Excellent - I now have comprehensive content from Bailey & Love, Schwartz, and Robbins. I have enough to produce the complete, authoritative teaching document. Let me now compose the full MS General Surgery examination teaching note.
🎓 CARCINOMA BREAST
Complete MS General Surgery Teaching Module
Based on Bailey & Love (28th Ed.) | Schwartz (11th Ed.) | Robbins Pathology | NCCN Guidelines 2025
1. DEFINITION
Exam-oriented definition:
Carcinoma of the breast is a malignant epithelial neoplasm arising from the ductal or lobular epithelium of the breast, capable of local invasion, regional lymph node spread, and distant haematogenous metastasis.
High-yield examiner points:
- Most common cancer in women worldwide (2.3 million new cases in 2020 - Bailey & Love, 28th Ed.)
- Surpassed lung cancer as the most common cancer globally in 2020 (Robbins Pathology)
- Lifetime risk: 1 in 8 females (to age 90) in USA; 1 in 9 in Western Europe
- In India: incidence rising, now #1 female cancer overtaking cervical cancer in urban areas
- For every 2 women diagnosed in resource-poor countries, 1 dies - reflecting late presentation
Important keywords (viva favourites):
- Adenocarcinoma (epithelial origin - ducts and lobules)
- In situ vs. Invasive carcinoma
- ER/PR/HER2 receptor status - "triple negative" (TNBC)
- BRCA1/BRCA2 mutations
- Sentinel lymph node biopsy (SLNB)
- Breast conserving surgery (BCS)
- Nottingham Histological Grade (NHG)
2. CLASSIFICATION
A. By Stage of Invasion
| Category | Definition |
|---|
| In Situ (Non-invasive) | Cancer confined within ducts/lobules, basement membrane intact |
| DCIS | Ductal Carcinoma In Situ |
| LCIS | Lobular Carcinoma In Situ |
| Invasive (Infiltrating) | Basement membrane breached, invasion into stroma |
B. Histological Classification (WHO)
| Type | Frequency | Key Feature |
|---|
| Invasive Ductal Carcinoma - NST (No Special Type) | 70-80% | Most common; no special pattern |
| Invasive Lobular Carcinoma | 10-15% | Single-file "Indian file" pattern |
| Mucinous (Colloid) Carcinoma | 2-3% | Mucin pools; good prognosis |
| Tubular Carcinoma | 1-2% | Well-differentiated tubules; best prognosis |
| Medullary Carcinoma | 1-5% | Lymphocytic infiltrate; better prognosis |
| Papillary Carcinoma | <1-2% | Elderly women; good prognosis |
| Cribriform Carcinoma | Rare | Good prognosis |
| Metaplastic Carcinoma | Rare | Worst prognosis in special types |
| Inflammatory Breast Cancer | 1-5% | Dermal lymphatic invasion; worst prognosis |
| Paget's Disease of Nipple | <1-2% | Associated with underlying DCIS/IDC |
Mnemonic for special types: "MPTM - CLiP" (Mucinous, Papillary, Tubular, Medullary - Cribriform, Lobular, inflammatory, Paget's)
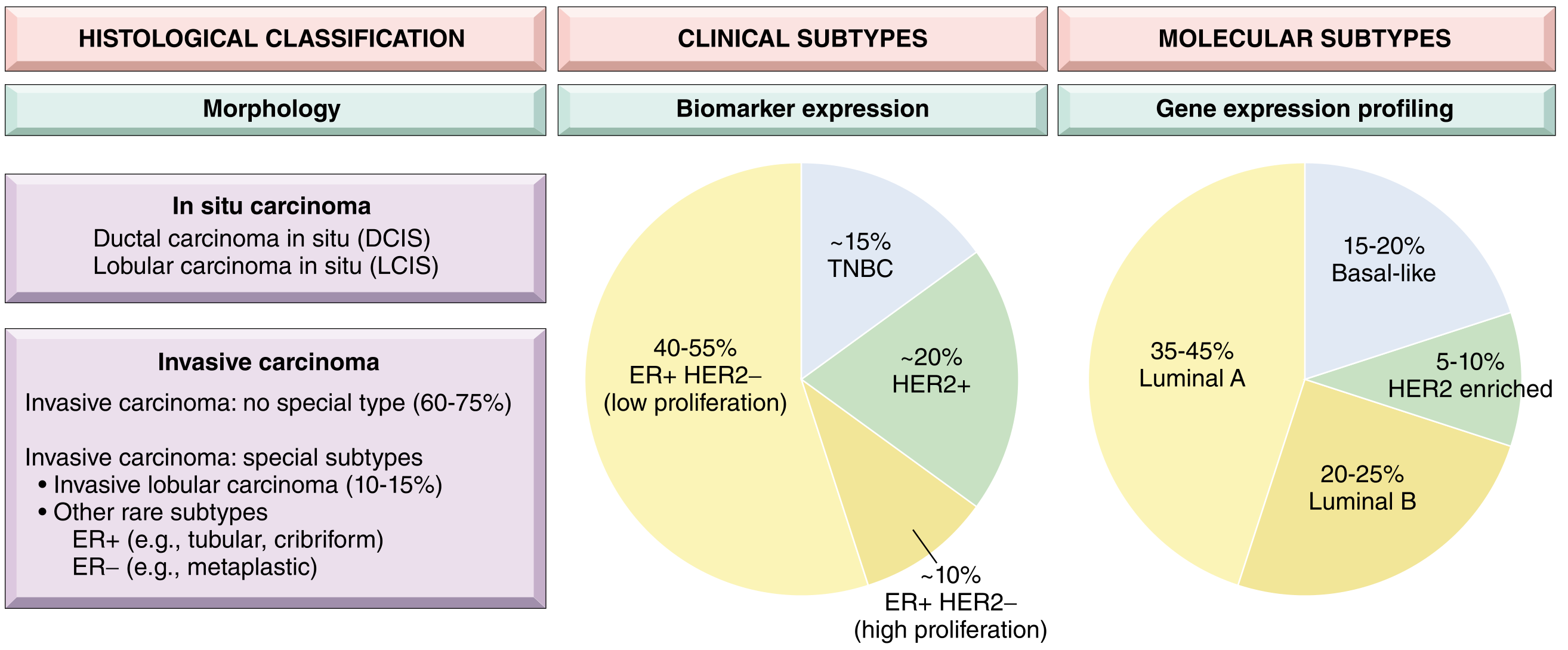
C. Molecular (Intrinsic Subtype) Classification - Robbins / Schwartz
| Subtype | ER | PR | HER2 | Key Points |
|---|
| Luminal A | + | + | - | Best prognosis; hormone-sensitive |
| Luminal B | + | +/- | +/- | Intermediate prognosis |
| HER2-enriched | - | - | + | Trastuzumab target |
| Basal-like (TNBC) | - | - | - | Worst prognosis; BRCA1-associated; chemo-sensitive |
| Normal-like | + | + | - | Similar to Luminal A |
| Claudin-low | - | - | - | Stem cell features |
D. DCIS Classification (Schwartz Table 17-9)
| Subtype | Nuclear Grade | Necrosis | DCIS Grade |
|---|
| Comedo | High | Extensive | High |
| Intermediate | Intermediate | Focal or absent | Intermediate |
| Non-comedo (solid, cribriform, papillary) | Low | Absent | Low |
Examiner trap: Comedo DCIS = high-grade, worst prognosis among DCIS types. Calcifications on mammography are due to necrosis in comedo DCIS.
E. TNM Staging (AJCC 8th Edition)
Primary Tumor (T)
| T | Description |
|---|
| T0 | No evidence of primary tumor |
| Tis | DCIS, LCIS, Paget's (no tumor) |
| T1 | ≤20 mm |
| T1mi | ≤1 mm (microinvasion) |
| T1a | >1 mm, ≤5 mm |
| T1b | >5 mm, ≤10 mm |
| T1c | >10 mm, ≤20 mm |
| T2 | >20 mm, ≤50 mm |
| T3 | >50 mm |
| T4 | Any size with chest wall/skin involvement |
| T4a | Chest wall invasion |
| T4b | Skin edema/ulceration/satellite nodules |
| T4c | T4a + T4b |
| T4d | Inflammatory breast cancer |
Regional Lymph Nodes (N) - Pathological
| N | Description |
|---|
| N0 | No nodes |
| N1 | 1-3 axillary nodes; or internal mammary (clinical) |
| N2 | 4-9 axillary nodes; or internal mammary (clinical, no axillary) |
| N3 | ≥10 axillary; or infraclavicular; or supraclavicular |
Overall Stage Grouping
| Stage | TNM | 5-Year Survival |
|---|
| 0 | Tis N0 M0 | ~99% |
| IA | T1 N0 M0 | ~99% |
| IB | T0-1 N1mi M0 | ~99% |
| IIA | T0-1N1/T2N0 | ~93% |
| IIB | T2N1/T3N0 | ~75% |
| IIIA | T0-2N2/T3N1-2 | ~66% |
| IIIB | T4 any N | ~41% |
| IIIC | Any T N3 | ~41% |
| IV | Any T, Any N, M1 | ~27% |
3. SURGICAL ANATOMY
A. Breast Anatomy
Position: Modified cone structure overlying pectoralis major (2nd-6th rib, sternum to mid-axillary line)
Quadrants:
UOQ (Upper Outer) | UIQ (Upper Inner)
─────────────────────────────────────
LOQ (Lower Outer) | LIQ (Lower Inner)
Central/Subareolar
- UOQ = most common site for carcinoma (50%) - examiner's favourite
- Axillary tail of Spence = extension into axilla through foramen in deep fascia
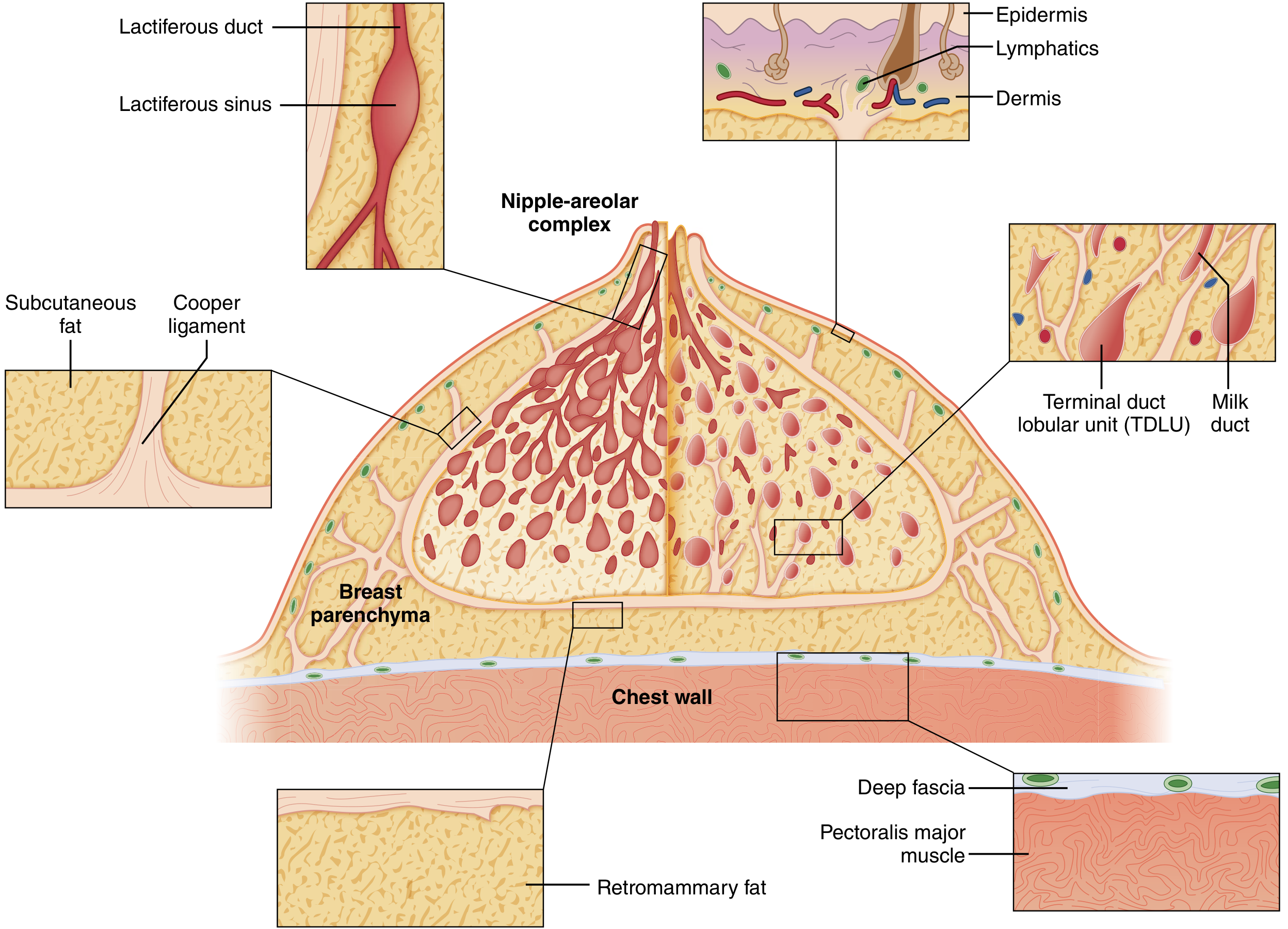
B. Layers from Skin to Chest Wall
- Skin
- Subcutaneous fat
- Cooper's ligaments (suspensory ligaments)
- Breast parenchyma (15-20 lobes radiating from nipple)
- Retromammary bursa (plane of surgical dissection)
- Deep pectoral fascia
- Pectoralis major
Clinical pearl: Cooper's ligaments attach breast parenchyma to overlying skin - when invaded by carcinoma = skin dimpling/peau d'orange appearance
C. Blood Supply
| Artery | Source | Territory |
|---|
| Internal mammary (thoracic) perforators | Internal thoracic artery (branches of subclavian) | Medial 60% of breast |
| Lateral thoracic artery | 2nd part of axillary artery | Lateral/upper breast |
| Thoracoacromial artery | 2nd part of axillary artery | Upper breast |
| Anterior intercostal perforators | Intercostal arteries | Deep breast |
| Subscapular artery | 3rd part of axillary artery | Lateral |
Key examiner fact: Internal mammary artery = dominant supply = reason medial quadrant tumors have worse prognosis (internal mammary node drainage)
D. Venous Drainage
- Mirrors arterial supply
- Internal mammary veins → brachiocephalic vein → SVC
- Intercostal veins → vertebral venous plexus of Batson → haematogenous spread to spine (most common bone metastasis site)
- Axillary vein tributaries
Batson's plexus - valveless communication between pelvic/breast veins and vertebral venous plexus = explains vertebral and CNS metastases
E. Lymphatic Drainage - CRITICAL FOR EXAM
Level Classification of Axillary Nodes (Berg's Levels):
| Level | Location | Relation to Pectoralis Minor |
|---|
| Level I | Lateral to PM | 75% of nodes - most common sentinel node level |
| Level II | Behind PM (interpectoral/Rotter's nodes) | |
| Level III | Medial to PM (apical/infraclavicular) | |
Level I (lateral) → Level II (behind) → Level III (apical/Halsted's)
→ Subclavian vein → Thoracic duct/Right lymphatic duct
Other drainage pathways:
- Internal mammary nodes (parasternal) - especially medial quadrant tumors
- Supraclavicular nodes - N3 disease (Stage IIIC)
- Interpectoral (Rotter's) nodes - between pectoralis major and minor
