thalamic syndrome use guyton and hall and ganong as your reference
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have sufficient content from both Guyton & Hall and Ganong to compose a thorough answer on thalamic syndrome. Let me compile the full response.
Thalamic Syndrome (Dejerine-Roussy Syndrome)
Definition
Thalamic syndrome refers to a cluster of sensory and pain disturbances that arise from a lesion - most commonly an infarct - of the posterolateral thalamus. It is also known as the Dejerine-Roussy syndrome or thalamic pain syndrome. The classic presentation involves an initial contralateral hemisensory loss, followed by the appearance of chronic, often intractable pain on the same affected side as recovery begins.
Physiology of the Thalamus in Sensation (Guyton & Hall)
To understand the syndrome, the normal thalamic role must be appreciated.
Guyton and Hall Textbook of Medical Physiology identifies the thalamus as a key relay and processing center in somatosensory pathways:
"When the somatosensory cortex of a human being is destroyed, that person loses most critical tactile sensibilities, but a slight degree of crude tactile sensibility does return. Therefore, the thalamus (and other lower centers) apparently has a slight ability to discriminate tactile sensation..."
"Conversely, loss of the somatosensory cortex has little effect on one's perception of pain sensation and only a moderate effect on the perception of temperature. Therefore, the lower brain stem, the thalamus, and other associated basal regions of the brain are believed to play dominant roles in discrimination of these sensibilities."
- Guyton and Hall Textbook of Medical Physiology, Chapter 48 (Function of the Thalamus in Somatic Sensation)
This means the thalamus, particularly the ventrobasal complex (VPL and VPM nuclei), is the primary relay station for pain and temperature on their way to the cortex - and also independently contributes to conscious pain perception. Disruption of this structure, therefore, has profound sensory consequences.
Two ascending pain pathways are relevant (Guyton & Hall):
- Neospinothalamic (fast pain): Sharp, well-localized pain travels via A-delta fibers to the VPL nucleus, then to the somatosensory cortex.
- Paleospinothalamic (slow-chronic pain): Diffuse, burning pain via C-fibers terminates in reticular formation, intralaminar and ventrolateral nuclei of the thalamus. Only 10-25% of these fibers reach the thalamus directly.
"Electrical stimulation in the reticular areas of the brain stem and in the intralaminar nuclei of the thalamus, the areas where the slow-suffering type of pain terminates, has a strong arousal effect on nervous activity throughout the entire brain."
- Guyton and Hall, Chapter 49 (Paleospinothalamic Pathway)
Thalamic Syndrome - Pathophysiology (Guyton & Hall)
Guyton & Hall explains thalamic lesions in the context of secondary hyperalgesia:
"Secondary hyperalgesia frequently results from lesions in the spinal cord or the thalamus."
- Guyton and Hall, Chapter 49 (Some Clinical Abnormalities of Pain and Other Somatic Sensations)
When the thalamus is infarcted, the initial result is loss of sensation. However, as partial recovery occurs, the damaged thalamic circuitry - particularly the ventroposterior nuclei - becomes hyperexcitable or disinhibited. The thalamus, which normally integrates and modulates pain signals, now generates spontaneous, dysesthetic pain without adequate peripheral input.
The complete removal of somatosensory cortex does not eliminate pain, underlining that the thalamus itself is a primary seat of pain consciousness. When it is damaged, this pain-generating role becomes pathologically amplified.
Thalamic Syndrome - Direct Description (Ganong)
Ganong's Review of Medical Physiology (26th Edition) describes the syndrome directly within its discussion of CNS lesion effects:
"An infarct in the thalamus can lead to a loss of sensation. Thalamic pain syndrome can occur during recovery from a thalamic infarct. The syndrome is characterized by chronic pain on the side of the body contralateral to the stroke."
- Ganong's Review of Medical Physiology, 26th Ed., Chapter 8 (Effects of CNS Lesions)
Ganong also explains the broader context of thalamic damage: damage to the somatosensory pathways (specifically the ventrolateral spinothalamic tract, which synapses in the VPL nucleus of the thalamus) leads to contralateral loss of pain and temperature. When recovery is partial or the lesion is incomplete, abnormal central sensitization generates the pain syndrome.
