SGLT 2 inhibitors side effects
Reading File
Finding Sources
Searching PubMed
"SGLT2 inhibitors" AND "adverse effects"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of SGLT-2 inhibitor side effects, drawn from multiple pharmacology and clinical textbooks.
SGLT-2 Inhibitors - Side Effects
Drugs in class: Canagliflozin, Dapagliflozin, Empagliflozin, Ertugliflozin
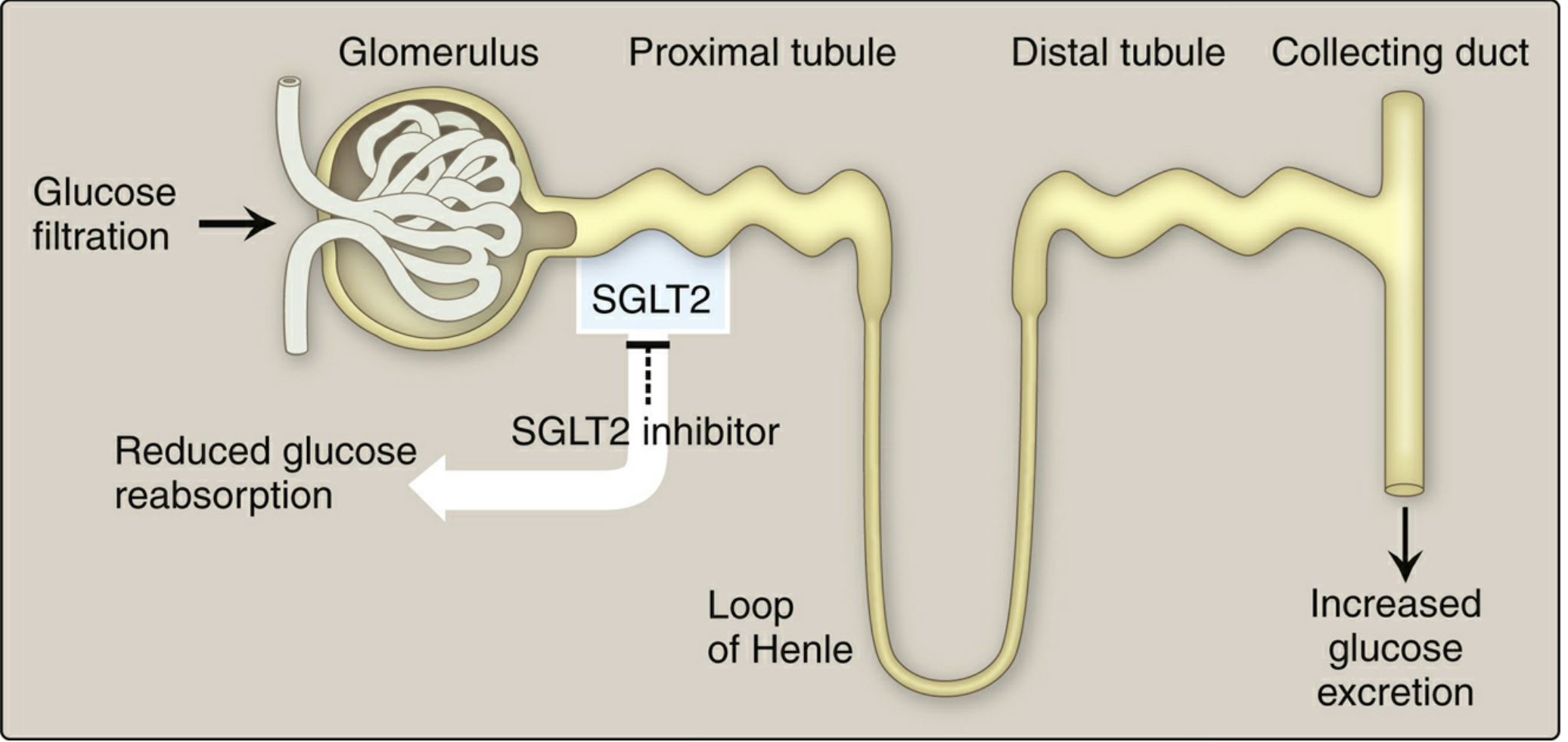
Understanding the mechanism (glucosuria + osmotic diuresis + natriuresis) explains most of the side effects below.
