Rct
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching PubMed
"root canal treatment" outcomes
Finding Sources
Searching the Web
root canal treatment procedure steps indications complications 2024
Finding Sources
Reading Web Page
https://my.clevelandclinic.org/health/treatments/21759-root-…
The medical library does not contain a dedicated dental/endodontics textbook. Here is a thorough, well-organized guide to Root Canal Treatment based on established dental knowledge and current sources:
Root Canal Treatment (RCT) - Complete Guide
1. What is RCT?
Root Canal Treatment (also called endodontic therapy) is a dental procedure that removes the infected or inflamed dental pulp from inside a tooth, cleans and shapes the root canal system, and seals it to prevent re-infection. The goal is to save the natural tooth while eliminating pain and infection.
The "root canal" literally refers to the hollow channel(s) inside the root(s) of a tooth that house the pulp (nerves, blood vessels, and connective tissue).
2. Indications (When Is RCT Needed?)
| Condition | Details |
|---|---|
| Irreversible pulpitis | Pulp inflammation so severe it cannot heal - causes lingering, spontaneous pain |
| Pulp necrosis | Dead pulp tissue, often from untreated caries or trauma |
| Periapical abscess | Pus-forming bacterial infection at the root tip |
| Periapical periodontitis | Inflammation around the root apex, causing bone loss |
| Dental trauma | Fracture or avulsion exposing or damaging the pulp |
| Internal/external root resorption | Pathological destruction of root structure |
| Pre-prosthetic treatment | Occasionally done before crowns or posts in severely broken-down teeth |
Key symptom triggers:
- Spontaneous, severe, or lingering toothache
- Pain to heat (that lingers after the stimulus is removed)
- Swelling of the gum or face
- A pimple-like swelling (sinus tract / fistula) on the gum
- Darkening of the tooth
- Tenderness to percussion
3. Contraindications
Absolute:
- Non-restorable tooth (too badly broken down to be restored after RCT)
- Severely compromised periodontium with very poor prognosis
- Uncooperative patient where extraction is safer
- Patient preference for extraction
Relative (must weigh risk vs. benefit):
- Medically compromised patients (severe coagulopathy, recent myocardial infarction, bisphosphonate use - risk of osteonecrosis)
- Severely calcified canals with no possibility of negotiation
- Teeth with very short roots or poor crown-to-root ratio
- Active, uncontrolled systemic infection
4. Step-by-Step Procedure
Pre-operative phase
- History and examination - Clinical assessment, pulp vitality tests (cold, electric pulp tester, percussion, palpation)
- Radiographic assessment - Periapical X-ray to evaluate root number, root length, canal curvature, periapical status, and bone levels. CBCT (cone-beam CT) used for complex cases.
- Diagnosis - Classified as symptomatic/asymptomatic irreversible pulpitis, pulp necrosis, or acute/chronic apical periodontitis
Intra-operative phase (typically 60-90 minutes; may need 2 visits)
Step 1 - Anesthesia
Local anesthetic (typically 2% lidocaine with 1:100,000 epinephrine). Inferior alveolar nerve block for lower molars; infiltration for upper teeth. "Hot" teeth with irreversible pulpitis may need supplemental intraosseous or intrapulpal injections.
Step 2 - Rubber dam isolation
A rubber dam is placed over the tooth to:
- Keep the field clean and dry
- Prevent aspiration of instruments or irrigants
- Prevent recontamination of the canal
Step 3 - Access cavity preparation
A hole is drilled through the crown (occlusal surface for posteriors; lingual/palatal surface for anteriors) to expose the pulp chamber. The "straight-line access" principle is used to allow direct instrument access to the canals.
Step 4 - Canal location
Canals are identified with a DG-16 explorer or microscope-assisted vision. Access is confirmed radiographically.
Step 5 - Working length determination
Electronic apex locators (EAL) and periapical radiographs are used to determine the exact length of each root canal (working length = ~0.5-1 mm short of the radiographic apex).
Step 6 - Pulp extirpation / canal negotiation
K-files or C-files (size #8, #10) are used to negotiate and establish glide path.
