | ↑ (recruits more capillaries) |
| Supine position | ↑ (better perfusion of upper zones) |
| High altitude | ↓ (lower PO₂, but DLCO itself not greatly affected) |
| Age | ↓ (alveolar surface area decreases) |
| Female sex | Slightly lower than males |
✅ Hematological Correction (Important for Exams!)
DLCO must be corrected for hemoglobin:
- Anemia → ↓ DLCO (less Hb to bind CO)
- Polycythemia → ↑ DLCO (more Hb available)
Correction formula:
DLCOcorrected = DLCOmeasured × [(10.22 + Hb) / (1.7 × Hb)]
6. DLCO — Causes of Decrease vs. Increase
⬇️ Decreased DLCO
| Category | Examples |
|---|---|
| Membrane thickening | Pulmonary fibrosis (IPF), sarcoidosis, pneumoconiosis |
| Alveolar destruction | Emphysema (most common obstructive cause) |
| Pulmonary vascular | Pulmonary hypertension, pulmonary embolism, vasculitis |
| Reduced capillary blood | Anemia, post-pneumonectomy |
| Infiltration | Interstitial lung disease (ILD) |
| Other | Smoking, diabetes (microangiopathy) |
⬆️ Increased DLCO
| Cause | Mechanism |
|---|---|
| Pulmonary hemorrhage (Goodpasture's, Wegener's) | Free Hb in alveoli binds CO |
| Polycythemia vera | More Hb available |
| Left-to-right cardiac shunt | Increased pulmonary blood flow |
| Asthma | Increased pulmonary blood volume |
| Obesity | Increased blood flow |
| Exercise | Capillary recruitment |
| Supine position | Increased perfusion |
High-yield pearl: DLCO is the ONLY PFT abnormality in pulmonary hemorrhage — it is elevated because free alveolar Hb binds CO.
7. DLCO in Pattern Recognition (PFT Interpretation)
| Pattern | FEV1/FVC | TLC | DLCO |
|---|---|---|---|
| Emphysema | ↓ | ↑ | ↓↓ |
| Chronic bronchitis | ↓ | Normal/↑ | Normal |
| Asthma | ↓ (reversible) | Normal/↑ | Normal or ↑ |
| IPF / ILD | Normal or ↑ | ↓ | ↓↓ |
| Pulmonary hypertension | Normal | Normal | ↓ |
| Pulmonary hemorrhage | Normal | Normal | ↑↑ |
| Neuromuscular disease | Normal or ↑ | ↓ | Normal |
| Obesity | Normal | ↓ | Normal or ↑ |
Key distinction: Both emphysema and ILD have ↓ DLCO. Emphysema has ↑ TLC (air trapping); ILD has ↓ TLC (restriction).
8. KCO (Transfer Coefficient) — DLCO/VA
KCO = DLCO / VA (where VA = alveolar volume)
This corrects DLCO for lung volume. It answers: "Is the DLCO low because there's less lung, or because the remaining lung is sick?"
| Scenario | DLCO | VA | KCO | Interpretation |
|---|---|---|---|---|
| Pneumonectomy | ↓ | ↓ | Normal | Less lung, but remaining is healthy |
| Emphysema | ↓ | ↑ or N | ↓↓ | Alveolar destruction |
| ILD | ↓ | ↓ | Normal or ↓ | Less lung + membrane disease |
| Pulmonary vascular disease | ↓ | Normal | ↓ | Vascular problem, not alveolar |
| Pulmonary hemorrhage | ↑ | Normal | ↑ | Extra CO uptake |
9. Diagnostic Interpretation Flowchart
(ERS/ATS Technical Standard)
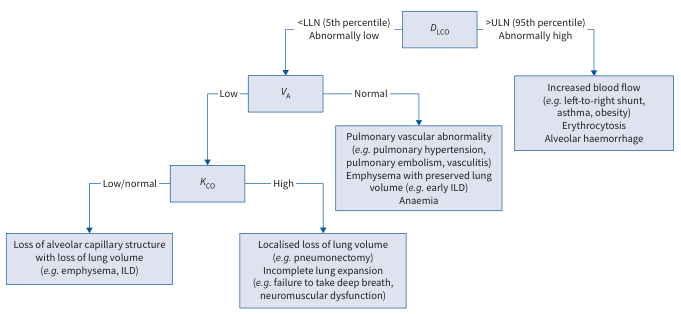
Algorithmic approach:
- DLCO < LLN (5th percentile):
- VA low → check KCO:
- KCO low/normal → Loss of alveolar-capillary structure (emphysema, ILD)
- KCO high → Localized volume loss (pneumonectomy, neuromuscular disease)
- VA normal → Pulmonary vascular (PH, PE, vasculitis), early ILD, anemia
- VA low → check KCO:
- DLCO > ULN (95th percentile): Left-to-right shunt, erythrocytosis, alveolar hemorrhage
(Technical Standard on Interpretive Strategies for Routine Lung Function Tests, p. 24)
10. Grading of DLCO Reduction (ERS/ATS)
| Grade | % Predicted |
|---|---|
| Normal | ≥ 75% |
| Mild reduction | 60–74% |
| Moderate reduction | 40–59% |
| Severe reduction | < 40% |
11. Clinical Scenarios — High-Yield Exam Points
-
Emphysema vs. Chronic Bronchitis: Both are COPD, but DLCO is low only in emphysema (alveolar wall destruction reduces surface area).
-
Pulmonary Fibrosis: Restriction + ↓ DLCO = hallmark combo. DLCO may fall before FVC in early disease.
-
Goodpasture Syndrome / DAH: ↑ DLCO is the clue — free alveolar Hb acts as an "extra sink" for CO.
-
Pre-operative assessment: DLCO < 40% predicted → high risk for post-operative pulmonary complications; consider it in lung resection planning.
-
Scleroderma: Isolated ↓ DLCO with normal spirometry suggests early pulmonary vascular disease (pre-clinical PH).
-
Anemia correction: Always correct DLCO for Hb before interpreting — anemia can artifactually lower DLCO.
-
Altitude: Reduced inspired PO₂ does not significantly alter DLCO measurement because CO gradient is still maintained.
12. Summary Table — High-Yield One-Liners
| Fact | Detail |
|---|---|
| Gas used | Carbon monoxide (CO) |
| Technique | Single-breath, 10-second breath hold |
| Normal value | ~25 mL/min/mmHg |
| Key equation | 1/DLCO = 1/Dm + 1/(θ × Vc) |
| Only ↑ DLCO in lung disease | Pulmonary hemorrhage (DAH) |
| DLCO ↓ in COPD | Emphysema only (not chronic bronchitis) |
| Best corrected by | Hemoglobin level |
| Differentiates | Emphysema (↑TLC + ↓DLCO) vs ILD (↓TLC + ↓DLCO) |
| KCO normal + ↓DLCO | Pneumonectomy / localized volume loss |
| KCO ↓ + ↓DLCO | Emphysema / ILD / vascular disease |
Sources: Harrison's Principles of Internal Medicine, 21st Ed. (pp. 7850, 7873); ERS/ATS Technical Standard on Interpretive Strategies for Routine Lung Function Tests (p. 24)
This is a shared conversation. Sign in to Orris to start your own chat.