1. Genitourinary Infections (Most Common)
- Genital mycotic infections and urinary tract infections are the most frequent adverse effects, affecting 8-9% of patients
- Glucosuria creates a nutrient-rich environment for fungal/bacterial growth
- Cases of pyelonephritis and septicemia requiring hospitalization have been reported
- Fournier's gangrene (necrotizing fasciitis of the perineum) - rare but life-threatening; in 2018, the FDA issued a warning based on 12 documented cases
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
2. Volume Depletion & Hypotension
- Osmotic diuresis and natriuresis from glucosuria lead to intravascular volume contraction and hypotension
- Particularly relevant in elderly patients and those on diuretics
- Can cause dizziness, orthostatic hypotension, syncope
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
3. Euglycemic Diabetic Ketoacidosis (DKA)
- A distinctive and underrecognized risk - DKA occurs even with near-normal glucose levels
- Mechanism: SGLT-2 inhibition shifts metabolism toward fat oxidation and ketone production; glucosuria lowers blood glucose masking the ketotic state
- Particularly dangerous in type 1 diabetes patients (off-label use): patients may withhold insulin because glucose appears normal, precipitating severe ketoacidosis
- Also triggered by: fasting state (surgery, illness), alcohol abuse, caloric restriction
- SGLT-2 inhibitors should be held 3-4 days before surgery for this reason
- Sabiston Textbook of Surgery; Miller's Anesthesia; Goldman-Cecil Medicine; Lippincott Pharmacology
4. Renal Effects
- Can increase serum creatinine and decrease eGFR, especially in patients with pre-existing kidney impairment
- Generally not recommended when eGFR < 45 mL/min/1.73m² for glycemic control purposes
- Contraindicated when eGFR < 30 mL/min/1.73m²
- Note: Paradoxically, dapagliflozin and canagliflozin have shown renoprotective benefits in specific CKD populations (different threshold applies)
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
5. Lipid Changes
- Canagliflozin and empagliflozin cause a modest increase in LDL cholesterol (4-8%)
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
6. Bone Effects (Canagliflozin - most studied)
- Decreased bone mineral density at the lumbar spine and hip
- Pooled analysis of 8 trials (mean 68 weeks): ~30% increase in fracture risk
- Modest increase in upper limb fractures (may be related to hypotension-related falls or direct bone effects)
- Likely a class effect, not limited to canagliflozin
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
7. Lower Limb Amputations (Canagliflozin)
- One multinational trial of canagliflozin showed an increased risk of lower limb amputations, especially toes
- This finding has NOT been consistently replicated with other SGLT-2 inhibitors
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
8. Possible Cancer Risk (Dapagliflozin - historical concern)
- In early clinical trials, dapagliflozin patients had higher rates of breast cancer (9 vs 0) and bladder cancer (9 vs 1 in placebo)
- These rates exceeded age-matched diabetic reference populations
- This was a concern during initial FDA review; ongoing post-marketing surveillance continues
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
Summary Table
| Side Effect | Mechanism | Notes |
|---|---|---|
| Genital mycotic infections / UTIs | Glucosuria feeds pathogens | Most common (8-9%) |
| Fournier's gangrene | Severe perineal infection | Rare; FDA warning 2018 |
| Volume depletion / hypotension | Osmotic diuresis | Monitor in elderly |
| Euglycemic DKA | Ketone production + masked glucose | Hold pre-surgery; avoid in T1DM |
| Acute kidney injury (transient) | Volume depletion | Monitor eGFR |
| Increased LDL | Unknown | 4-8% rise |
| Bone loss / fractures | Phosphate/calcium changes | Mostly canagliflozin |
| Lower limb amputations | Unknown | Canagliflozin; not class-wide |
| Cancer (bladder/breast) | Unknown | Dapagliflozin; uncertain causation |
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Lippincott Illustrated Reviews: Pharmacology
- Goldman-Cecil Medicine, International Edition
- Fuster and Hurst's The Heart, 15th Edition
- Sabiston Textbook of Surgery
- Miller's Anesthesia, 10th Edition
How do SGLT-2 inhibitors compare to GLP-1 agonists for adverse effects?
Finding Sources
Searching PubMed
"GLP-1 receptor agonists" AND "SGLT2 inhibitors" AND "adverse effects"
Finding Sources
Finding Sources
Finding Sources
Reading Article
PMID: 39210781
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive data from both drug classes. Here is the full head-to-head comparison.