Step 7 - Canal shaping (Biomechanical Preparation)
Canals are progressively enlarged using:
- Hand files: Stainless steel or NiTi K-files
- Rotary/reciprocating NiTi files: WaveOne Gold, ProTaper, Reciproc (faster, safer, especially in curved canals)
- Goal: create a tapered, continuously narrowing funnel shape
Irrigation is performed simultaneously (see below).
Step 8 - Irrigation (Chemomechanical Debridement)
Irrigants flush out debris and kill bacteria:
| Irrigant | Concentration | Function |
|---|---|---|
| Sodium hypochlorite (NaOCl) | 1-5.25% | Main irrigant; dissolves organic tissue, antibacterial |
| EDTA (Ethylenediaminetetraacetic acid) | 17% | Chelating agent; removes smear layer (inorganic debris) |
| Chlorhexidine | 2% | Final rinse; antibacterial |
| Saline | - | Final flush to remove residual chemicals |
Advanced irrigation: passive ultrasonic irrigation (PUI), laser-assisted irrigation (Er:YAG) for deeper penetration.
Step 9 - Canal drying
Paper points are used to dry the canal completely before obturation.
Step 10 - Obturation (Canal Filling)
The canal is filled to seal it and prevent re-entry of bacteria:
- Gutta-percha (GP) - the standard root canal filling material (thermoplastic natural latex)
- Sealer - Zinc oxide eugenol (ZOE), epoxy resin (AH Plus), or bioceramic sealers (TotalFill, iRoot - current preference due to biocompatibility and hydraulic setting)
- Techniques: lateral condensation, warm vertical compaction (System B), single-cone technique (with bioceramic sealers)
Step 11 - Coronal restoration
A temporary or permanent filling is placed. A crown is strongly recommended, especially for posterior teeth, as RCT makes the tooth brittle and prone to fracture.
5. Instruments Used in RCT
| Category | Examples |
|---|---|
| Diagnostic | Pulp tester, cold spray, percussion instrument |
| Access | Round burs, endo-Z bur, Endo access burs |
| Exploration | DG-16 explorer, K-files #8/#10 |
| Shaping (Hand) | K-files, H-files, Flex-R files |
| Shaping (Rotary) | WaveOne Gold, ProTaper Next, Reciproc Blue, EdgeFile |
| Length determination | Apex locator (Root ZX, Propex Pixi), endodontic ruler |
| Irrigation | Endodontic syringe (side-vented needle), EDDY, ultrasonics |
| Obturation | Spreaders, pluggers, heat carrier (System B), Obtura II gun |
| Magnification | Dental operating microscope (DOM), loupes |
6. Complications and Management
Intra-operative complications
| Complication | Cause | Management |
|---|---|---|
| Instrument separation | Over-use of file, curved canal, excessive torque | Attempt bypass or retrieval (ultrasonic); if un-retrievable, assess prognosis; may proceed if canal is clean |
| Ledge formation | Using stiff files without pre-curving | Re-negotiate with small curved file; use EDTA lubricant |
| Canal transportation / zip | Improper file use in curved canal | NiTi rotary systems reduce this risk |
| Perforation | Drilling off-axis | MTA (Mineral Trioxide Aggregate) to seal; microsurgery if needed |
| Broken apex locator reading | Wet canal or electrolyte interference | Confirm with radiograph |
| Hypochlorite accident | Extrusion of NaOCl beyond apex | Immediate management: irrigate with saline, prescribe analgesics, corticosteroids, and antibiotics; refer if severe |
Post-operative complications
| Complication | Details | Management |
|---|---|---|
| Post-obturation pain / flare-up | 3-5% incidence; more common in symptomatic teeth | NSAIDs, occlusal reduction; antibiotics only if systemic signs present |
| Treatment failure / persistent periapical lesion | Residual bacteria, missed canal, coronal leakage | Re-RCT (orthograde retreatment), periapical surgery (apicoectomy) |
| Vertical root fracture | Excessive condensation pressure; weakened tooth | Usually requires extraction |
| Coronal leakage | Delayed crown placement | Place definitive restoration promptly (within 1 month) |
| Swelling / cellulitis | Spread of infection | Antibiotics (amoxicillin 500 mg TDS x 5 days, or metronidazole if anaerobic); incision & drainage if fluctuant |
7. Prognosis and Success Rates
