Dupuytrens contracture
Reading File
Finding Sources
Searching PubMed
Dupuytren contracture treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive content from multiple sources. Let me compile the full answer.
Dupuytren's Contracture (Dupuytren Disease)
Definition and Pathophysiology
Dupuytren's contracture is a benign fibroproliferative disorder of the palmar fascia (aponeurosis) that leads to progressive, usually painless flexion contracture of one or more fingers. The key cellular player is the myofibroblast, which is the predominant cell type found on histologic analysis of contracted fascia. Contraction of myofibroblasts generates the early nodular findings and subsequent fibrous cords. There is a characteristic increase in the ratio of type III to type I collagen in affected tissue.
The underlying tendons and joints are not involved - the disease is confined to the fascia and overlying skin (through local invasion by fibroblastic cells, causing skin pitting).
Key anatomical points:
- Grayson's ligaments (volar) - ARE involved
- Cleland's ligaments (dorsal) - are NOT involved
- Spiral cord - associated with PIP joint contracture; the neurovascular bundle is displaced centrally and superficially, placing it at risk during surgery
Clinical Features
Bilateral hands with finger contractures:

Skin pitting and early MCP contracture (ring finger):

Progression:
- Nodular stage - firm subcutaneous nodules at the base of digits/palm; may never progress
- Cord stage - thickened fibrous bands extend into the digit, pulling finger into flexion
- Contracture stage - fixed flexion deformity at MCP and/or PIP joints
Fingers affected (in order of frequency): Ring finger > little finger > long finger
Epidemiology and Risk Factors
| Feature | Detail |
|---|---|
| Predominant population | White patients of Northern European descent |
| Sex ratio | Men affected 7x more often than women |
| Age | Rarely seen before age 40 |
| Inheritance | Autosomal dominant with variable penetrance |
| Associated conditions | Tobacco use, epilepsy (and anticonvulsant use), chronic pulmonary disease, diabetes, HIV, alcoholic cirrhosis |
| Not associated | Occupation or manual trauma (trauma not proved as a causative factor) |
Note: Occupation has NOT been associated with Dupuytren disease (Miller's Review of Orthopaedics, 9e).
Dupuytren Diathesis
A more severe, aggressive form that:
- Affects other fascial structures: soles of the feet (Ledderhose disease), popliteal fascia, knuckle pads (Garrod's pads), and penis (Peyronie's disease)
- Presents at an earlier age
- Higher risk of recurrence after treatment
Surgical Indications (Hueston Tabletop Test)
Treatment is indicated when the patient cannot place the hand flat on a tabletop (positive Hueston test), specifically:
- MCP flexion contracture >30 degrees
- Any PIP flexion contracture (even mild PIP contractures are harder to correct and tend to progress)
Treatment Options
Conservative
- Mild disease: local heat, stretching exercises, protective gloves
- Splinting does not alter disease progression
- Intralesional corticosteroid injections for painful nodules (symptomatic relief only)
Interventional / Surgical
| Option | Key Points |
|---|---|
| Open limited fasciectomy | Preferred/standard technique; best long-term correction; recurrence is still the most common complication |
| Needle aponeurotomy (percutaneous needle fasciotomy) | Smaller incisions, effective short-term, but high recurrence rate |
| Collagenase Clostridium histolyticum (CCH) injection | Enzymatic cord dissolution + corrective manipulation; as effective as open excision; gaining popularity as first-line for single-digit disease |
Collagenase outcomes (pooled data):
- Average MCP correction: up to 85%
- Average PIP correction: up to 60%
- Adverse effects: pain, swelling, bruising (temporary); skin tears more common than flexor tendon rupture
Complications of fasciectomy (in order):
- Recurrence (most common)
- Digital nerve injury
- Wound breakdown
- Complex regional pain syndrome
Recent Evidence (2023-2026)
A 2023 meta-analysis (Zhang et al., PMID 37725027) comparing collagenase vs needle fasciotomy for single-digit contractures found both are effective options with comparable results. A 2024 surgical network meta-analysis (Nann et al., PMID 37246411) reviewed all surgical approaches and confirmed that while fasciectomy provides the most durable correction, minimally invasive approaches are appropriate for many patients. A 2026 systematic review (Pistone et al., PMID 40811833) examined needle fasciotomy with and without corticosteroids - no major paradigm shift from established management.