SGLT-2 Inhibitors vs. GLP-1 Agonists: Side Effect Comparison
Mechanism Review (drives all side effects)
| SGLT-2 Inhibitors | GLP-1 Agonists | |
|---|---|---|
| Core action | Block glucose reabsorption in proximal tubule → glucosuria + osmotic diuresis | Mimic GLP-1 incretin → stimulate insulin, suppress glucagon, delay gastric emptying, suppress appetite |
| Route | Oral | Subcutaneous injection (most); oral semaglutide available |
Side-by-Side Adverse Effect Profile
| Adverse Effect | SGLT-2 Inhibitors | GLP-1 Agonists |
|---|---|---|
| GI effects | Minimal | Major - nausea (11-40%), vomiting (4-13%), diarrhea (9-17%); dose-dependent |
| Genitourinary infections | Very common (8-9%) - UTIs + genital mycotic infections | Not a feature |
| Fournier's gangrene | Rare but serious (FDA 2018 warning - 12 cases) | Not reported |
| Euglycemic DKA | Yes - unique risk, especially in fasting/surgical states and T1DM | No |
| Hypoglycemia | Very low (glucose-independent mechanism) | Very low (glucose-dependent insulin release) |
| Volume depletion / hypotension | Yes - due to osmotic diuresis | Indirect only (severe vomiting/diarrhea) |
| Acute kidney injury | Can worsen eGFR, especially in CKD | Cases reported with exenatide (via dehydration from GI losses) |
| Pancreatitis | Not a class concern | Yes - all GLP-1 agonists carry this risk; counsel patients on severe abdominal pain |
| Thyroid C-cell tumors | No | Yes - rodent data for exenatide and liraglutide; contraindicated in medullary thyroid cancer history or MEN2 |
| Bone loss / fractures | Yes (canagliflozin - ~30% increase in fractures; likely class effect) | Not a concern |
| Lower limb amputations | Canagliflozin-specific signal (not class-wide) | No |
| LDL increase | Modest 4-8% (canagliflozin, empagliflozin) | No; neutral to mildly beneficial |
| Weight | Modest loss (2-5 kg) via caloric loss in urine | More pronounced loss (2-15 kg); semaglutide/tirzepatide show up to -12-19% body weight |
| Injection site reactions | None (oral) | Yes (subcutaneous formulations) - mostly mild |
| Antibody formation | None | Exenatide (~6%), lixisenatide (~70%) - may attenuate glycemic response |
| Diabetic retinopathy | Not reported | Semaglutide: paradoxical worsening seen in one trial (thought to be due to rapid glucose lowering) |
| Perioperative concern | Hold 3-4 days before surgery (euglycemic DKA + hypovolemia risk) | Hold 1 week before surgery (aspiration risk due to delayed gastric emptying) |
| Cancer risk | Bladder/breast cancer signal with dapagliflozin (early trials; uncertain) | No clear signal |
Key Differentiators
SGLT-2 inhibitors are MORE problematic for:
- Genitourinary tract (infections, Fournier's gangrene)
- Euglycemic DKA - a silent, dangerous complication
- Bone mineral density and fractures
- Volume depletion and orthostatic hypotension
- Perioperative DKA risk (must be held before surgery)
GLP-1 agonists are MORE problematic for:
- GI tolerability (nausea/vomiting is the leading reason for discontinuation)
- Pancreatitis risk
- Thyroid cancer contraindication (medullary thyroid carcinoma / MEN2)
- Perioperative aspiration risk (delayed gastric emptying - hold 1 week before surgery)
- Injection burden (most formulations are subcutaneous)
Shared Advantages (relevant context)
Both classes offer cardiovascular and renal protection beyond glucose control, and both carry a very low intrinsic risk of hypoglycemia - distinguishing them favorably from sulfonylureas and insulin. A 2024 Circulation meta-analysis (Neuen et al., PMID 39210781) confirmed that GLP-1 agonists' CV and kidney benefits are consistent whether or not the patient is already on an SGLT-2 inhibitor, with comparable safety profiles in combination use.
Practical Prescribing Takeaways
- Recurrent UTIs / yeast infections? Prefer GLP-1 agonist over SGLT-2 inhibitor
- Poor GI tolerability? Prefer SGLT-2 inhibitor over GLP-1 agonist
- Medullary thyroid Ca / MEN2? Avoid GLP-1 agonists entirely
- T1DM or insulin-deficient patients? Avoid SGLT-2 inhibitors (euglycemic DKA risk)
- Pre-surgery? Hold both - SGLT-2 inhibitors 3-4 days prior, GLP-1 agonists 1 week prior
- Need for significant weight loss? GLP-1 agonists (especially semaglutide, tirzepatide) are substantially superior
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th Edition (primary source for both classes)
- Sabiston Textbook of Surgery (perioperative guidance)
- Lippincott Illustrated Reviews: Pharmacology
- Neuen et al., Circulation 2024 - Systematic Review, PMID 39210781
This is a shared conversation. Sign in to Orris to start your own chat.