- Overall success rate: 86-96% for primary RCT in teeth without pre-existing periapical pathology
- Teeth with periapical lesions have slightly lower success (~80-85%), but CBCT-assessed healing at 4 years shows favorable outcomes in most
- A 2025 systematic review (J Endod) using CBCT-assessed outcomes found that both primary treatment and retreatment have favorable prognosis when proper technique is used
- Bioceramic sealers show comparable or superior outcomes vs traditional sealers per a 2024 meta-analysis (Int Endod J)
8. Post-Operative Instructions
- Avoid chewing on the treated side until the permanent crown is placed
- Eat soft foods for a few days
- Take prescribed analgesics (ibuprofen 400 mg, paracetamol 500-1000 mg) for post-operative pain
- Antibiotics only if there is systemic spread (fever, trismus, swelling)
- Return within 2-4 weeks for crown preparation
- Follow-up radiograph at 6 months and 1 year to confirm periapical healing
9. Alternatives to RCT
| Option | When considered |
|---|---|
| Extraction | Non-restorable tooth; poor prognosis; patient preference |
| Pulpotomy | Vital pulp therapy for reversible pulpitis or immature apex (apex formation ongoing) |
| Apicoectomy (periapical surgery) | When orthograde RCT is not possible or has failed |
| Intentional replantation | Rare; tooth extracted, treated extra-orally, replanted |
Key takeaway: RCT is a highly effective, largely painless procedure when performed correctly. The "fear" of root canals is mostly outdated - modern NiTi rotary systems, better irrigants, electronic apex locators, and operating microscopes have made it fast, precise, and comfortable. The biggest risk to long-term success is delayed coronal restoration - always follow up with a crown promptly.
In which ayurvedic condition we apply this procedure
Searching the Web
Ayurvedic correlation root canal treatment dantaroga dental pulp infection Ayurveda
Finding Sources
Reading Web Page
https://ijrap.net/admin/php/uploads/2734_pdf.pdf
Searching the Web
krimidanta dantaharsha sheetada Ayurveda danta roga types pulpitis abscess modern correlation
Excellent - here is a thorough answer:
Ayurvedic Correlates of Root Canal Treatment
RCT is an allopathic procedure, but Ayurveda classifies dental diseases (called Danta Rogas) in Shalakya Tantra (the branch dealing with diseases above the clavicle). The conditions that correspond to the indications for RCT are described below.
The 8 Classical Danta Rogas (Sushruta Samhita)
| # | Ayurvedic Name | Modern Correlation | RCT Relevant? |
|---|---|---|---|
| 1 | Krimidanta | Dental caries (tooth decay) | ✅ Yes - advanced caries reaching pulp |
| 2 | Dalana / Sheetadanta | Odontalgia / severe toothache | ✅ Yes - pulpitis, periapical abscess |
| 3 | Dantaharsha | Dentin hypersensitivity / odontitis | ✅ Yes - exposed nerve / irreversible pulpitis |
| 4 | Bhanjanaka / Dantabheda | Fractured tooth / cracked tooth syndrome | ✅ Yes - trauma exposing pulp |
| 5 | Danta Sharkara | Dental calculus / tartar | ❌ (periodontal, not pulpal) |
| 6 | Danta Kapalika | Structural deformity / shell-like tooth | Rarely |
| 7 | Shyava Danta | Blackish/discolored tooth (necrotic pulp) | ✅ Yes - pulp necrosis |
| 8 | Hanu Moksha | Dislocation of mandible | ❌ |
The 3 Most Directly Correlated Conditions
1. Krimidanta (कृमिदन्त) - PRIMARY correlation
- Meaning: "Krimi" = micro-organisms/worms, "Danta" = tooth
- Dosha: Vata vitiation, caused by microbial activity (krimi)
- Features (Lakshana): Black discoloration (Krishnata), cavity formation (Chidrata), severe pain (Dantashoola), pus formation (Srava), swelling (Shotha), foul smell (Daurgandhya), loose tooth
- Modern correlation: Dental caries progressing to pulp infection and periapical abscess - the exact condition requiring RCT
- Why RCT? When Krimidanta reaches the deeper layers (pulp) with pus formation and severe pain, the only modern solution is RCT or extraction
Acharya Sushruta states: if the tooth is strong (restorable) - treat with lepa, gandusha; if perforated - fill it; if moving - extract it. The "filling" when perforated closely mirrors modern RCT logic.