Prognosis and Recurrence
Risk of recurrence is higher in:
- Younger patients
- Bilateral aggressive disease
- Strong family history
- Fibrotic lesions elsewhere (diathesis)
No definitive cure exists. Even after successful surgery or collagenase injection, new disease can form in other digits.
Sources: Rheumatology 2-Volume Set (Elsevier, 2022); Miller's Review of Orthopaedics 9e; PubMed meta-analyses 2023-2026
Physiotherapy management for dupuytrents contrecturey
Finding Sources
Searching PubMed
Dupuytren contracture physiotherapy rehabilitation splinting
Searching the Web
physiotherapy management Dupuytren contracture exercises splinting post-operative rehabilitation
Reading Web Page
https://emedicine.medscape.com/article/329414-treatment
Searching PubMed
Dupuytren contracture hand therapy splint outcome
Reading Article
PMID: 40047775
Reading Article
PMID: 36994455
I now have comprehensive, evidence-based content to produce a thorough answer.
Physiotherapy Management of Dupuytren's Contracture
Physiotherapy cannot reverse or cure the underlying fibrosis, but it plays a major role in three contexts: conservative management (early/mild disease), post-procedural rehabilitation (after surgery, needle fasciotomy, or collagenase injection), and function maintenance throughout the disease course.
1. Conservative / Pre-Procedural Physiotherapy
Used in early-stage disease (nodular stage, mild contracture) or when patients are not yet surgical candidates.
Physical Modalities
| Modality | Purpose | Evidence |
|---|---|---|
| Thermotherapy (heat) | Increases tissue extensibility before stretching; reduces stiffness | Empirical; commonly used |
| Therapeutic ultrasound | Deep heating of palmar fascia; may soften nodules | Low-quality evidence; may help in early nodular stage |
| Continuous ultrasound | Applied to fibrous cords to improve collagen extensibility before stretching | Adjunct use |
| TENS / Electrotherapy | Pain management for painful nodules | Symptomatic only |
Important: Splinting does not alter disease progression in conservative management. It is not recommended as a standalone conservative strategy to halt the disease. - Rheumatology 2-Volume Set (Elsevier, 2022)
Exercise Therapy (Conservative)
- Active and passive ROM exercises for all finger joints - performed several times daily
- Palmar stretching - gentle, sustained extension of the affected fingers using the opposite hand
- Tendon gliding exercises - hook fist, full fist, straight fist, table-top position to maintain differential tendon gliding
- Intrinsic stretch - abduction/adduction exercises to maintain web space mobility
- Avoid aggressive forceful stretching - it does not reverse Dupuytren cords and may cause pain
Splinting in Conservative Management
- Night extension splints (custom thermoplastic) - worn to prevent further flexion during sleep
- Goal is contracture prevention rather than reversal
- Patient education: a splint that causes pain or circulatory changes must be loosened immediately
Functional / Adaptive Strategies
- Occupational therapy component: adaptive equipment (jar openers, modified grip tools)
- Gloves during activities - protective, reduce skin irritation over nodules
- Ergonomic modifications for daily activities
2. Post-Surgical Rehabilitation
This is where physiotherapy has its greatest impact. Effective post-operative management has been stated to account for up to 50% of surgical outcomes. - Herweijer et al. (2007), Disability and Rehabilitation
Phase 1: Acute Phase (Days 0-5 post-op)
Goals: Wound protection, oedema control, pain management
- Dorsal thermoplastic static extension splint (24 hours/day until wound healing)
- Oedema management: elevation, retrograde massage, compression bandaging
