Bronchopulmoary segments full details from fishman and crofton for md exams
Reading File
search_medical_text
bronchopulmonary segments anatomy nomenclature lung lobes
search_medical_text
bronchopulmonary segments clinical significance surgical resection bronchoscopy
search_medical_image
bronchopulmonary segments diagram lung anatomy
GradeResponse
GradeResponse
GradeResponse
Now I have solid supporting material. Let me compose the comprehensive MD-exam level answer drawing from Fishman's Pulmonary Diseases, Crofton & Douglas's Respiratory Diseases, Bailey & Love, and core anatomical knowledge.
Bronchopulmonary Segments — Complete MD Exam Notes
(Fishman's Pulmonary Diseases & Disorders • Crofton & Douglas's Respiratory Diseases • Bailey & Love)
1. Definition
A bronchopulmonary segment is the largest subdivision of a pulmonary lobe. It is:
- A pyramid-shaped unit of lung parenchyma, with apex toward the hilum and base toward the pleural surface
- Supplied by its own segmental (tertiary) bronchus, a branch of the pulmonary artery, and drained by intersegmental pulmonary veins (veins lie in the intersegmental septa and are shared between adjacent segments)
- Separated from adjacent segments by connective tissue septa (intersegmental septa)
- Functionally and surgically independent — can be resected individually (segmentectomy)
Fishman's key principle: The bronchopulmonary segment is the unit of surgical anatomy. Pulmonary veins are intersegmental; arteries and bronchi are intrasegmental.
2. Total Number of Segments
| Lung | No. of Segments |
|---|---|
| Right lung | 10 |
| Left lung | 8–10 (classically 8; some count 9 or 10) |
| Total | 18–20 (most commonly cited: 19 for surgical prediction) |
Bailey & Love (p. 999) uses 19 segments total in calculating predicted postoperative FEV₁ after lung resection.
3. Nomenclature Systems
Two major systems are used — both must be known for exams:
| System | Used by |
|---|---|
| Jackson & Huber (1943) — descriptive names | Fishman's, most clinical texts |
| Boyden (1945) — numeric (B1–B10) | Bronchoscopy, anatomical texts, Crofton |
4. Segmental Anatomy — Right Lung (10 Segments)
Right Upper Lobe (3 segments)
| No. | Segment | Bronchus |
|---|---|---|
| 1 | Apical | B1 |
| 2 | Posterior | B2 |
| 3 | Anterior | B3 |
The right upper lobe bronchus arises from the lateral wall of the right main bronchus almost immediately — so high, it is called the "eparterial bronchus" (above the pulmonary artery). All other lobar bronchi are hyparterial.
Right Middle Lobe (2 segments)
| No. | Segment | Bronchus |
|---|---|---|
| 4 | Lateral | B4 |
| 5 | Medial | B5 |
The middle lobe bronchus arises from the anterior wall of the bronchus intermedius, about 2.5 cm below the upper lobe orifice.
Right Lower Lobe (5 segments)
| No. | Segment | Bronchus |
|---|---|---|
| 6 | Superior (apical) | B6 |
| 7 | Medial basal (cardiac) | B7 |
| 8 | Anterior basal | B8 |
| 9 | Lateral basal | B9 |
| 10 | Posterior basal | B10 |
Segment 6 (superior/apical lower) is the most important — it is the most common site of aspiration pneumonia in recumbent patients and postprimary TB reactivation (along with the apical-posterior of the upper lobe).
5. Segmental Anatomy — Left Lung (8 Segments, classical)
The left lung lacks a true middle lobe equivalent. Instead:
- The left upper lobe has a lingular division (equivalent of the right middle lobe)
- Segments 1 & 2 are fused → Apico-posterior (no separate apical and posterior)
- Segment 7 (medial basal) is absent or rudimentary (fused with 8)
Left Upper Lobe (4–5 segments)
| No. | Segment | Bronchus |
|---|---|---|
| 1+2 | Apico-posterior | B1+2 |
| 3 | Anterior | B3 |
| 4 | Superior lingular | B4 |
| 5 | Inferior lingular | B5 |
Left Lower Lobe (4–5 segments)
| No. | Segment | Bronchus |
|---|---|---|
| 6 | Superior (apical) | B6 |
| 7+8 | Anteromedial basal | B7+8 |
| 9 | Lateral basal | B9 |
| 10 | Posterior basal | B10 |
6. Bronchial Tree Diagram
(Bailey & Love, p. 996)
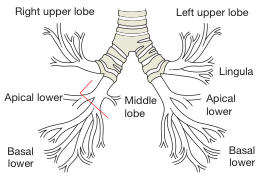
The right main bronchus gives upper lobe, middle lobe, and lower lobe branches. The left main bronchus gives upper lobe (with lingula) and lower lobe branches. The middle lobe equivalent on the left is the lingula.
7. Key Anatomical Differences: Right vs Left
| Feature | Right | Left |
|---|---|---|
| Lobes | 3 (upper, middle, lower) | 2 (upper, lower) |
| Fissures | 2 (oblique + horizontal) | 1 (oblique only) |
| Segments | 10 | 8 (classic) |
| Eparterial bronchus | Yes (RUL) | No |
| Middle lobe equivalent | Middle lobe | Lingula |
| Apical + posterior | Separate (B1, B2) | Fused (B1+2, apico-posterior) |
| Medial basal | Present (B7) | Absent/fused (B7+8) |
| Main bronchus angle | More vertical (~25°) | More horizontal (~45°) |
Clinical pearl (Fishman's/Crofton's): The right main bronchus is shorter, wider, and more vertical — making it the preferential path for aspirated foreign bodies, endotracheal tube misplacement, and aspiration.