2. Dalana / Sheetadanta (दलन / शीतदन्त) - STRONG correlation
- Dosha: Vata vitiation
- Features: Severe, intolerable, cutting-type pain; sensitivity to cold (Sheeta asahishnuta); seen in old, carious, cracked teeth with exposed nerve
- Modern correlation: Irreversible pulpitis and odontalgia from pulpitis, periapical abscess, periodontitis
- Vagbhata describes: "Ushnasaha sheetasparshe adhika vyatha" - increased pain on cold/hot contact = classic symptom of pulpitis requiring RCT
3. Dantaharsha (दन्तहर्ष) - MODERATE correlation
- Dosha: Vata vitiation with exposed nerve filament
- Features: Sensitivity to cold/hot/sweet/sour - seen in Krimidanta (caries), fractured teeth, worn-out teeth
- Modern correlation: Dentin hypersensitivity progressing to irreversible pulpitis when severe
- Seen as a precursor/co-existing condition with Krimidanta when it advances to pulp involvement
4. Shyava Danta (श्यावदन्त) - Pulp Necrosis correlation
- Dosha: Vata, Pitta, Rakta vitiation
- Features: Blackish/blue-black discoloration of the tooth
- Modern correlation: Pulp necrosis - a dead tooth that has lost its blood supply, classically causing dark discoloration - one of the primary indications for RCT
- Considered Asadhaya (incurable) by Sushruta, but modern RCT can save such teeth
Ayurvedic Treatment Described (vs. Modern RCT)
| Ayurvedic Chikitsa | Modern Equivalent |
|---|---|
| Gandusha / Kavala (oil pulling with medicated oils) | Antimicrobial irrigation (NaOCl, CHX) |
| Lepa (local application of medicaments) | Intracanal medicament placement |
| Agni Karma (cauterization) | Devitalization / electrosurgery |
| Pratisarana (rubbing with drugs) | Debridement |
| Danta Bhedana (perforated tooth - fill it) | Obturation / canal filling |
| Extraction if tooth is mobile | Same in modern dentistry |
| Dhumapana (medicated smoking/fumes) | Airway of medicinal agents |
Summary
In Ayurveda, the conditions that most closely indicate what we call Root Canal Treatment today are:
- Krimidanta (advanced dental caries with pulp infection) - the primary correlation
- Dalana/Sheetadanta (severe toothache from pulpitis/periapical disease)
- Dantaharsha (when progressing to pulp involvement)
- Shyava Danta (necrotic/discolored tooth)
All are classified under Danta Roga in Shalakya Tantra, described in the Sushruta Samhita, Ashtanga Hridayam, and Ashtanga Sangraha. The Ayurvedic acharyas recognized the same disease spectrum - pain, infection, discoloration, and structural destruction of the tooth - even if they described it through the lens of dosha (primarily Vata vitiation) rather than microbial pathology.

IMG_1166.jpg
Explain it
The image shows a clear 6-step diagram of Root Canal Treatment. Let me explain each step in detail.