- Wound care: dressing changes, monitoring for signs of infection
- ROM exercises (remove splint once every 2 hours for gentle active digit exercises)
- Avoid applied mechanical tension in the early phase - studies show this reduces complications with no loss of extension range
Phase 2: Wound Healing Phase (Week 1-3)
Goals: Restore ROM, scar management, begin function
- ROM exercises - 4 to 6 times per day (the standard NHS post-op set):
- Spread fingers apart as wide as possible, then bring together - 10 reps
- Make a fist (closing and opening fully) - 10 reps
- Passive extension stretch using the non-operated hand - 10 reps
- Table-top passive extension - palm up, gently press fingers flat, hold 2-3 seconds - 10 reps
- Dorsal passive extension - palm down on table, push fingers flat with other hand - 10 reps
- Active/passive ROM (A/PROM) exercises 8-10 times per day (protocol: once splint use transitions to nighttime only)
- Splint transition: once wound healed, move to volar thermoplastic static extension splint at night + 3 × 1.5-hour daytime periods
- Scar management: silicone gel sheets/dressings over scar to reduce hypertrophy; massage once wound fully closed
- Suture removal at 2 weeks (if non-dissolvable)
Phase 3: Remodelling Phase (Weeks 3-6)
Goals: Full ROM, grip strength, return to activities
- Progressive strengthening: putty exercises, grip strengthening
- Scar massage - cross-friction massage to improve scar mobility and pliability
- Dynamic extension splinting may be used if residual extension deficit persists (spring-loaded or serial static splinting)
- Gradually decrease splint use - rehabilitation is a progressive increase in activity with decreasing splinting
- Return to work/daily activities guided by wound healing and ROM progress
Phase 4: Late Rehabilitation (6+ weeks)
- Strengthening continues
- Fine motor and dexterity tasks
- Work-specific or sport-specific rehabilitation
- Night splinting may continue for 3-6 months post-operatively to prevent recurrence of flexion contracture during scar maturation
3. Post-Collagenase (CCH / Xiaflex) Injection Rehabilitation
Slightly different protocol from surgery since there is no wound:
- Day 2-3 post-injection/manipulation: Fabricate digit extension orthosis (hand-based)
- Active/passive ROM exercises: 8-10 times daily, performed out of the splint
- Splint schedule: Nighttime initially; if flexion lag returns, reintroduce daytime wear
- Duration: Current standard recommendation is nighttime extension orthosis for 4 months post-CCH
Key RCT Evidence on Orthosis After CCH (2025):
A prospective RCT (Dent et al., 2025 - PMID 40047775) randomised 80 patients to nighttime orthosis vs. no orthosis for 4 months post-CCH injection:
- Orthosis group had significantly lower residual contracture at 4 months (11° vs. 20°)
- Benefit was mainly in PIP joints (19° vs. 36° at 4 months) - no significant difference at MCP joints
- Recommendation: Night orthosis after CCH for PIP contractures is recommended; optional for MCP contractures
4. Splinting: Current Evidence Summary
A systematic review and meta-analysis (Karam et al., 2022 - PMID 36994455) of 4 RCTs (295 patients) comparing hand therapy alone vs. hand therapy + splinting post-fasciectomy found:
- No significant difference in total active flexion, extension, DASH scores, pain, or grip strength
- Splinting offered no added functional benefit to hand therapy alone post-fasciectomy
- However, orthotic regimes are still reasonable in patients who develop a post-op extension deficit
Practical takeaway: Splinting is most evidence-supported for PIP contractures post-CCH. After surgical fasciectomy, the evidence does not strongly support splinting as a mandatory adjunct - but it is still widely practiced for patients at risk of extension lag.