- Cross-drainage to contralateral axilla possible
Examiner trap: "Which nodes are sampled in SLNB?" - Level I axillary nodes and internal mammary nodes (in selected cases)
F. Nerve Supply - Critical for Operative Anatomy
| Nerve | Origin | Function | Injury Consequence |
|---|
| Long thoracic nerve (of Bell) | C5, C6, C7 | Serratus anterior | Winged scapula |
| Thoracodorsal nerve | Posterior cord | Latissimus dorsi | Weak arm extension/adduction |
| Medial pectoral nerve | Medial cord | Pec major & minor | Pectoralis atrophy |
| Lateral pectoral nerve | Lateral cord | Pec major | Pectoralis atrophy |
| Intercostobrachial nerve (T2) | T2 lateral cutaneous | Upper inner arm sensation | Numbness/dysesthesia inner arm |
MOST FEARED COMPLICATION in axillary dissection = Injury to Long Thoracic Nerve = Winged Scapula
4. ETIOLOGY AND RISK FACTORS
A. Risk Factor Table (Bailey & Love - Table 58.3)
Non-Modifiable Risk Factors
| Factor | Relative Risk | Comments |
|---|
| Female sex | Male: Female = 1:100 | |
| Increasing age | Major risk | Peaks 50-70 years |
| BRCA1 mutation (17q21) | 50-85% lifetime risk | Also 40% ovarian CA risk; mostly TNBC |
| BRCA2 mutation (13q12.3) | 50-60% lifetime risk | Also prostate, colon, pancreatic CA |
| Family history (1st degree) | RR = 2.1 | Mother/sister/daughter |
| Family history (2nd degree) | RR = 1.5 | |
| Previous breast cancer | RR = 5 | |
| DCIS/LCIS | RR = 8-10 (DCIS); 6-9 (LCIS) | LCIS = risk marker, not precursor |
| Atypical ductal hyperplasia | RR = 4-5 | |
| Early menarche (<12 years) | RR = 1.3 | Increased estrogen exposure |
| Late menopause (>55 years) | RR = 1.5 | |
| Dense breast tissue | RR = 2-6 | |
| Li-Fraumeni syndrome (TP53) | Very high | |
| Cowden syndrome (PTEN) | 25-50% lifetime | |
Modifiable Risk Factors (Bailey & Love)
| Factor | Relative Risk | Notes |
|---|
| Nulliparity / Late first pregnancy (>35 yrs) | RR = 1.3-2.0 | |
| HRT >10 years | RR = 1.2 | Combined estrogen-progestogen |
| Obesity (BMI >30) - postmenopausal | RR = 1.29 | Adipose tissue aromatase |
| Alcohol | RR up to 1.46 (>4 drinks/day) | |
| Radiation exposure (chest irradiation) | RR = 6 | Mantle field for Hodgkin lymphoma |
| Smoking | RR = 1.14 (>25 cigs/day) | |
| Physical inactivity | RR = 1.2-1.4 | |
Protective Factors
- Breastfeeding >12 months (protective)
- Early first pregnancy (<20 years)
- Physical activity
- Bilateral oophorectomy before age 40
- Tamoxifen/Raloxifene (chemoprevention)
B. Genetic Mutations Summary
| Gene | Location | Associated Cancers | Risk |
|---|
| BRCA1 | 17q21 | Breast (TNBC), Ovarian | 50-85% |
| BRCA2 | 13q12.3 | Breast, Ovary, Prostate, Pancreas | 50-60% |
| TP53 | 17p13.1 | Li-Fraumeni syndrome | Very high |
| PTEN | 10q23 | Cowden syndrome | 25-50% |
| CDH1 | 16q22 | Lobular carcinoma, Gastric | ~40% |
| STK11 | 19p13.3 | Peutz-Jeghers | ~50% |
| PALB2 | 16p12.2 | Breast | ~35% |
| CHEK2 | 22q12.1 | Moderate risk | ~25% |
5. PATHOPHYSIOLOGY
Step-by-Step Disease Progression
NORMAL BREAST EPITHELIUM
↓
Normal → Hyperplasia (without atypia)
↓
Atypical Ductal Hyperplasia (ADH) / Atypical Lobular Hyperplasia (ALH)
↓ [RR = 4-5×]
DCIS (Ductal) / LCIS (Lobular) — IN SITU PHASE
↓ [DCIS → 30-50% risk; LCIS = 1-2% per year]
INVASIVE CARCINOMA (Basement membrane breached)
↓
Local invasion into breast stroma
↓
Lymphatic permeation → Regional lymph nodes
- Level I → Level II → Level III axillary
- Internal mammary nodes
- Supraclavicular nodes (N3)
↓
Haematogenous spread (Batson's plexus, axillary/internal mammary veins)
↓
DISTANT METASTASES
(Bone > Lung > Liver > Brain > Adrenals)
Key Molecular Events
- Estrogen receptor (ER) activation drives proliferation in luminal tumors
- HER2 amplification (chromosome 17q) → tyrosine kinase overexpression → uncontrolled proliferation
- Loss of BRCA1/2 → failure of DNA double-strand break repair
- Epithelial-Mesenchymal Transition (EMT) → invasion and metastasis
- Angiogenesis (VEGF upregulation) → vascular invasion
Skin Changes - Pathophysiological Basis
| Sign | Mechanism |
|---|
| Skin dimpling | Cooper's ligament tethering/invasion |
| Peau d'orange (orange peel skin) | Dermal lymphatic invasion → lymphedema of skin |
| Nipple retraction | Invasion/fibrosis of major subareolar ducts |
| Skin ulceration | Tumor breaching dermis |
| Paget's disease | Intraepidermal spread of carcinoma cells along nipple epidermis |
6. CLINICAL FEATURES
History
Cardinal presenting complaint:
- Painless lump in the breast (most common, ~70%)
- Pain (10-15% have pain as dominant symptom)
- Nipple discharge (blood-stained = red flag)
- Nipple retraction/inversion
- Skin changes (dimpling, peau d'orange, ulceration)
- Axillary lump
- Arm swelling (lymphedema - late)
- Systemic symptoms (weight loss, bone pain, cough, jaundice)
History checklist for viva/long case:
- Duration and progression of lump
- Change in size (especially with menstrual cycle)
- Nipple discharge: character, laterality, number of ducts
- Pain: cyclical vs. non-cyclical
- Family history (BRCA)
- Menstrual history: menarche, menopause, OCP/HRT use
- Obstetric history: pregnancies, breastfeeding
- Previous biopsies / radiation history
- Systemic symptoms (metastasis screen)
Signs
Local Signs
- Lump characteristics: Hard, irregular, ill-defined, fixed
- Skin dimpling / tethering
- Peau d'orange (pitting edema of skin)
- Nipple retraction / deviation
- Nipple discharge (blood-stained)
- Skin ulceration (advanced disease)
- Satellite nodules (T4b)
- Chest wall fixity (T4a)
Regional Signs
- Axillary lymphadenopathy (ipsilateral) - hard, matted, fixed
- Supraclavicular lymphadenopathy (N3)
- Arm edema (axillary node block)
Systemic Signs (Metastatic Disease)
- Bone pain/tenderness (vertebrae, pelvis, ribs, skull)
- Hepatomegaly
- Pleural effusion (dyspnea)
- Neurological signs (brain metastasis)
- Jaundice (liver metastasis)
Red Flag Signs
- ⚠️ Hard, irregular lump > 2 cm
- ⚠️ Skin dimpling or peau d'orange
- ⚠️ Blood-stained nipple discharge (unilateral, single duct)
- ⚠️ Recent nipple inversion (previously normal nipple)
- ⚠️ Hard, fixed axillary nodes
- ⚠️ Supraclavicular nodes
- ⚠️ Paget's disease of nipple
- ⚠️ Inflammatory breast cancer (erythema, warmth, skin induration)
- ⚠️ Bone pain + breast lump
- ⚠️ Arm edema ipsilateral to breast lump
Differential Diagnosis of Breast Lump
| Condition | Age | Character | Other Features |
|---|
| Carcinoma | >40 (post-menopausal) | Hard, irregular, ill-defined, fixed | Skin changes, nodes |
| Fibroadenoma | 15-35 (young) | Firm, smooth, mobile, well-defined ("breast mouse") | No skin changes |
| Fibrocystic disease | 30-45 (premenopausal) | Tender, ill-defined, nodular, varies with cycle | Bilateral |
| Breast cyst | 35-55 | Smooth, fluctuant, well-defined | Transilluminates |
| Fat necrosis | Any | Hard, irregular, may have skin dimpling | History of trauma |
| Phyllodes tumor | 35-45 | Smooth, lobulated, rapidly growing | Dilated veins |
| Breast abscess | Post-partum | Tender, fluctuant, red | Fever, lactating |
| Duct ectasia | 40-60 | Periareolar, pasty/multicolored discharge | Nipple retraction |
Examiner trap - Fat necrosis vs. Carcinoma: Fat necrosis can mimic carcinoma with skin dimpling and irregular hard lump. Always biopsy.