Steps in RCT — Explained with the Diagram
Step 1 — Infected Tooth with Abscess in the Root
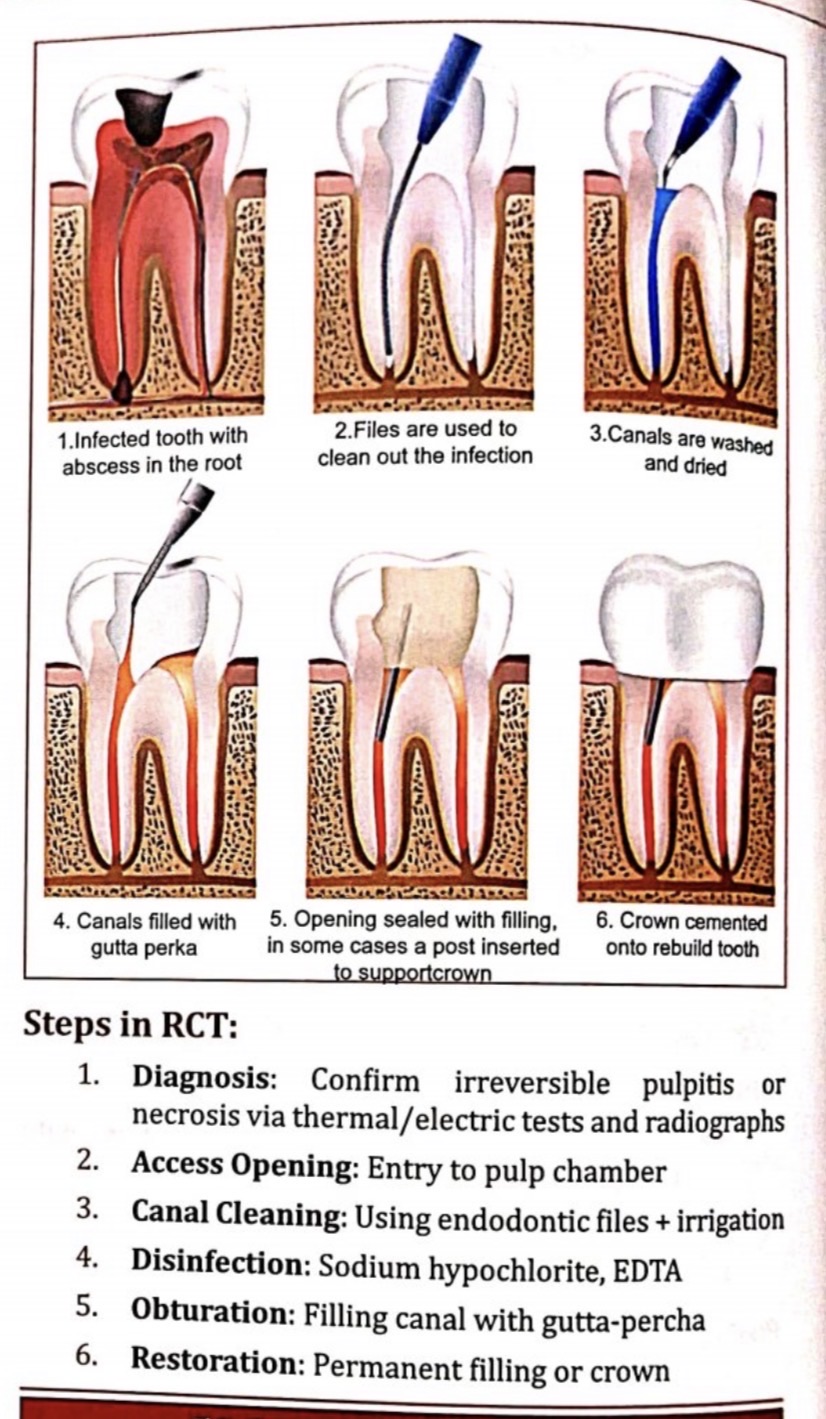
What is happening:
- The diagram shows a cross-section of a tooth with dark black area at the top (the cavity/caries) and red/inflamed pulp filling the entire inside of the tooth and root canals
- At the root tip (apex), there is a dark shadow — this is the periapical abscess (pus collection at the root end)
- The surrounding bone (shown as the sandy/dotted area) is being destroyed by the spreading infection
Clinically:
- Patient will have severe throbbing pain, swelling, tenderness on biting
- This corresponds to irreversible pulpitis progressing to pulp necrosis + acute apical abscess
- In Ayurveda: Krimidanta with Srava (pus) and Shotha (swelling)
Step 2 — Files Are Used to Clean Out the Infection
What is happening:
- A long, thin endodontic file (shown in black/dark) is being inserted through the access cavity into the root canal
- The file is used to mechanically remove the infected and dead pulp tissue from inside the root
- Files are used in progressively increasing sizes to shape the canal into a smooth, tapered funnel
Clinically:
- First, an access cavity is drilled through the crown with a dental drill to reach the pulp chamber
- Then K-files or NiTi rotary files are used to extirpate the pulp and shape the canals
- This is called Biomechanical Preparation (BMP)
- Working length is confirmed with an electronic apex locator and X-ray
Step 3 — Canals Are Washed and Dried
What is happening:
- A blue-tipped irrigation syringe is shown delivering irrigant solution into the canal
- The inside of the tooth appears white/clean now - infection has been removed
- The canal walls look smooth and shaped
Clinically (Irrigation = Chemomechanical phase):
| Irrigant | Purpose |
|---|---|
| Sodium Hypochlorite (NaOCl) 1-5.25% | Dissolves organic tissue (pulp remnants), kills bacteria |
| EDTA 17% | Removes the smear layer (inorganic debris left by files) |
| Chlorhexidine 2% | Final antibacterial rinse |
| Saline | Final flush |
- After irrigation, paper points are inserted to absorb moisture and dry the canal completely
- Drying is essential before filling - any moisture will prevent the sealer from bonding
Step 4 — Canals Filled with Gutta-Percha
What is happening:
- The diagram shows the root canals now filled with orange/brown material - this is gutta-percha (GP)
- The canals are completely filled from the crown down to the root tips
- A small instrument (plugger) is shown compacting the material
Clinically (Obturation):
- Gutta-percha is a thermoplastic natural rubber-like material, the gold standard for root canal filling