5. Physiotherapy Referral Criteria
Patients most likely to benefit from formal physiotherapy referral include:
- Recurrent Dupuytren's contracture
- Pre-op MCP or PIP contracture >40°
- Post-op extension deficit at any point
- Bilateral disease or Dupuytren diathesis
- Any wound complications (breakdown, infection, skin grafting)
- Patients with high recurrence risk (young age, strong family history)
Summary Table
| Phase | Key PT Interventions |
|---|---|
| Conservative (early disease) | Heat, ultrasound, ROM exercises, night extension splint, patient education |
| Post-op acute (day 0-5) | Dorsal splint 24h, oedema management, gentle ROM, wound care |
| Post-op healing (week 1-3) | ROM ex 4-6x/day, scar management, silicone, splint to nighttime |
| Post-op remodelling (week 3-6) | Progressive strengthening, scar massage, dynamic splinting if needed |
| Post-op late (6+ weeks) | Dexterity, return to work, night splinting up to 6 months |
| Post-CCH injection | Digit extension orthosis from day 2-3, ROM 8-10x/day, night splint 4 months (PIP essential) |
Tb spine in physiotherapy
Finding Sources
Searching PubMed
spinal tuberculosis rehabilitation physiotherapy
Searching the Web
TB spine Pott's disease physiotherapy management rehabilitation exercises spinal orthosis
Finding Sources
Reading Article
PMID: 36819453
Reading Web Page
https://www.cureus.com/articles/233168-physiotherapeutic-reh…
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have solid content from Campbell's Operative Orthopaedics, Adams & Victor's Neurology, PubMed case reports, and web sources. I have enough to write a thorough, structured answer.
TB Spine (Pott's Disease) - Physiotherapy Management
Brief Disease Overview (Context for Physiotherapy)
TB spine (Pott's disease / tuberculous spondylitis) is the most common form of skeletal TB. The infection involves the anterior vertebral body first, then spreads under the longitudinal ligaments to adjacent levels. Progressive bone destruction causes the characteristic gibbus (kyphotic) deformity and can result in cord compression and paraplegia.
MRI showing kyphotic deformity at the thoracolumbar junction with active TB disease:
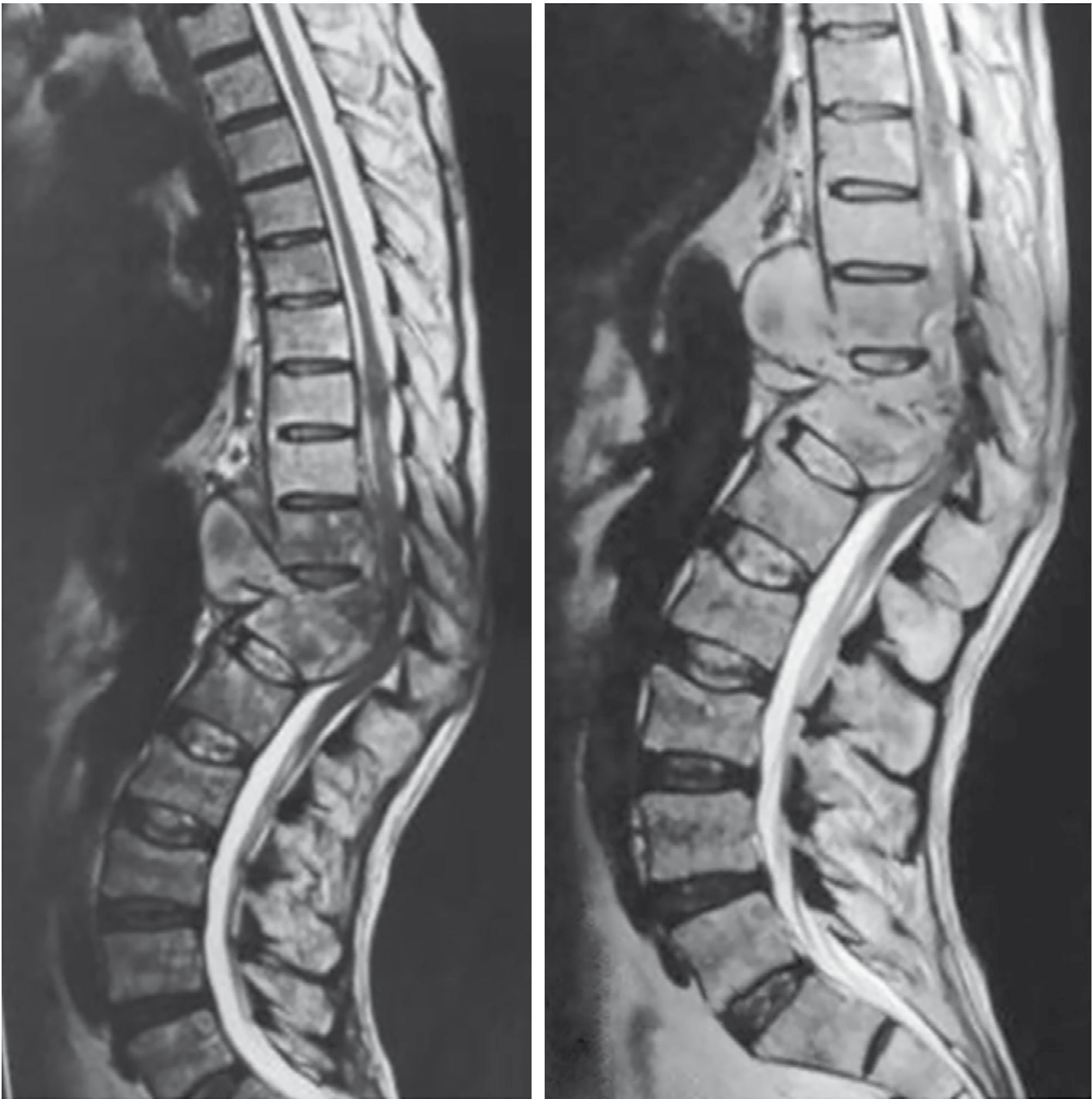
Key pathological features relevant to physiotherapy:
- Anterior vertebral destruction → spinal instability → kyphosis
- Paraspinal/psoas abscess → pain, hip flexion deformity
- Epidural pus/granulation tissue → cord compression → Pott's paraplegia (most feared complication)
- Disc involvement (in children) vs. disc sparing (adults)