7. CLINICAL EXAMINATION
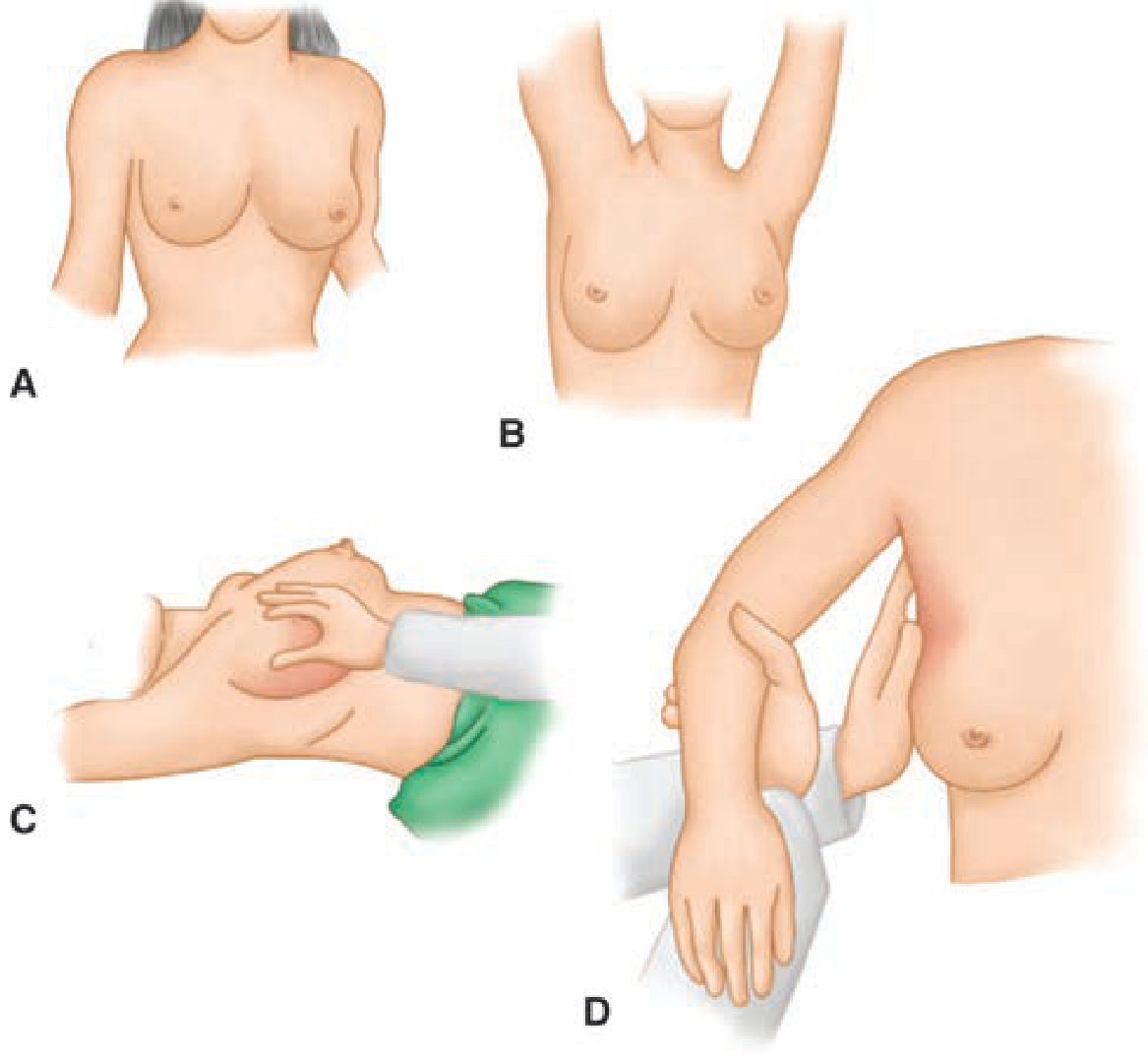
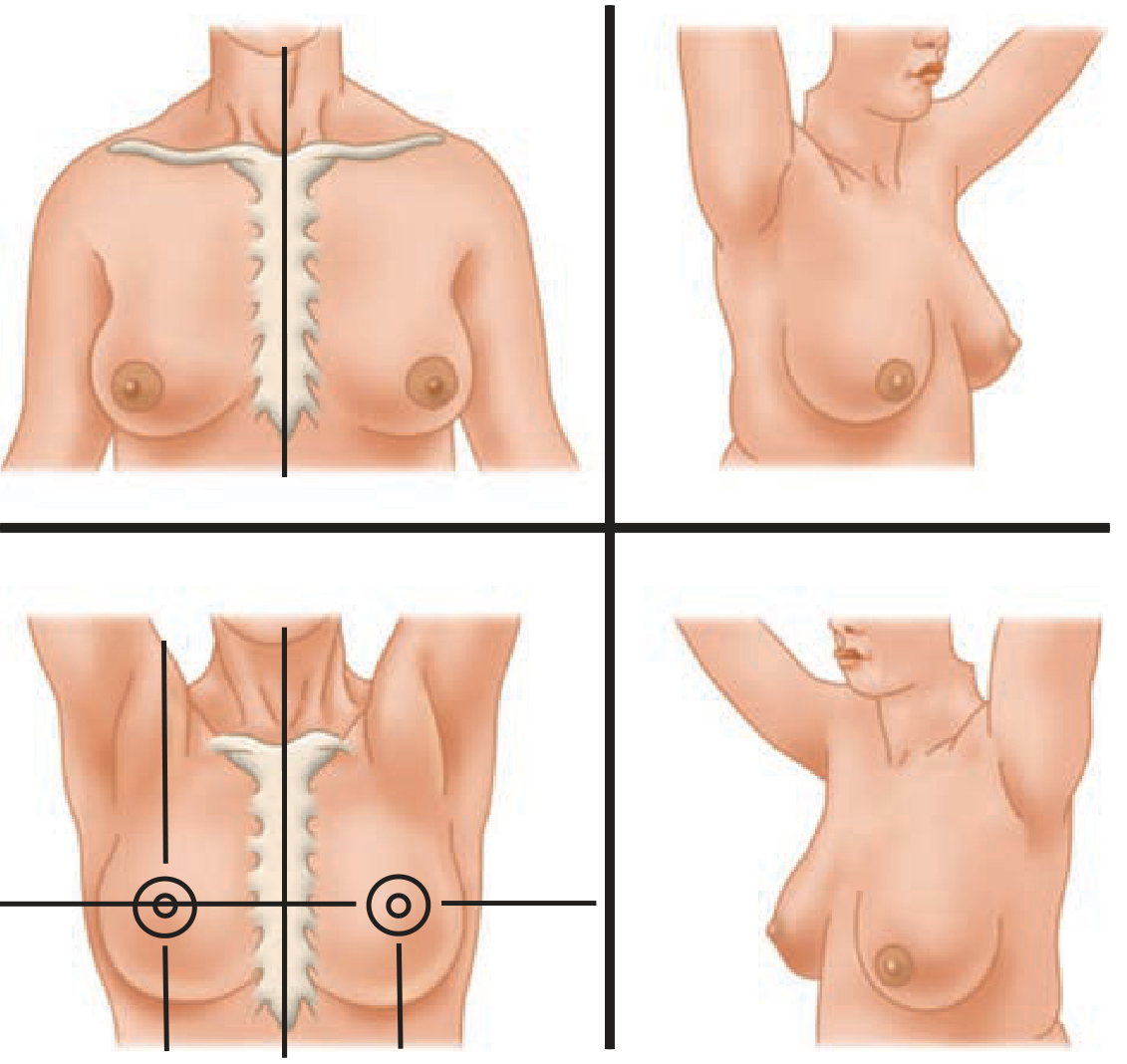
Inspection (Patient sitting, arms at side → raised above head → hands on hips)
Observe for:
- Asymmetry of breasts (size, shape, level)
- Skin changes: dimpling, peau d'orange, erythema, ulceration, satellite nodules
- Nipple: retraction, deviation, Paget's changes, discharge
- Dilated veins over breast
- Edema of arm (look from behind)
- Lymphedema of arm
Positions for inspection:
- Sitting, arms relaxed
- Arms raised above head (tethering/dimpling becomes visible)
- Hands pressed on hips (pectoralis contracted - fixity to chest wall)
- Leaning forward (ptosis, skin tethering)
Palpation
Technique:
- Examine with flat of fingers, not fingertips
- Systematic: 4 quadrants + subareolar + axillary tail
- Palpate axilla with arm relaxed (patient's arm resting on examiner's forearm)
- Always examine both breasts and both axillae
- Examine supraclavicular fossae
Lump characteristics to describe:
- Site (quadrant, distance from nipple)
- Size (measure in cm)
- Shape (regular/irregular)
- Surface (smooth/nodular/irregular)
- Margin (well/ill-defined)
- Consistency (soft/firm/hard/stony hard)
- Fixity (to skin? to deep fascia? to chest wall?)