Summary of Clinical Features
Drawing from both texts, the hallmarks of thalamic syndrome are:
| Feature | Basis (from Guyton & Ganong) |
|---|---|
| Contralateral hemisensory loss (initial) | Infarct destroys VPL/VPM nuclei - relay for all somatosensory modalities lost |
| Spontaneous chronic pain (contralateral) | Partial recovery with thalamic disinhibition/hyperexcitability - thalamus is a major pain-conscious center |
| Allodynia / hyperpathia | Secondary hyperalgesia from facilitation of sensory transmission in damaged thalamic circuits |
| Loss of pain and temperature | Interruption of spinothalamic tract input to thalamus |
| Relative preservation of crude touch | Partial transmission via other routes (reticular formation, brainstem) |
| Dysesthesias | Aberrant spontaneous discharge from damaged thalamic relay cells |
Key Mechanisms (Synthesis)
-
Initial phase: The thalamic infarct (typically in the territory of the thalamogeniculate artery, supplying the VPL) destroys the relay nucleus for all somatosensory modalities - producing contralateral hemisensory loss for pain, temperature, touch, vibration, and proprioception.
-
Recovery phase: As Ganong notes, during recovery the damaged circuits become aberrantly active. Because the thalamus (not just the cortex) is the primary seat of pain and temperature consciousness per Guyton & Hall, damage here produces spontaneous pain rather than simply a deficit.
-
Chronic pain: The slow-chronic paleospinothalamic pathway terminates in intralaminar nuclei of the thalamus. Damage to adjacent ventroposterior nuclei may disinhibit these intralaminar nuclei, generating persistent, poorly-localized burning pain - exactly the type Guyton & Hall attributes to the slow C-fiber system.
Cause
Most commonly caused by:
- Thalamic infarct (most common) - occlusion of thalamogeniculate branches of the posterior cerebral artery
- Thalamic hemorrhage
- Thalamic tumors or demyelination (less common)
References:
- Guyton and Hall Textbook of Medical Physiology - Chapters 48 ("Function of the Thalamus in Somatic Sensation") and 49 ("Paleospinothalamic Pathway," "Some Clinical Abnormalities of Pain," "Hyperalgesia")
- Ganong's Review of Medical Physiology, 26th Ed. - Chapter 8 ("Effects of CNS Lesions," "Thalamic Pain Syndrome")
thalamic syndrome details
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive content from multiple authoritative sources. Let me compile the full, detailed response.
Thalamic Syndrome - Detailed Review
1. Nomenclature and Historical Background
Thalamic syndrome is classically called Dejerine-Roussy syndrome, named after the French neurologists Joseph Jules Dejerine and Gustave Roussy who described it in 1906. It is also called thalamic pain syndrome or central poststroke pain (CPSP) - the latter term is now preferred because not all post-stroke central pain originates purely from thalamic damage, though the thalamus remains central to the pathophysiology.
2. Anatomy - The Relevant Thalamic Nuclei
Guyton and Hall (Chapter 48 - Somatosensory Pathways) describes the thalamic ventrobasal complex as the key relay:
"The thalamus apparently has a slight ability to discriminate tactile sensation... loss of the somatosensory cortex has little effect on one's perception of pain sensation... the lower brain stem, the thalamus, and other associated basal regions of the brain are believed to play dominant roles in discrimination of these sensibilities."
The thalamus has two distinct nuclei targeted by each major ascending sensory pathway:
| Nucleus | Abbreviation | Input | Body Part |
|---|---|---|---|
| Ventral posterolateral | VPL | Spinothalamic tract, medial lemniscus | Contralateral body |
| Ventral posteromedial | VPM | Trigeminothalamic tract | Contralateral face |
Adams and Victor's (Chapter: Hemisensory Loss Caused by a Lesion of the Thalamus) states:
"Involvement of the VPL and VPM nuclei of the thalamus, usually because of a vascular lesion, causes loss or diminution of all forms of sensation on the opposite side of the body. Position sense is affected more frequently than any other sensory function."
3. Vascular Anatomy and Etiology
The classic thalamic syndrome is caused by infarction in the thalamogeniculate (posterolateral thalamic) territory, supplied by the thalamogeniculate branches of the posterior cerebral artery (PCA, P2 segment).