- Neurological deficit in ~30% of patients in less developed countries
- Good prognostic indicators: intact motor function + normal rectal tone
Source: Campbell's Operative Orthopaedics 15e (2026)
Role of Physiotherapy in TB Spine
Physiotherapy is an essential part of the multidisciplinary team (alongside anti-TB chemotherapy and surgery when indicated). It addresses:
- Pain management
- Spinal protection and posture
- Respiratory function (especially with thoracic involvement)
- Neurological rehabilitation (paralysis/paresis)
- Functional independence and mobility
- Prevention of complications (contractures, pressure sores, DVT, pneumonia)
Phase 1: Acute Phase (Active Disease / Bed Rest Period)
Goals
- Protect the unstable spine
- Prevent immobilisation complications
- Maintain respiratory function
- Manage pain
1a. Spinal Protection
- Strict bed rest in supine (log-rolling for position changes) until spinal stability is confirmed by the treating physician
- No spinal flexion, rotation, or unsupported sitting until cleared
- Patient and carer education on proper positioning and transfers
1b. Spinal Orthosis / Brace
A custom spinal brace or TLSO (thoracolumbar sacral orthosis) is a cornerstone of conservative management:
- Indicated for thoracolumbar TB in patients without neurological deficit
- Worn during any weight-bearing or ambulation
- Purpose: limit spinal motion, prevent kyphosis progression, reduce pain, allow early mobilisation
- Evidence supports a spinal brace + chemotherapy regimen for uncomplicated thoracolumbar TB, with good outcomes over 36-48 months follow-up - Spinal brace in TB of spine, NSJ
- Cervical TB: cervical collar or halo-vest depending on instability
1c. Respiratory Physiotherapy
Thoracic TB spine frequently compromises chest expansion and respiratory mechanics:
- Diaphragmatic breathing exercises - retrain primary respiratory muscle
- Deep breathing and breath-holding techniques - maintain lung volumes
- Incentive spirometry
- Postural drainage and chest percussion if there is pulmonary TB co-involvement
- Segmental breathing to address localised lung areas
- Cough facilitation if secretion clearance is compromised (especially with thoracic kyphosis)
1d. Bed Exercises (During Bed Rest)
- Ankle pump exercises - DVT prophylaxis
- Isometric quadriceps and gluteal contractions
- Upper limb ROM and strengthening (if no cervical involvement)
- Static core activation - gentle transversus abdominis activation in supine
- Avoid any manoeuvre that loads or rotates the unstable spine