- Tenderness
- Transillumination (for cyst - will not transilluminate in carcinoma)
- Pulsatility
Testing fixity to skin: Pinch skin over lump - if fixed, skin moves with lump
Testing fixity to chest wall: Move lump with pectoralis relaxed, then contracted (hands on hips)
Axillary Examination
Groups of axillary nodes (CREAM):
- Central nodes (Level I - most commonly involved)
- Apical (Level III - infraclavicular)
- Pectoral (anterior - Level I)
- Subscapular (posterior - Level I)
- Lateral (Level I - along axillary vein)
Examination of axilla:
- Examiner's right hand examines patient's right axilla
- Patient's arm supported by examiner's left hand
- Feel along: chest wall, anterior wall, posterior wall, medial wall, axillary vein
Node characteristics:
- Number, size, consistency, fixity, matting
Special Tests
| Test | Technique | Positive Finding |
|---|
| Skin tethering test | Lift skin over lump | Cannot lift = skin involved |
| Pectoralis test | Move lump with pec relaxed vs. contracted | Reduced mobility on contraction = deep fixity |
| Nipple discharge | Gentle pressure along breast ducts toward nipple | Blood-stained = red flag |
| Axillary vein compression | Palpate along axillary vein | Firm, fixed nodes = malignant |
Clinical Pearls
- "Breast mouse" = mobile fibroadenoma (young woman)
- "Peau d'orange" is NOT pathognomonic for carcinoma - also in mastitis, but with fever
- A lump that disappears after aspiration = cyst; if solid residue remains = suspicious
- Always examine the contralateral breast (10% bilateral carcinoma)
- In Paget's disease: eczematous change that STARTS AT NIPPLE (unlike dermatitis which starts at areola)
- Triple assessment = Clinical + Imaging + Pathology (cytology/biopsy)
8. INVESTIGATIONS
Triple Assessment (The Gold Standard Diagnostic Framework)
TRIPLE ASSESSMENT
│
┌─────────┼─────────┐
│ │ │
Clinical Imaging Pathology
Exam (USG/ (FNAC/
Mammo) Core Biopsy)
Each component graded 1-5:
- 1 = Normal
- 2 = Benign
- 3 = Uncertain/probably benign
- 4 = Suspicious for malignancy
- 5 = Malignant
Triple Assessment 5/5/5 = Malignant; 1/1/1 = Benign
Routine Investigations
| Investigation | Purpose |
|---|
| CBC, renal/liver function | Pre-operative assessment |
| Serum calcium | Bone metastasis screen |
| Alkaline phosphatase (ALP) | Bone/liver metastasis |
| Chest X-ray | Lung metastasis, pleural effusion |
| Blood group and cross-match | Pre-operative |
| ECG, echocardiogram | If anthracycline chemotherapy planned |
Specific/Imaging Investigations
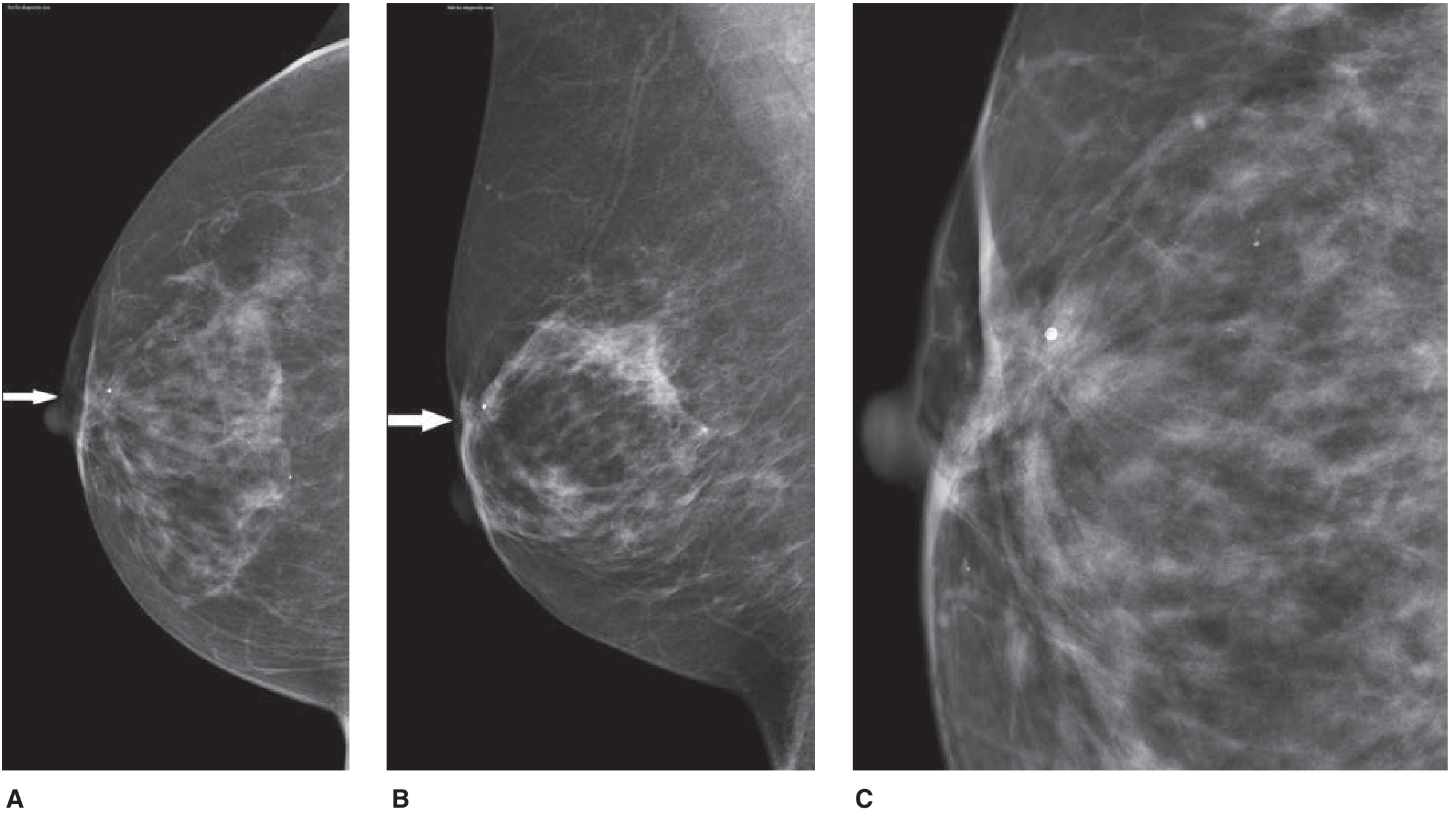
Mammography
- Best initial imaging in women >35 years
- Screening: 2-view mammography (craniocaudal + mediolateral oblique)
- Features of malignancy on mammography:
- Irregular/spiculated mass (stellate lesion)
- Microcalcifications (especially clustered, pleomorphic - pathognomonic of comedo DCIS)
- Architectural distortion
- Asymmetric density
- Skin/nipple retraction
- ACR BI-RADS (Breast Imaging Reporting and Data System):
| BI-RADS | Category | Management |
|---|
| 0 | Incomplete | Additional imaging |
| 1 | Negative | Routine screening |
| 2 | Benign | Routine screening |
| 3 | Probably benign | Short-term follow-up (6 months) |
| 4 | Suspicious | Tissue sampling |
| 5 | Highly suggestive of malignancy | Tissue sampling |
| 6 | Known malignancy | Treatment planning |
Ultrasound (USG) Breast
- Best initial imaging in women <35 years and in pregnancy
- Differentiates solid vs. cystic lesions
- Features of malignancy: irregular margins, posterior acoustic shadowing, spiculated
- Guides FNAC/core needle biopsy
- Axillary USG for lymph node assessment
MRI Breast
- Not routine; specific indications:
- BRCA mutation carriers (annual screening from age 25)
- Occult primary breast cancer (axillary nodes, no mammographic lesion)
- Implant integrity
- Surgical planning for BCS (assess extent/multifocality)
- Monitoring neoadjuvant chemotherapy response
- Dense breasts where mammography limited
PET-CT
- Staging of advanced/metastatic disease
- Monitoring treatment response
- Detecting recurrence
Bone Scan
- Suspected bone metastasis
- Routine for Stage III-IV disease
Pathological Investigations
FNAC (Fine Needle Aspiration Cytology)
- Quick, cheap, office procedure
- Graded C1-C5:
- C1 = Inadequate
- C2 = Benign
- C3 = Atypia (probably benign)
- C4 = Suspicious (probably malignant)
- C5 = Malignant
- Limitation: Does not distinguish invasive from in situ carcinoma
Core Needle Biopsy (Tru-Cut Biopsy) - GOLD STANDARD
- 14G needle; US-guided
- Gives histology, receptor status (ER/PR/HER2), grade
- Advantages over FNAC: Tissue architecture preserved; can grade; receptor status
- Preferred over FNAC in current practice
Excision Biopsy
- For impalpable lesions (wire-guided/vacuum-assisted)
- For lesion not amenable to core biopsy
IHC (Immunohistochemistry) on Biopsy Specimen
| Marker | Significance |
|---|
| ER (Estrogen Receptor) | + = hormone therapy benefit |
| PR (Progesterone Receptor) | + = hormone therapy benefit |
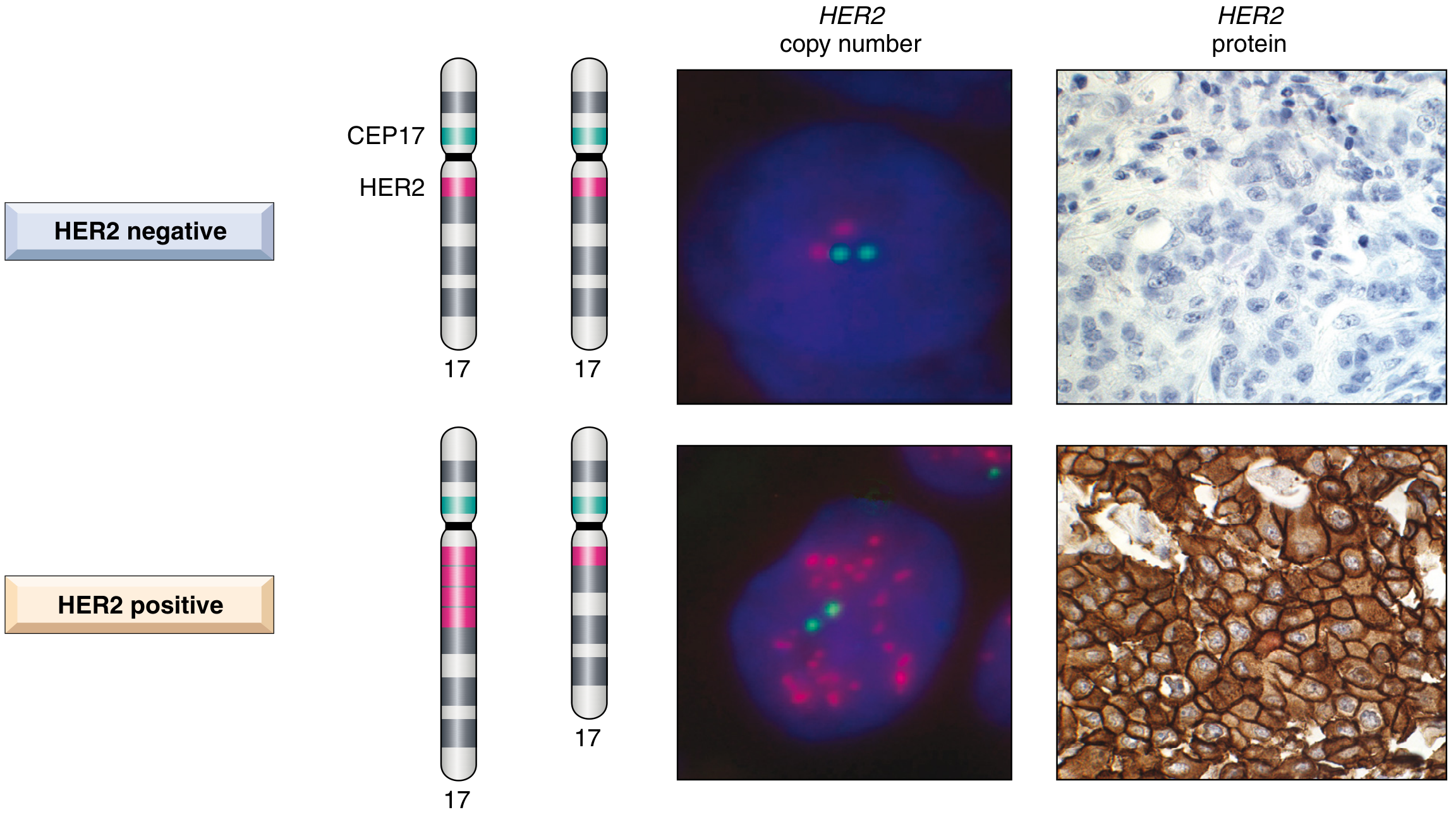
| HER2 | 3+ (IHC) or FISH amplified = trastuzumab target |
| Ki-67 | Proliferation index; >20% = high grade |
| p53 | BRCA1-associated tumors |
HER2 Testing Algorithm:
IHC 3+ → HER2 POSITIVE (trastuzumab eligible)
IHC 2+ → FISH (fluorescence in situ hybridization) → amplified or not amplified
IHC 0 or 1+ → HER2 NEGATIVE
Nottingham Histological Grade (NHG / Elston-Ellis Grade)
| Feature | Score 1 | Score 2 | Score 3 |
|---|
| Tubule formation | >75% | 10-75% | <10% |
| Nuclear pleomorphism | Mild | Moderate | Marked |
| Mitotic count | Low | Intermediate | High |
- Total score 3-5 = Grade 1 (well differentiated, best prognosis)
- Total score 6-7 = Grade 2 (moderately differentiated)
- Total score 8-9 = Grade 3 (poorly differentiated, worst prognosis)
Examiner pearl: Nottingham Grade = Elston-Ellis modification of Bloom-Richardson grading
Staging Workup
| Stage | Investigations |
|---|
| Stage I-IIA | Mammogram, USG, core biopsy, CXR, LFTs, ALP |
| Stage IIB-III | Add: bone scan, CT chest/abdomen/pelvis |
| Stage IV (metastatic) | Add: PET-CT, MRI brain if neurological symptoms |
9. DIAGNOSTIC ALGORITHM
BREAST LUMP
│
▼
TRIPLE ASSESSMENT
│
┌────┼────┐
│ │ │
Clin Img Path
│
Age <35 → USG first
Age >35 → Mammogram first
│
Benign features → Reassure + Follow-up
Indeterminate → Core needle biopsy
Malignant features → Core biopsy + IHC
│
▼
CONFIRMED MALIGNANCY
│
▼
STAGING WORKUP
(CXR, LFTs, ALP, Bone scan if Stage II-III, CT/PET-CT if Stage III-IV)
│
▼
MULTIDISCIPLINARY TEAM (MDT) MEETING
│
┌────┴────┐
│ │
Early (I-III) Metastatic (IV)
│ │
Surgery + Palliative systemic
Adjuvant Rx therapy + best
supportive care
10. DIFFERENTIAL DIAGNOSIS
Comparison Table
| Feature | Carcinoma | Fibroadenoma | Fibrocystic | Cyst | Fat Necrosis |
|---|
| Age | >40 | 15-35 | 35-50 | 35-50 | Any |
| Pain | Painless | Painless | Cyclical pain | +/- | +/- |
| Lump | Hard, irregular | Firm, smooth | Ill-defined, nodular | Smooth, fluctuant | Hard, irregular |