Localization in Clinical Neurology, 8e (Chapter: Syndromes of Thalamic Infarction) describes the four thalamic vascular territories:
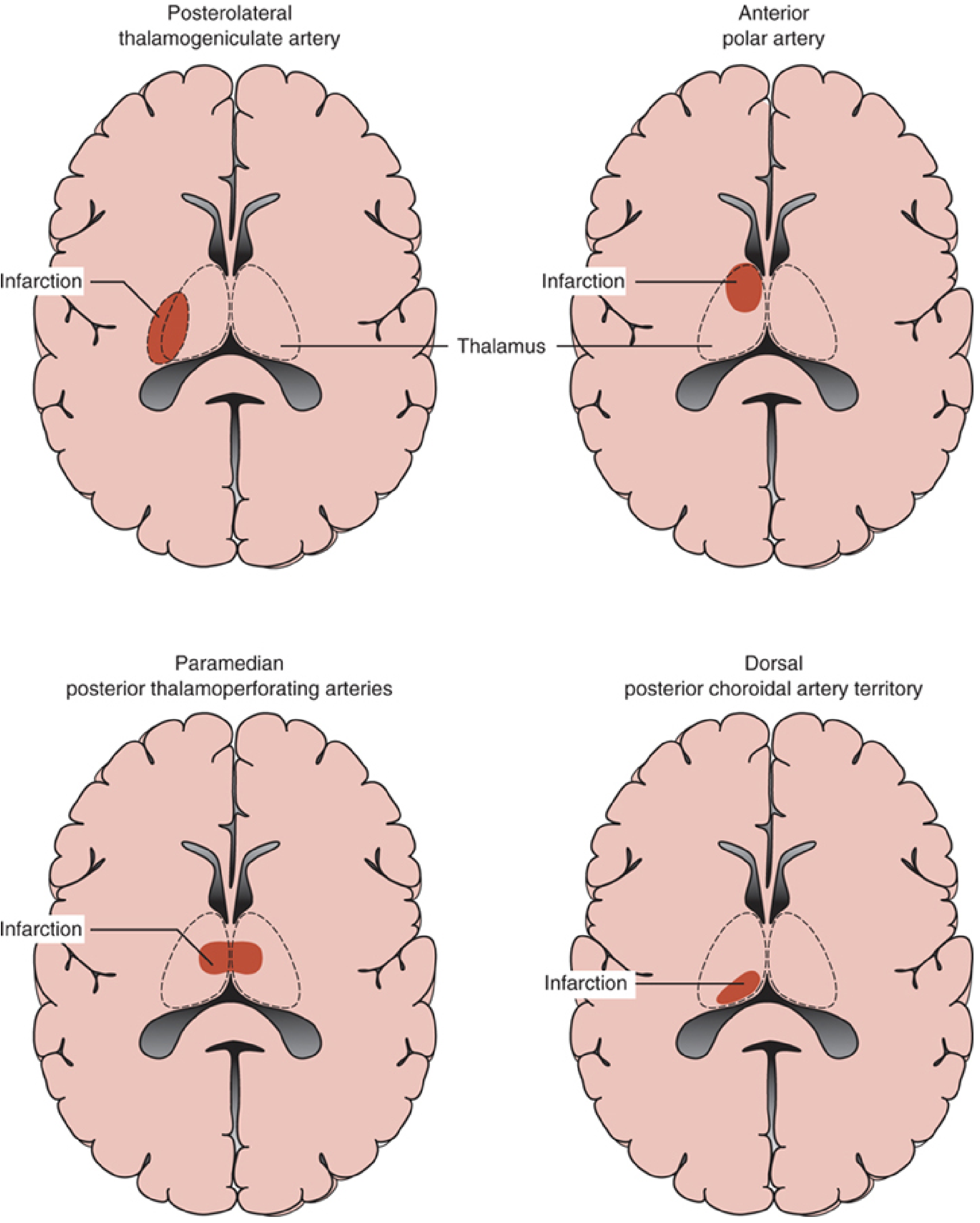
"Occlusion of thalamogeniculate branches arising from the PCA (P2 segment) causes a pure sensory stroke, a sensorimotor stroke, or the thalamic pain syndrome (Dejerine-Roussy syndrome)."
Other causes include:
- Thalamic hemorrhage - intracerebral hemorrhage involving the posterolateral thalamus (Harrison's notes patients may develop Dejerine-Roussy syndrome after thalamic hemorrhage)
- Thalamic tumors (gradual onset, unlike the apoplectic onset of stroke)
- MS plaques in thalamus/subthalamic white matter
- Hereditary hemorrhagic telangiectasia (enlarging vascular malformations)
The differential rests on rate of onset:
- Apoplectic/sudden = stroke
- Gradual = tumor
- MRI confirms the diagnosis
4. Complete Clinical Features
A. Sensory Deficits (Phase 1 - Acute)
Bradley and Daroff's Neurology (dedicated "Thalamic Syndrome" section):
"The common symptoms of thalamic syndrome include pain (thalamic pain), numbness, and hemisensory loss. The pain may be spontaneous or evoked by any form of stimulation. It often has a disagreeable and lasting quality. Patients may also complain of a distorted sense of taste. Right thalamic lesions appear to predominate.""On examination, a marked hemianesthesia is present which may be dissociated: that is, pain and temperature or light touch and vibration sense may be separately lost. Proprioceptive loss, often with astereognosis, is a common feature. A transitory hemiparesis sometimes occurs."