1e. Positioning and Skin Care
- Pressure area care - 2-hourly turns using log roll technique
- Foam/air mattresses to prevent pressure ulcers
- Limb positioning - splints/pillows to prevent foot drop, hip flexion contractures (especially with psoas abscess)
- Anti-foot drop splints if lower limb weakness is present
Phase 2: Subacute Phase (Disease Stabilising, Brace Prescribed)
Goals
- Gradual mobilisation with spinal protection
- Strengthen spinal and peripheral muscles
- Normalise gait and posture
- Manage neurological deficits
2a. Mobilisation Progression
- Supervised sitting → standing → walking with spinal orthosis
- Parallel bars initially for weight-bearing
- Gait training with appropriate assistive device (walking frame, elbow crutches)
- Staircase training as strength improves
2b. Core and Spinal Stabilisation Exercises
(Commenced once vertebral stability confirmed - usually after 4-6 weeks of anti-TB therapy and with radiological monitoring)
- Transversus abdominis activation in crook-lying
- Bridging exercises (gluteal + spinal extensor co-activation)
- Prone hip extensions (avoiding spinal hyperextension)
- Bird-dog exercises (supine/quadruped contralateral arm-leg raises)
- Pelvic tilts in supine
- Avoid loaded spinal flexion (sit-ups, toe touches) until fully healed
2c. Postural Correction
Kyphosis is the dominant deformity:
- Thoracic extension exercises - supported prone lying over a pillow, wall-supported thoracic extension
- Scapular retraction exercises (rhomboids, mid-trapezius) to combat the forward-rounded posture
- Chin tucks for cervical posture
- Mirror biofeedback for postural awareness
- Advise against prolonged sitting or spinal flexion activities
2d. Hip Flexor and Psoas Stretching
Psoas abscess frequently leads to a hip flexion contracture (Psoas sign / antalgic posture):
- Supine Thomas test position stretching
- Prone lying to stretch hip flexors passively
- Progress to standing hip extension stretches once allowed to weight-bear
Phase 3: Neurological Rehabilitation (Pott's Paraplegia)
This is the most complex component. Pott's paraplegia arises from cord compression and may be:
- Type A (early onset, active disease) - due to inflammatory exudate, granulation tissue; more reversible with medical/surgical treatment
- Type B (late onset) - due to bony deformity, fibrous tissue; less reversible
Neurological recovery may occur even with medical management alone, but surgical decompression accelerates it when compression is significant.