| Mobility | Fixed | Very mobile | Slightly mobile | Mobile | May be fixed |
| Skin changes | + (late) | - | - | - | + (may dimple) |
| Nipple discharge | Blood-stained | - | Multicolored | - | - |
| Axillary nodes | Hard, fixed | - | - | - | - |
| Mammogram | Spiculated mass/calc | Well-defined oval | Dense + cysts | Round opacity | Lucent/oil cyst |
| USG | Irregular, shadow | Oval, homogeneous | Mixed | Anechoic, thin wall | Variable |
| Biopsy | Malignant | Benign fibroepithelial | Benign | Benign | Benign |
11. MANAGEMENT
A. Multidisciplinary Team (MDT) Approach
Surgical Oncologist + Medical Oncologist + Radiation Oncologist
+ Radiologist + Pathologist + Plastic Surgeon + Psychologist
= MDT MEETING (Gold Standard for treatment planning)
B. Initial Resuscitation / Emergency Management
- Inflammatory breast cancer emergency: initiate systemic chemotherapy urgently
- Pathological fracture: orthopaedic stabilization + radiotherapy
- Spinal cord compression (oncological emergency):
- High-dose dexamethasone immediately
- Urgent MRI spine
- Radiotherapy ± surgical decompression
- Hypercalcaemia of malignancy:
- IV hydration + bisphosphonates (zoledronic acid 4 mg IV)
C. Management Algorithm by Stage
STAGE 0 (DCIS)
│
BCS + Whole Breast RT (WBRT)
OR Mastectomy ± SLNB
+ Tamoxifen (ER+ DCIS, 5 years)
STAGE I - IIA (Early Breast Cancer)
│
Surgery: BCS + SLNB OR Mastectomy + SLNB
│
Adjuvant:
ER+/HER2-: Hormonal therapy ± Chemotherapy (OncotypeDx guided)
HER2+: Trastuzumab + Chemotherapy
TNBC: Chemotherapy (AC-T or TC regimen)
RT: After BCS (mandatory); After mastectomy (if T3/N2-3)
STAGE IIB - IIIA (Locally Advanced, Resectable)
│
Neoadjuvant Chemotherapy (NACT) first
│
Reassess → Surgery (BCS if good response OR Mastectomy)
│
Adjuvant: RT + Hormonal/HER2 targeted therapy
STAGE IIIB-IIIC (Locally Advanced, Unresectable)
│
NACT → Surgery (usually modified radical mastectomy)
│
Adjuvant RT + Systemic therapy
STAGE IV (Metastatic)
│
Palliative intent:
ER+/HER2-: Endocrine therapy (CDK4/6 inhibitors ± aromatase inhibitor)
HER2+: Trastuzumab + pertuzumab + chemotherapy
TNBC: Chemotherapy ± immunotherapy (pembrolizumab if PD-L1+)
+ Bisphosphonates for bone metastases
+ Palliative RT for pain/cord compression
D. Surgical Management
1. Breast Conserving Surgery (BCS) / Wide Local Excision / Lumpectomy
Indications:
- Single, unifocal tumor
- T1-T2 lesions (up to 4-5 cm relative to breast size)
- Patient preference
- No contraindications to radiotherapy
Contraindications to BCS:
- Multifocal/multicentric disease
- Previous breast/chest wall irradiation
- Pregnancy (relative if 3rd trimester)
- Inflammatory breast cancer (T4d)
- Diffuse malignant-appearing microcalcifications
- Inability to achieve clear margins after re-excision
- Connective tissue disease (scleroderma, active lupus)
- Large tumor relative to breast size (oncoplastic techniques may help)
Principles:
- Margin of excision must be clear (≥2 mm per NICE; no tumor on ink per SSO/ASTRO 2014)
- Must always be followed by whole breast radiotherapy (WBRT)
- Oncological equivalence to mastectomy in appropriately selected patients (Milan trials, NSABP B-06)
2. Mastectomy Types
| Procedure | What is Removed | Preserved |
|---|
| Simple (Total) Mastectomy | Entire breast + skin + nipple | Pectoralis major, axillary nodes |
| Modified Radical Mastectomy (MRM) | Entire breast + axillary LN (levels I-III) | Pectoralis major (preserves chest wall) |
| Radical Mastectomy (Halsted) | Breast + pec major + pec minor + axillary LN | Nothing |
| Extended Radical Mastectomy | + Internal mammary nodes | Historically used |
| Patey's Operation | Breast + axillary LN levels I-III + pec minor | Pectoralis major |
| Auchincloss-Madden | Breast + axillary LN levels I-II | Both pectorals |
| Skin-sparing Mastectomy | Breast tissue only, preserves skin envelope | Skin for reconstruction |
| Nipple-sparing Mastectomy | Breast tissue only | Skin + nipple-areola complex |
| Prophylactic Mastectomy | Prophylaxis in BRCA carriers | Reconstruction |
Examiner favourite: "What is the difference between Patey's and Halsted's?" - Patey = pec major preserved; Halsted = pec major removed
MRM is the standard mastectomy for operable breast cancer in India/developing countries
3. Axillary Management
SLNB (Sentinel Lymph Node Biopsy):
- Indications: Clinically/imaging node-negative (cN0)
- Technique: Patent Blue dye ± Tc-99m labelled nanocolloid (radioisotope)
- Sentinel node = first node to receive lymphatic drainage
- If SLN negative → no further axillary surgery
- If SLN positive → ALND or axillary radiotherapy (per Z0011 trial criteria)
ALND (Axillary Lymph Node Dissection) - Levels I-III:
- Indications: Clinically positive axillary nodes (cN1+), positive SLNB (>2 positive SLN, or not meeting Z0011 criteria)
- Standard yield: ≥10 lymph nodes
- Complications: Lymphedema (20-30%), seroma, nerve injury
ACOSOG Z0011 Trial (Key viva point):
- SLNB-positive patients with 1-2 positive SLN, T1-T2 tumors, BCS + WBRT can OMIT ALND without compromise in survival
E. Systemic Therapy
Neoadjuvant Chemotherapy (NACT)
Indications:
- Locally advanced breast cancer (Stage IIIA-IIIC)
- HER2+ or TNBC in early stage (to downstage for BCS)
- Inflammatory breast cancer
- Large tumor relative to breast size (to facilitate BCS)
Regimens (anthracycline + taxane based):
- AC → T: Doxorubicin + Cyclophosphamide → Paclitaxel/Docetaxel
- FEC → D: 5-FU + Epirubicin + Cyclophosphamide → Docetaxel
- For HER2+: Add pertuzumab + trastuzumab to chemotherapy backbone
pCR (Pathological Complete Response):
- No residual invasive cancer in breast and nodes after NACT
- Best predictor of long-term survival especially in HER2+ and TNBC
Adjuvant Chemotherapy
- ER-/HER2- (TNBC): AC-T regimen; add pembrolizumab (KEYNOTE-522)
- HER2+: Trastuzumab for 1 year; T-DM1 if residual disease after NACT (KATHERINE trial)
- Capecitabine for TNBC with residual disease post-NACT (CREATE-X trial)
Hormonal Therapy
| Agent | Class | Indication |
|---|
| Tamoxifen | SERM | Premenopausal ER+ (5-10 years) |
| Anastrozole / Letrozole / Exemestane | Aromatase inhibitor (AI) | Postmenopausal ER+ (5-10 years) |
| Ovarian suppression (GnRH agonist) | Goserelin/Leuprolide | Premenopausal high-risk |
| Fulvestrant | SERD | Metastatic ER+ |
| CDK4/6 inhibitors (Palbociclib, Ribociclib, Abemaciclib) | Cell cycle inhibitor | Metastatic ER+/HER2- (first line) |
| Elacestrant | Oral SERD | ESR1-mutated metastatic ER+ |
HER2-Targeted Therapy
- Trastuzumab (Herceptin): Anti-HER2 monoclonal antibody (1 year adjuvant)
- Pertuzumab: Anti-HER2 (different epitope); neoadjuvant/metastatic
- T-DM1 (ado-trastuzumab emtansine): Antibody-drug conjugate; residual disease after NACT
- T-DXd (trastuzumab deruxtecan): Second-line metastatic HER2+; also HER2-low tumors
- Lapatinib + Tucatinib: Small molecule TKIs; brain metastases
PARP Inhibitors (BRCA-mutated)