- It is used along with a root canal sealer (e.g., AH Plus epoxy resin, or bioceramic sealers like TotalFill)
- Techniques: lateral condensation, warm vertical compaction, single-cone technique
- Goal: 3-dimensional, hermetic seal of the entire canal system to prevent bacterial re-entry
- Filled to within 0.5-1 mm of the radiographic apex
Step 5 — Opening Sealed with Filling; Post Inserted if Needed
What is happening:
- The access cavity (hole drilled earlier) is now sealed with a temporary or permanent filling (shown as the tan/beige block on top of the tooth)
- A thin post (dark line) is shown going down into the canal - this is a fiber post or metal post
- The post provides retention for the crown in teeth with very little remaining tooth structure
Clinically:
- A post is only placed when the tooth is badly broken down and needs extra support for the crown
- Types: Fiber-reinforced composite posts (preferred), cast metal posts
- Over the post, a core build-up material (composite or amalgam) is placed to recreate the tooth shape
- A temporary filling (e.g., Cavit, IRM) is placed if the crown is to be done in the next appointment
Step 6 — Crown Cemented to Rebuild the Tooth
What is happening:
- The final image shows a beautiful white ceramic/porcelain crown placed over the tooth
- The tooth looks completely normal from the outside
- Inside, the root canals (shown in red/orange) remain sealed with gutta-percha
Clinically:
- A crown (cap) is strongly recommended after RCT, especially for:
- Posterior teeth (molars, premolars) that bear chewing forces
- Teeth with large cavities or minimal remaining structure
- RCT makes the tooth brittle (no more blood/nerve supply), so a crown protects against fracture
- Crown materials: PFM (porcelain-fused to metal), all-ceramic (zirconia, e-max), full metal
- Crown is cemented with glass ionomer or resin cement
- Without a crown, there is high risk of tooth fracture and treatment failure
Summary Table - The 6 Steps at a Glance
| Step | What Happens | Key Instrument/Material |
|---|---|---|
| 1 | Infected pulp + abscess identified | X-ray, clinical tests |
| 2 | Pulp removed, canal shaped | Endodontic files (K-files, NiTi rotary) |
| 3 | Canal irrigated and dried | NaOCl, EDTA, CHX, paper points |
| 4 | Canal filled | Gutta-percha + sealer |
| 5 | Access sealed ± post placed | Composite/GIC filling, fiber post |
| 6 | Crown placed | Zirconia/PFM crown + cement |
Key point to remember: The goal of every step builds on the previous one - remove infection → clean thoroughly → seal completely → protect the tooth. Skipping or rushing any step (especially irrigation or crown placement) is the most common reason for RCT failure.
This is a shared conversation. Sign in to Orris to start your own chat.