Assessment Tools Used in PT
- ASIA Impairment Scale (A-E) - for spinal cord injury classification
- Frankel grading - older scale for neurological deficit in TB spine
- Modified Barthel Index - functional independence
- Berg Balance Scale - balance assessment
- MRC grade - individual muscle strength
3a. Lower Limb Rehabilitation (Paraplegia/Paresis)
- Passive ROM exercises for all lower limb joints - started from day 1 to prevent contractures
- Facilitation techniques (PNF patterns, Bobath) to stimulate weak muscles
- Active-assisted → active → resisted exercises as recovery progresses
- Stretching of spastic muscles (hamstrings, hip flexors, plantar flexors)
- Electrical stimulation (NMES/FES) to maintain muscle bulk and facilitate weak muscles
- Hydrotherapy - buoyancy reduces spinal load; excellent medium for early mobilisation
3b. Gait Rehabilitation
- Parallel bars → walking frame → crutches → stick → unaided
- Tilt table - for gradual re-introduction to upright in complete/severe paraplegia (prevents orthostatic hypotension)
- KAFO (knee-ankle-foot orthosis) if knee extension is weak
- AFO (ankle-foot orthosis) for foot drop
- Gait re-education - heel strike, push off, weight transfer
3c. Sensory Re-education
- Texture discrimination exercises
- Weight-bearing sensory input through feet (vibration, proprioception)
- Balance training in standing with sensory perturbations (foam surface, eyes closed)
3d. Bladder and Bowel Management
- Coordinate with nursing team for bladder programme (intermittent catheterisation if needed)
- Pelvic floor muscle training where neurologically possible
- Bowel management and positioning advice
3e. Upper Limb Strengthening (for Paraplegia Patients)
- Intensive upper limb strengthening for wheelchair use and transfers
- Push-up blocks, resistance bands, shoulder press
- Transfer training (bed to wheelchair, wheelchair to toilet)
Phase 4: Late Rehabilitation and Community Reintegration
Goals
- Maximum functional independence
- Prevent deformity recurrence
- Return to activities of daily living and work/school
| Component | Intervention |
|---|---|
| Strengthening | Progressive resistive exercises, gym-based programme |
| Aerobic conditioning | Walking, cycling, swimming (as appropriate) |
| Vocational rehab | Ergonomic advice, graded return to work |
| Psychological support | TB carries stigma; address anxiety, depression |
| Patient education | Medication compliance (anti-TB drugs 6-18 months), signs of relapse |
| Home programme | Written home exercise programme, follow-up schedule |
Outcome Measures Used in TB Spine Rehabilitation
| Measure | What It Assesses |
|---|---|
| ASIA / Frankel scale | Neurological recovery |
| Modified Barthel Index | Functional independence in ADLs |
| VAS / NRS | Pain |
| Cobb angle (radiological) | Kyphosis deformity progression |
| Spirometry | Respiratory function |
| Berg Balance Scale | Balance |
| MRC grading | Muscle strength |
| 6-minute walk test | Functional ambulation endurance |
Important Precautions in TB Spine Physiotherapy
| Precaution | Reason |
|---|---|
| No spinal mobilisation/manipulation | Spinal instability, risk of cord damage |
| No spinal loading exercises until stability confirmed | Anterior bone destruction, risk of collapse |
| Infection control precautions (masks, isolation) | TB is airborne; active pulmonary TB may coexist |
| Avoid aggressive chest PT if haemoptysis present | Risk of bleeding |
| Monitor neurological status at each session | Neurological deterioration = urgent surgical review |
| Screen for orthostatic hypotension before upright | Prolonged bed rest causes autonomic dysregulation |
Evidence Base
A 2023 case report (Mandhane et al., PMID 36819453) of a conservatively managed 20-year-old with Pott's disease showed that a 6-week tailored physiotherapy programme (mobility, lower limb + core strengthening, breathing exercises, postural correction, sensory re-education) produced marked improvement in spinal mobility, pain, respiratory function, sensory function, and functional independence.
Formal high-quality RCT evidence specifically for TB spine physiotherapy is limited; management is largely based on spinal cord injury rehabilitation principles, expert consensus, and case series - reflecting the clinical complexity and variable neurological involvement of the condition.
Sources: Campbell's Operative Orthopaedics 15e (2026); Adams and Victor's Principles of Neurology 12e; PubMed (PMID 36819453); Medscape; NSJ Spinal Brace Study
This is a shared conversation. Sign in to Orris to start your own chat.