- Olaparib / Talazoparib: Metastatic BRCA-mutated HER2-negative; also adjuvant (OlympiA trial)
F. Radiotherapy
| Scenario | RT Indication | Technique |
|---|
| After BCS | Mandatory - reduces local recurrence | Whole breast RT (WBRT) |
| After mastectomy (Post-mastectomy RT, PMRT) | T3-4, N2-3, close/positive margins | Chest wall + nodal RT |
| Hypofractionation | Equivalent to conventional; preferred | 40 Gy/15# (FAST-Forward trial) |
| APBI (Accelerated Partial Breast Irradiation) | T1, ER+, node-negative, age >40, no BRCA | ASTRO 2024 guidelines |
| Axillary RT | Alternative to ALND in 1-3 positive SLN | AMAROS trial |
| Palliative RT | Bone metastasis, CNS, skin ulceration | Varies |
12. SURGICAL PROCEDURES
A. Modified Radical Mastectomy (MRM) - PATEY'S OPERATION
Indications
- Operable breast cancer not suitable for BCS
- Patient preference
- Locally advanced cancer after NACT
Contraindications
- Stage IV (palliative mastectomy only for toilet/fungating tumor)
- Medically unfit
Patient Positioning
- Supine, arm abducted 90° on arm board
- Shoulder slightly elevated with sandbag
- Arm draped separately for mobility
Anesthesia
Incision (Stewart/Greenough transverse ellipse)
Medial Lateral
←─────────────────────────→
ELLIPTICAL INCISION
(encircling nipple-areola complex)
Upper and lower skin flaps raised
- Transverse ellipse 3 cm above and below breast
- Includes nipple-areola complex
- Extends from parasternal to mid-axillary line
Operative Steps (Stepwise)
Step 1: Incision
- Mark ellipse encompassing nipple; 3 cm clearance from tumor
Step 2: Skin flap elevation
- Raise upper flap: to clavicle and below pectoralis major
- Raise lower flap: to inframammary fold
- Flap thickness 5-8 mm (preserve subdermal plexus; avoid skin necrosis)
Step 3: Breast clearance from pectoralis major
- Elevate breast off pectoralis major fascia (leaving it on specimen)
- From superomedial to inferolateral
- Pectoralis major muscle preserved (distinguishes from Halsted)
Step 4: Division of pectoralis minor (Patey's - pec minor excised)
- Divide pec minor at coracoid process insertion
- This exposes Level III (apical) nodes
- In Auchincloss-Madden: pec minor retracted, not divided
Step 5: Axillary clearance
- Clear from medial to lateral
- Identify and preserve:
- Long thoracic nerve of Bell (on serratus anterior - medial wall of axilla)
- Thoracodorsal nerve (on subscapularis - posterior wall)
- Thoracodorsal vessels (may be ligated if nodal clearance demands)
- Axillary vein (superior limit of dissection)
- Remove Level I, II, III nodes en bloc with specimen
Step 6: Hemostasis and drain placement
- Two suction drains (axilla and inferior flap)
- Wound closure in layers (subcutaneous + skin)
Critical Anatomy and Danger Zones
| Structure | Location | Consequence of Injury |
|---|
| Long thoracic nerve | Medial wall of axilla on serratus anterior | Winged scapula |
| Thoracodorsal nerve | Posterior wall on subscapularis | Weak arm adduction/internal rotation |
| Axillary vein | Upper limit of axillary dissection | Major hemorrhage |
| Brachial plexus | Superior to axillary vein | Arm paralysis |
| Intercostobrachial nerve | T2, crosses axilla horizontally | Numbness upper inner arm |
Complications
Early:
- Hemorrhage / hematoma
- Seroma (most common - 30-40%)
- Skin flap necrosis
- Infection
- Pneumothorax (rare)
Late:
- Lymphedema (20-30% after ALND)
- Shoulder stiffness/dysfunction
- Winged scapula (long thoracic nerve injury)
- Numbness inner arm (intercostobrachial nerve)
- Local recurrence
- Phantom breast sensation
B. Sentinel Lymph Node Biopsy (SLNB)
Technique
- Peri-tumoral/periareolar injection of:
- Patent Blue dye (methylene blue) - intraoperative
- Tc-99m nanocolloid - preoperative (lymphoscintigraphy)
- Wait 5-10 minutes for dye to migrate
- Hand-held gamma probe guides identification of hot node
- Identify blue-stained lymphatic channel → follow to blue/hot node
- Excise sentinel node(s) → intraoperative frozen section or imprint cytology
- If negative: no further axillary surgery
- If positive: ALND OR axillary RT (per ACOSOG Z0011 criteria)
Identification Rates and False Negative Rates
- Identification rate: 95-98%
- False negative rate: 5-10%
C. Breast Conserving Surgery (Wide Local Excision)
Steps
- Mark lump + 1-2 cm margins on skin
- Elliptical incision along Langer's lines (cosmetic)
- Excise specimen with adequate 3D margins (orientate specimen with clips/sutures)
- Send specimen for margin assessment (intraoperative frozen section OR post-op)
- If margins positive → re-excision OR conversion to mastectomy
- Haemostasis + closure
- Specimen mammogram (if impalpable lesion with wire localization)
13. COMPLICATIONS
A. Post-Mastectomy / Post-ALND Complications
EARLY COMPLICATIONS LATE COMPLICATIONS
───────────────────── ─────────────────────
Hemorrhage/Hematoma Lymphedema (most common late)
Seroma (most common early) Shoulder stiffness
Wound infection Winged scapula
Skin flap necrosis Numbness inner arm
Pneumothorax Local recurrence
Deep vein thrombosis Tumor-en-cuirasse
Pulmonary embolism Stewart-Treves syndrome
(lymphangiosarcoma in chronic lymphedema)
B. Lymphedema Management
- Severity: measured by limb circumference difference
- Prevention: avoid IV lines/blood pressure cuff on affected arm
- Treatment:
- Complete Decongestive Therapy (CDT)
- Compression garments
- Manual lymphatic drainage (MLD)
- Exercises
- Surgery (Charles procedure, liposuction) - rarely
C. Seroma Management
- Most common early complication (30-40%)
- Drain with needle aspiration
- Compression bandage
- Drain removal only when <30 mL/day output
D. Stewart-Treves Syndrome
- Lymphangiosarcoma developing in chronic post-mastectomy lymphedema
- Bluish-purple skin lesions on arm
- Very poor prognosis
- Radical excision ± radiotherapy
14. VIVA DISCUSSION
Rapid-Fire Viva: 40+ Examiner Questions with Model Answers
Q1. What is the most common site of carcinoma in the breast?
A: Upper outer quadrant (UOQ) - 50% of cases, because it contains the greatest amount of breast tissue (axillary tail of Spence).
Q2. What is the most common type of breast carcinoma?
A: Invasive Ductal Carcinoma - Not Otherwise Specified (IDC-NST), accounting for 70-80%.
Q3. What is the gold standard for diagnosing breast cancer?
A: Triple Assessment (Clinical + Imaging + Pathology), with Core Needle Biopsy as the gold standard tissue diagnosis.
Q4. What is the difference between DCIS and LCIS?
A: DCIS = true precursor lesion; basement membrane intact; 30-50% risk of ipsilateral breast cancer; requires treatment. LCIS = risk marker, NOT precursor; bilateral risk 1-2% per year; can be observed in most cases (Bailey & Love).
Q5. What are the contraindications to BCS?
A: Multifocal/multicentric disease, previous irradiation, diffuse malignant microcalcifications, inability to achieve clear margins, inflammatory breast cancer, connective tissue disease, patient preference.
Q6. What nerve injury causes winged scapula?