Localization in Clinical Neurology (Thalamogeniculate Territory) provides the full list of features:
- Hemianesthesia (occasional sparing of proprioception)
- Transient slight hemiparesis
- Hemiataxia
- Hemiataxia-hypesthesia syndrome
- Impaired automatic movements / gait (damaged "automatic pilot")
- Disequilibrium / "thalamic astasia"
- Choreoathetoid movements
- Athetoid posture ("thalamic hand") - characteristic dystonic posture of the hand on the affected side
- Pain with dysesthesias and allodynia (thalamic pain)
- Homonymous hemianopia - if medial occipital infarction occurs simultaneously
All findings are contralateral to the lesioned thalamus.
Harrison's (Signs and Symptoms: Structures Involved) adds:
"Thalamic syndrome: sensory loss (all modalities), spontaneous pain and dysesthesias, choreoathetosis, intention tremor, spasms of hand, mild hemiparesis: Posteroventral nucleus of thalamus; involvement of the adjacent subthalamus body or its afferent tracts."
B. Thalamic Pain (Phase 2 - Subacute to Chronic)
Adams and Victor's (Hemisensory Loss - Thalamus) gives the most detailed description:
"With partial recovery of sensation or with an acute but incomplete lesion, spontaneous pain, or discomfort (Dejerine-Roussy syndrome; thalamic pain syndrome), sometimes of the most distressing type, may appear on the affected side of the body. A stimulus may then have a diffuse, unpleasant, lingering quality. Thermal - especially cold - stimuli, emotional disturbance, loud sounds, and even certain types of music may aggravate the painful state. In spite of this overresponse to stimuli, the patient usually shows an elevated pain threshold, that is, a stronger stimulus than normal is necessary to produce a sensation of pain (hypalgesia with hyperpathia)."
Ganong's Review of Medical Physiology (26th Ed., Chapter 8):
"An infarct in the thalamus can lead to a loss of sensation. Thalamic pain syndrome can occur during recovery from a thalamic infarct. The syndrome is characterized by chronic pain on the side of the body contralateral to the stroke."
Harrison's (Localization of Sensory Abnormalities):
"The severe, persistent, unrelenting unilateral pain often has a burning quality and may be associated with allodynia and hyperpathia. It is persistent and responds poorly to analgesics."
Key characteristics of the pain:
- Location: Usually entire contralateral hemibody; predominantly distal in the limbs
- Quality: Burning, aching, searing, shooting, stabbing, or lancinating
- Timing: Present at rest; exacerbated by any sensory stimulation (allodynia) including touch, temperature changes (especially cold), emotional distress, loud noise, and music
- Onset: Variable - weeks to months to years after the stroke; most frequently within the first 6 months
- Distribution may shift so that it is poorly localized
5. Physiology of Thalamic Pain Generation
Guyton and Hall explains the underlying physiology in two passages:
On the role of the thalamus in pain perception:
"Complete removal of the somatic sensory areas of the cerebral cortex does not prevent pain perception. Therefore, it is likely that pain impulses entering the brain stem reticular formation, the thalamus, and other lower brain centers contribute to conscious perception of pain... the cortex plays an especially important role in interpreting pain quality, even though pain perception might be principally the function of lower centers [i.e., the thalamus]." (Chapter 49 - Role of Reticular Formation, Thalamus, and Cerebral Cortex in Appreciation of Pain)
On secondary hyperalgesia from thalamic lesions:
"Secondary hyperalgesia frequently results from lesions in the spinal cord or the thalamus." (Chapter 49 - Hyperalgesia)
Ganong ties the two together: the spinothalamic tract relays pain and temperature to the VPL nucleus; when the VPL is damaged, the pathway is disrupted acutely (producing sensory loss), but as recovery proceeds, the injured thalamic neurons become hyperexcitable - generating spontaneous aberrant discharges that are perceived as severe pain.
Bradley and Daroff (Poststroke Pain Syndrome) describes the mechanism:
"The pathogenesis of PSP is not yet known. However, it has been suggested that hyperexcitation in the damaged sensory pathways, damage to the central inhibitory pathways, or a combination of the two may be responsible for the onset of PSP."