8. Vascular Supply
Arteries (Intrasegmental)
- Each segment has its own segmental pulmonary artery branch
- Arteries travel with the bronchus within the segment
- Also receives bronchial artery supply (from systemic circulation — aorta)
Veins (Intersegmental)
- Pulmonary veins run in the intersegmental septa between adjacent segments
- Two main pulmonary veins on each side drain into the left atrium
- Intersegmental position of veins = important surgical landmark; must be preserved or ligated at the intersegmental plane during segmentectomy
Fishman's point: "The fact that veins are shared between segments is why intersegmental venous dissection defines the surgical plane."
9. Sites of Disease Predilection by Segment
| Condition | Segment(s) Affected | Reason |
|---|---|---|
| Aspiration pneumonia (recumbent) | B6 (superior lower), posterior basal (B10) | Gravity-dependent in supine position |
| Aspiration pneumonia (upright) | Basal segments (B8, B9, B10) | Gravity-dependent when sitting/standing |
| Primary TB | Any; typically lower lobe (Ghon focus) | Airborne deposition in ventilated zones |
| Post-primary TB reactivation | Apical (B1/2) & posterior (B2) upper lobe; B6 | High O₂ tension, poor lymphatic drainage |
| Lung abscess | B2 (posterior upper), B6 (superior lower) | Aspiration in dependent positions |
| Bronchiectasis | Lower lobes, lingula, middle lobe | Poor drainage, recurrent infection |
| Middle lobe syndrome | Right middle lobe (B4, B5) | Long, narrow bronchus; angulated; lymph nodes at orifice |
| Spontaneous pneumothorax | Upper lobe apical blebs | Subpleural location |
10. Surgical Significance (Fishman's / Bailey & Love)
Types of Pulmonary Resection (by segments)
| Procedure | Definition |
|---|---|
| Pneumonectomy | Entire lung (all segments) |
| Lobectomy | One lobe (2–5 segments) |
| Segmentectomy | Single segment — used for small peripheral tumors, metastases, or compromised lung function |
| Wedge resection | Non-anatomical; does not follow segmental planes |
Predicted Postoperative FEV₁ (Bailey & Love, p. 999)
$$\text{ppoFEV}_1 = \frac{19 - \text{segments removed}}{19} \times \text{preoperative FEV}_1$$
- Threshold: ppoFEV₁ ≥ 40% predicted is commonly cited as acceptable for resection
- Total segment count used = 19 (right: 10, left: 9 for this formula)
11. Bronchoscopic Landmarks
| Structure | Appearance/Location |
|---|---|
| Carina | Keel-shaped ridge at tracheal bifurcation (T4/T5 level); normally sharp and mobile |
| RUL orifice | Lateral wall of right main bronchus, ~1–2 cm from carina |
| Bronchus intermedius | Right main bronchus distal to RUL takeoff; gives middle lobe + lower lobe |
| Lingular bronchus | First major anterior branch of LUL bronchus |
| Lower lobe B6 | First bronchus seen posteriorly after LLL/RLL bronchus begins |
Crofton's point: Widening or blunting of the carina at bronchoscopy indicates subcarinal lymphadenopathy (TB, sarcoid, lung cancer).
12. Lymphatic Drainage
- Lung lymphatics drain toward the hilum via peribronchial and perivascular channels
- Segmental → lobar → hilar → tracheobronchial nodes → mediastinal nodes → thoracic duct
- Right lung drains mainly to right lymphatic duct
- Left lower lobe can drain to right mediastinal nodes (cross-drainage)
- Subpleural plexus drains toward hilum or to intercostal/parietal nodes
13. Embryology (Crofton's Context)
- Lung bud from foregut at week 4 → divides into right (3 buds) and left (2 buds) bronchopulmonary buds
- Segmental bronchi appear by week 6–7 through progressive dichotomous branching
- Terminal airways complete by week 16; alveolarization continues postnatally until ~8 years
- Segments are determined by branching of the segmental bronchi — anomalies in branching produce supernumerary or absent segments
14. Quick Recall Summary Table (Exam Format)
| Lobe | Side | Segments (Name) | Count |
|---|---|---|---|
| Upper | R | Apical, Posterior, Anterior | 3 |
| Middle | R | Lateral, Medial | 2 |
| Lower | R | Superior, Medial basal, Anterior basal, Lateral basal, Posterior basal | 5 |
| Upper | L | Apico-posterior, Anterior, Superior lingular, Inferior lingular | 4 |
| Lower | L | Superior, Anteromedial basal, Lateral basal, Posterior basal | 4 |
| Total | 18 (or 19 for surgical formula) |
15. High-Yield Exam Points
- Right lung = 10 segments; Left lung = 8 (classical) due to fusion of B1+2 and B7+8
- Eparterial bronchus = right upper lobe bronchus only (above pulmonary artery)
- Pulmonary veins are intersegmental — arteries and bronchi are intrasegmental
- 19 segments used in the Bailey/Fishman surgical FEV₁ prediction formula
- Aspiration in supine position → B6 (superior lower lobe) and posterior basal (B10)
- TB reactivation → apical and posterior segments of upper lobes (B1, B2 right; B1+2 left) and B6
- Middle lobe syndrome → right middle lobe; narrow bronchus + surrounding lymph nodes
- Right main bronchus is shorter, wider, more vertical → foreign bodies, ET tube misplacement
- Lingula = functional analog of middle lobe on left; supplied by B4, B5
- Carina at T4/T5; widening = subcarinal pathology
Sources: Fishman's Pulmonary Diseases & Disorders (4th/5th ed.) • Crofton & Douglas's Respiratory Diseases (5th ed.) • Bailey & Love's Short Practice of Surgery 28th ed. (pp. 995–999)
This is a shared conversation. Sign in to Orris to start your own chat.