A: Injury to the Long Thoracic Nerve of Bell (C5, C6, C7), which supplies serratus anterior.
Q7. What is the difference between Halsted's and Patey's mastectomy?
A: Halsted = removes pectoralis major + minor + breast + axillary LN. Patey = preserves pectoralis major but removes pectoralis minor. Auchincloss-Madden = preserves BOTH pectoralis muscles.
Q8. What are Berg's levels of axillary lymph nodes?
A: Level I = lateral to pectoralis minor; Level II = behind pec minor (Rotter's nodes); Level III = medial to pec minor (apical/infraclavicular nodes).
Q9. What is sentinel lymph node biopsy? What dye is used?
A: Identification of the first draining lymph node from the primary tumor. Uses Patent Blue dye ± Tc-99m labelled nanocolloid. A hand-held gamma probe identifies the radioactive "hot" node.
Q10. What are the components of the Nottingham Histological Grade?
A: (1) Tubule formation, (2) Nuclear pleomorphism, (3) Mitotic count. Each scored 1-3. Total 3-5 = Grade 1; 6-7 = Grade 2; 8-9 = Grade 3.
Q11. What is peau d'orange? What is the mechanism?
A: Orange-peel appearance of breast skin due to dermal lymphatic blockade causing skin edema. Hair follicles tethered to skin appear as dimples against edematous background.
Q12. What is Paget's disease of the nipple?
A: Eczematous change of the nipple and areola due to intraepidermal spread of large pale Paget's cells from an underlying DCIS or invasive carcinoma. Starts at nipple (unlike contact dermatitis which starts at areola).
Q13. What is inflammatory breast cancer? What is the TNM stage?
A: Diffuse erythema, edema, and warmth of ≥1/3 of breast skin due to dermal lymphatic invasion by carcinoma. Classified as T4d. Stage IIIB minimum. Treated with NACT first; mastectomy NOT the initial treatment.
Q14. What are the BRCA genes? What cancers are associated?
A: BRCA1 (17q21) - breast (TNBC mostly), ovarian, fallopian tube. BRCA2 (13q12.3) - breast, ovarian, prostate, pancreatic, gastric, gallbladder. BRCA1 carriers: 50-85% lifetime breast cancer risk.
Q15. What are the indications for neoadjuvant chemotherapy in breast cancer?
A: Locally advanced/unresectable disease, inflammatory breast cancer, HER2+ or TNBC (to downstage for BCS), large tumor relative to breast size.
Q16. What is the significance of hormone receptor status?
A: ER+/PR+ tumors respond to hormonal therapy (tamoxifen/aromatase inhibitors). HER2+ responds to trastuzumab. TNBC (ER-/PR-/HER2-) has worst prognosis; treated with chemotherapy ± immunotherapy.
Q17. What is the ACOSOG Z0011 trial?
A: RCT showing that in cN0 patients with T1-T2 breast cancer, 1-2 positive SLN, undergoing BCS + WBRT, omission of ALND does NOT compromise survival. Axillary RT can replace ALND.
Q18. What is BI-RADS classification?
A: ACR Breast Imaging Reporting and Data System: 0=incomplete, 1=negative, 2=benign, 3=probably benign, 4=suspicious (biopsy needed), 5=highly suspicious (biopsy needed), 6=known malignancy.
Q19. What is the most common site of distant metastasis in breast cancer?
A: Bone (spine, pelvis, ribs, skull) - via Batson's paravertebral venous plexus. Then lung, liver, brain.
Q20. What is the most common early complication of axillary dissection?
A: Seroma (30-40%). Most common late complication = Lymphedema (20-30%).
Q21. What is Stewart-Treves syndrome?
A: Lymphangiosarcoma developing in chronic post-mastectomy lymphedema. Bluish-purple papules/plaques on affected arm. Very poor prognosis (5-year survival <5%).
Q22. What is the van Nuys Prognostic Index (VPSI) for DCIS?
A: A scoring system for DCIS using: tumor size, margin width, nuclear grade + necrosis, and patient age. Score guides treatment (BCS alone vs. BCS + RT vs. mastectomy).
Q23. What is the difference between breast conserving surgery outcomes vs. mastectomy?
A: Survival is EQUIVALENT (NSABP B-06, Milan I trials). Local recurrence rates are higher with BCS (10-15% vs. 5-8% with mastectomy) but corrected by adjuvant radiotherapy. BCS = mastectomy in appropriately selected patients.
Q24. What is Batson's plexus?
A: Valveless paravertebral venous plexus communicating between thoracic veins (including internal mammary/intercostal) and vertebral veins. Explains haematogenous spread to vertebral column and CNS without going through lungs/liver first.
Q25. What is a "toilet mastectomy"?
A: Mastectomy performed for palliation in locally advanced/fungating tumor to improve hygiene, pain relief, and quality of life, without curative intent (Stage IV disease).
Q26. What is male breast cancer?
A: Rare (<1% of all breast cancers). Mean age 60-70 years. BRCA2 mutation more common than BRCA1 in males. Usually IDC. Mostly ER+. Treatment: MRM (BCS rarely done). Tamoxifen for ER+ disease.
Q27. Enumerate the layers of the axillary wall.
A: Anterior wall = pectoralis major + minor; Posterior wall = subscapularis, teres major, latissimus dorsi; Medial wall = serratus anterior + ribs; Lateral wall = coracobrachialis + short head of biceps + humerus; Apex = between 1st rib, clavicle, superior scapula; Base = axillary fascia + skin.
Q28. What is mammographic screening protocol?
A: UK: 2-view mammogram (CC + MLO) every 3 years, age 50-70. USA: Annual from age 40 (ACOG). India: No national program; opportunistic screening in high-risk.
Q29. What is OncotypeDx?
A: A 21-gene recurrence score assay on tumor tissue. Recurrence score 0-25 = low risk (hormone therapy alone); 26-100 = high risk (add chemotherapy). Used in ER+/HER2-/node-negative/low-node-positive early breast cancer.
Q30. What is trastuzumab? What is its mechanism?
A: Monoclonal antibody targeting HER2 extracellular domain. Blocks HER2 signaling, induces ADCC (antibody-dependent cellular cytotoxicity). Used in HER2+ breast cancer (adjuvant 1 year; neoadjuvant; metastatic). Side effect: cardiotoxicity (cardiomyopathy).
Q31. What are the criteria for BRCA testing?
A: Family history of ≥2 first-degree relatives with breast/ovarian cancer, breast cancer <40 years, bilateral breast cancer, male breast cancer, TNBC <50 years, Ashkenazi Jewish ancestry, known BRCA in family.
Q32. What is "port-wine stain" appearance in breast?
A: Peau d'orange skin in inflammatory breast cancer gives a dusky red, pitted appearance.
Q33. Name the arteries supplying the nipple-areola complex.
A: Branches of internal mammary artery (medial mammary branches), lateral thoracic artery, and thoracoacromial artery.
Q34. What is a Rotter's node? What is its significance?
A: Interpectoral lymph nodes lying between pectoralis major and minor (Level II). Missed in Level I ALND; included in Level III dissection. Named after J. Rotter.
Q35. What radiological signs suggest malignancy in mammogram?
A: Spiculated/irregular mass with ill-defined margins, clustered pleomorphic microcalcifications, architectural distortion, skin thickening, nipple retraction, asymmetric density.
Q36. What are the criteria for nipple-sparing mastectomy?
A: No tumor involvement of nipple/areola clinically or radiologically, tumor >2 cm from nipple, no Paget's disease, no extensive DCIS near nipple. Intraoperative frozen section of subareolar tissue.
Q37. What is the role of bisphosphonates in breast cancer?
A: Reduce skeletal-related events (fractures, hypercalcemia) in bone metastases. Zoledronic acid 4 mg IV every 4 weeks. In adjuvant setting: zoledronic acid reduces bone metastasis and improves survival in postmenopausal ER+ patients (ABCSG-12, AZURE trials).
Q38. What is the clinical relevance of tumor-node-metastasis in breast cancer prognosis?
A: Node status is the single most important prognostic factor. 5-year survival: node-negative = ~80%; 1-3 nodes = ~60%; ≥4 nodes = ~30-40% (Schwartz).
Q39. What operation is used for Paget's disease of nipple with underlying invasive cancer?
A: Mastectomy (usually MRM). If localized DCIS only: cone excision of nipple-areola complex + WBRT may be possible.
Q40. What are Haagensen's criteria of inoperability?
A: (1) Extensive skin edema >1/3 breast; (2) Satellite skin nodules; (3) Inflammatory breast cancer; (4) Supraclavicular nodes; (5) Arm edema; (6) Chest wall fixity (parasternal); (7) Distant metastases.
15. CASE DISCUSSION
How to Present a Breast Cancer Long Case in the Exam Hall
Case Introduction (1 minute)
"I have examined Mrs. [Name], a [age]-year-old [occupation] female, who presented with a painless lump in the [right/left] breast of [duration] duration. The lump has been [progressive/static]. She also complains of [skin changes/nipple discharge/axillary swelling]."
History Highlights to Cover
- Chief complaint + duration + progression
- Associated symptoms: pain, nipple changes, discharge, skin changes
- Systemic symptoms: weight loss, bone pain, cough, jaundice
- Menstrual/obstetric history (menarche, LMP, pregnancies, breastfeeding, OCP/HRT)
- Family history (breast/ovarian cancer)
- Past history (previous biopsies, radiation)
Examination Findings to Present
- General: BMI, pallor, jaundice, lymphadenopathy
- Breast: Inspect + Palpate - all characteristics of the lump
- Axilla: Palpate all 5 node groups
- Supraclavicular fossa: both sides
- Contralateral breast
- Systemic: Liver, chest, spine (metastasis screen)
Differential Diagnosis Discussion
Present in order of likelihood based on your clinical findings
Investigation Discussion
Present as: "I would like to investigate this patient with...":
- Triple assessment
- Staging investigations based on suspected stage
Management Discussion
Present as: "I would manage this patient as follows...":
- MDT referral
- Staging
- Stage-specific management plan
Examiner Cross-Questions to Prepare
- "Why did you choose BCS over mastectomy?"
- "What would you do if margins are positive?"
- "How would you manage axillary nodes in this patient?"
- "What systemic therapy would you recommend?"
- "What are the indications for NACT?"
- "If the patient is BRCA positive, how does management change?"