6. Partial/Variant Forms
Localization in Clinical Neurology notes:
"Partial forms (partial geniculothalamic infarct) result from lacunar infarction restricted to one of the penetrating thalamogeniculate vessels and result in pure sensory stroke or sensorimotor stroke. Disease of such small perforating arteries often accompanies diabetes and chronic hypertension."
A specific variant - hemiataxia-hypesthesia syndrome (thalamic ataxia syndrome) - results from involvement of the lateral thalamus (VPL + VL nucleus), causing ipsilateral sensory loss and contralateral "cerebellar" ataxia due to damage to the dentatorubrothalamic tract.
Pseudothalamic syndrome: Adams and Victor note that a similar hyperpathia can occur with lesions of the parietal lobe (cortical-subcortical parietal lesions), the medial lemniscus, and even the posterior columns of the spinal cord - though these are distinct from true thalamic syndrome.
7. Laterality
Both Bradley and Daroff and Bradley's poststroke pain chapter note that right-sided thalamic lesions predominate among reported cases of thalamic pain syndrome, though the reason for this asymmetry is not fully understood.
8. Associated Nonsensory Features
Bradley and Daroff (Thalamic Pain Syndrome section) notes:
"Thalamic infarction and hemorrhage are often associated with nonsensory symptoms that can include deficits in memory, executive function, sleep cycle, and other functions."
This reflects damage to adjacent thalamic nuclei (mediodorsal, pulvinar, intralaminar) depending on the extent of infarction.
9. Investigations
- MRI brain (preferred over CT): confirms infarct or hemorrhage in posterolateral thalamus
- MRI DWI: detects acute ischemia within hours
- In delayed presentations: repeat MRI to exclude new pathology (recurrent infarction, hemorrhage, tumor)
- Somatosensory evoked potentials can help confirm thalamic dysfunction
10. Treatment
Harrison's Principles (22nd Ed.):
"Anticonvulsants (carbamazepine or gabapentin) or tricyclic antidepressants may be beneficial."
Bradley and Daroff (Poststroke Pain Syndrome):
"Tricyclic antidepressants are still a choice of treatment. Gabapentin and lamotrigine have been used to treat central PSP syndrome in open-labeled studies."Advanced interventions: "Chronic motor cortex stimulation (MCS) therapy provides pain relief for some poststroke patients. Stereotactic radiosurgery (SRS) of the pituitary and deep brain stimulation (DBS) have been used to treat PSP syndrome with some success."
The frequency is significant: 8-16% of thalamic strokes lead to chronic pain; for geniculothalamic artery strokes specifically, 13-59% develop thalamic pain syndrome.
Summary Table
| Feature | Detail |
|---|---|
| Synonyms | Dejerine-Roussy syndrome, thalamic pain syndrome, central poststroke pain |
| Most common cause | Infarction - thalamogeniculate branches of PCA |
| Nucleus involved | VPL (body), VPM (face) |
| Laterality | Lesion contralateral to symptoms; right-sided lesions predominate |
| Initial presentation | Hemisensory loss (all modalities), transient hemiparesis |
| Cardinal pain features | Contralateral, chronic, burning/searing; worse with cold, emotion, noise |
| Paradox | Elevated pain threshold (hypalgesia) yet overresponse (hyperpathia) = hyperpathia |
| Motor features | Choreoathetosis, thalamic hand (athetoid posture), hemiataxia |
| Other | Astereognosis, distorted taste, memory/sleep disturbance |
| Onset of pain | Weeks to months after stroke (within 6 months most common) |
| Treatment | Tricyclics (amitriptyline), gabapentin, lamotrigine; DBS in refractory cases |
| Responds to standard analgesics? | No - poorly responsive |
Sources:
- Guyton and Hall Textbook of Medical Physiology - Chapters 48 and 49
- Ganong's Review of Medical Physiology, 26th Ed. - Chapter 8
- Adams and Victor's Principles of Neurology, 12th Ed. - Chapter on Hemisensory Loss
- Bradley and Daroff's Neurology in Clinical Practice - Thalamic Syndrome and Poststroke Pain sections
- Harrison's Principles of Internal Medicine, 22nd Ed. - Cerebrovascular disease, Sensory localization
- Localization in Clinical Neurology, 8th Ed. - Syndromes of Thalamic Infarction
This is a shared conversation. Sign in to Orris to start your own chat.