16. IMPORTANT TABLES
High-Yield Comparison Tables
A. Prognosis by Histological Type
| Type | Prognosis |
|---|
| Tubular carcinoma | Best (excellent) |
| Cribriform carcinoma | Excellent |
| Mucinous (Colloid) | Very good |
| Medullary carcinoma | Good (despite high grade) |
| IDC-NST | Intermediate |
| ILC | Intermediate |
| Inflammatory breast cancer | Poor |
| Metaplastic carcinoma | Very poor |
B. Clinical Features Summary Table
| Feature | Benign | Malignant |
|---|
| Age | <40 | >40 |
| Pain | +/- | Usually absent |
| Lump consistency | Soft/firm | Hard/stony |
| Margins | Well-defined | Ill-defined |
| Mobility | Mobile | Fixed |
| Skin changes | Absent | Dimpling, peau d'orange |
| Nipple discharge | Multicolored | Blood-stained |
| Nodes | Soft, mobile | Hard, fixed, matted |
C. Operations for Breast Cancer - Evolution
| Era | Operation | Structures Removed |
|---|
| 1894 | Halsted's Radical Mastectomy | Breast + Pec Major + Pec Minor + LN |
| 1948 | Patey's MRM | Breast + Pec Minor + LN (Pec Major preserved) |
| 1963 | Auchincloss-Madden MRM | Breast + LN (both Pec muscles preserved) |
| 1970s | Simple Mastectomy | Breast only |
| 1980s | Lumpectomy / BCS | Tumor + margin only |
| 2000s | Oncoplastic Surgery | BCS with volume replacement/displacement |
| 2010s | Nipple-sparing Mastectomy | Breast tissue (preserve skin + NAC) |
17. FLOW CHARTS
A. Diagnostic Flowchart
BREAST LUMP
│
▼
CLINICAL ASSESSMENT
(Age, Duration, Features)
│
┌───┴────┐
│ │
<35 yrs >35 yrs
│ │
USG Mammogram
│ │
└───┬────┘
│
Solid or Indeterminate
│
▼
CORE NEEDLE BIOPSY + IHC
│
┌──┴──┐
Benign Malignant
│ │
Discharge Staging
│
▼
MDT Meeting
│
Stage-specific
Management
B. Axillary Management Flowchart
CLINICALLY NODE NEGATIVE (cN0)
│
▼
SLNB (intraoperative)
│
┌─────┴─────┐
SLN- SLN+
negative positive
│ │
No further 1-2 positive SLN?
axillary │
surgery ┌───┴──────┐
│ │
BCS + >2 SLN positive
WBRT │
│ ALND
Omit ALND (Levels I-III)
(Z0011 criteria)
CLINICALLY NODE POSITIVE (cN1+)
│
▼
Biopsy positive
axillary node
│
NACT → reassess
│
Surgery:
ALND or Axillary RT
C. Staging and Treatment Algorithm
CONFIRMED BREAST CANCER
│
STAGING WORKUP
│
┌────────┼────────┬──────────┐
│ │ │ │
Stage 0 Stage I-IIA Stage IIB-IIIC Stage IV
(DCIS) (Early) (Locally Adv.) (Metastatic)
│ │ │ │
BCS or Surgery NACT first Palliative
Mastect first then surgery systemic
+ RT then + RT therapy
+Tamox adjuvant ± surgery
therapy (local control)
18. MIND MAP
CARCINOMA BREAST
│
┌─────────────────────┼──────────────────────┐
│ │ │
ETIOLOGY PATHOLOGY CLINICAL
──────── ───────── ───────
BRCA1/2 IDC-NST (70%) Painless lump (UOQ)
ER exposure ILC (10%) Skin dimpling
Radiation DCIS/LCIS Peau d'orange
HRT TNM Stages 0-IV Nipple retraction
Nulliparity Molecular: Blood discharge
Age >40 LumA, LumB, Axillary nodes
Obesity HER2, TNBC Paget's nipple
│ │ │
INVESTIGATIONS SURGERY SYSTEMIC THERAPY
──────────── ─────── ───────────────
Triple Assessment BCS (+ WBRT) Chemo (AC-T)
Mammogram (BI-RADS) MRM (Patey's) Hormonal (Tamox/AI)
USG breast SLNB / ALND HER2 (Trastuzumab)
Core biopsy Oncoplastic PARP (Olaparib)
IHC (ER/PR/HER2) Nipple-sparing CDK4/6 inhibitors
Staging CT/PET Prophylactic Immunotherapy (Pemb)
19. IMAGES AND VISUAL REFERENCES
Key images to recognize in exam (from standard textbooks):
Clinical photographs:
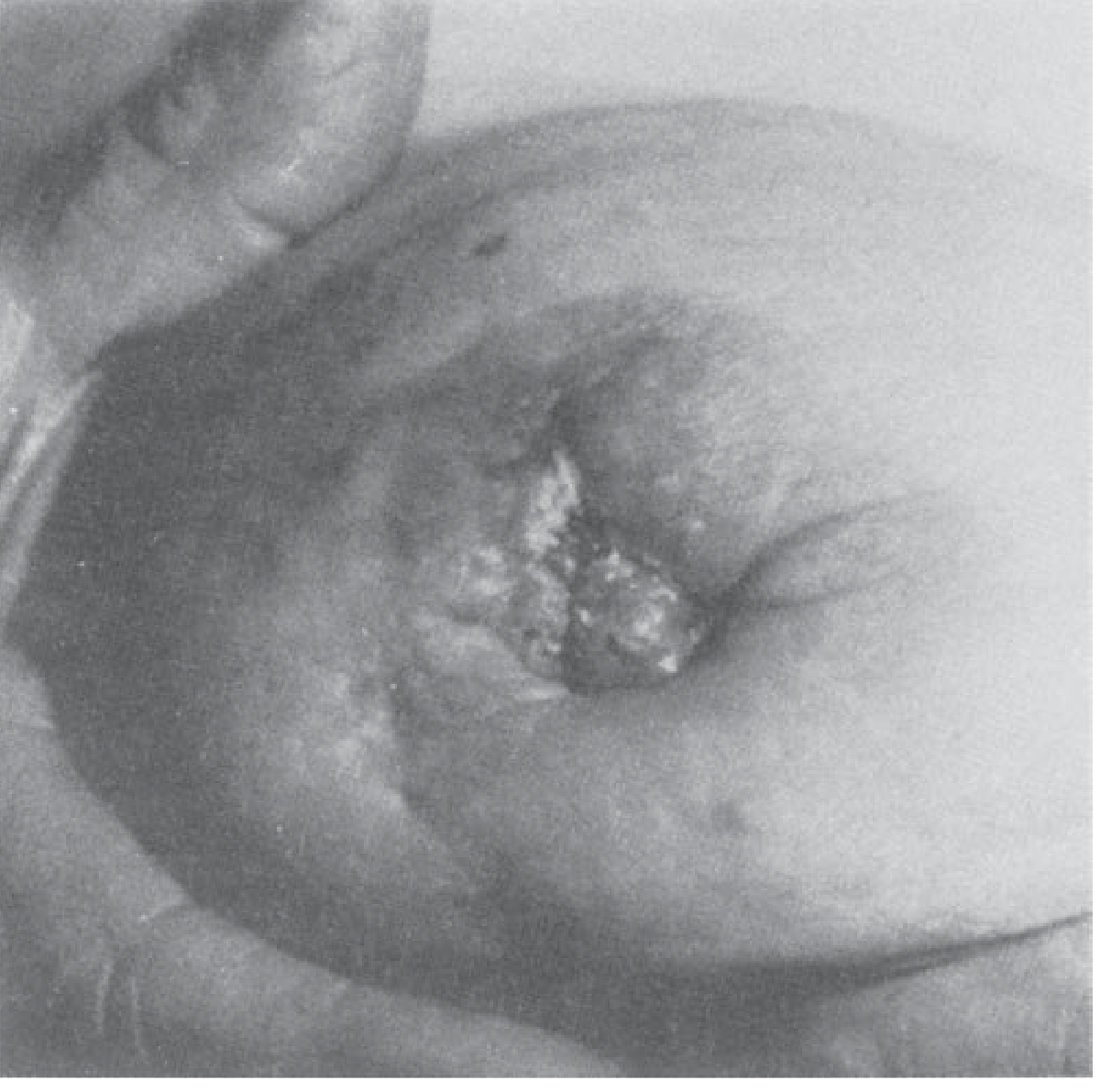
- Peau d'orange (dermal lymphatic invasion)
- Skin dimpling (Cooper's ligament tethering)
- Paget's disease of nipple (eczematous nipple change)
- Inflammatory breast cancer (erythema + edema)
- Fungating/ulcerating breast mass (T4b)
- Lymphedema of arm post-mastectomy
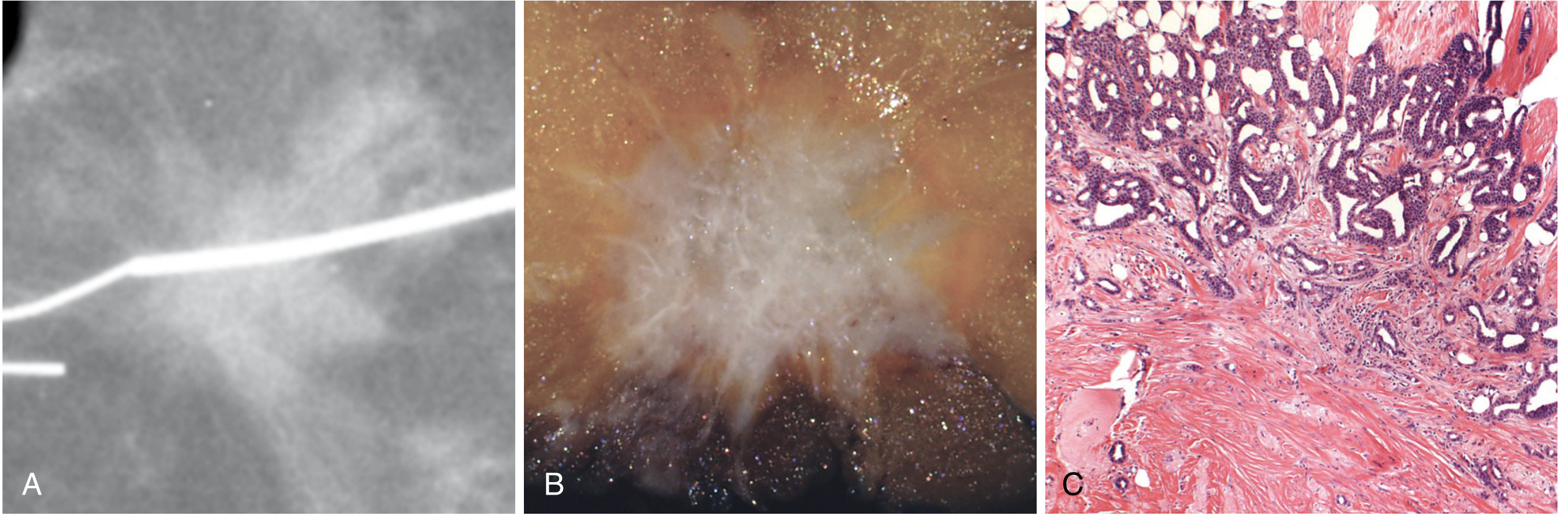
Mammographic features of malignancy:
- Spiculated/stellate mass
- Clustered pleomorphic microcalcifications (comedo DCIS)
- Architectural distortion
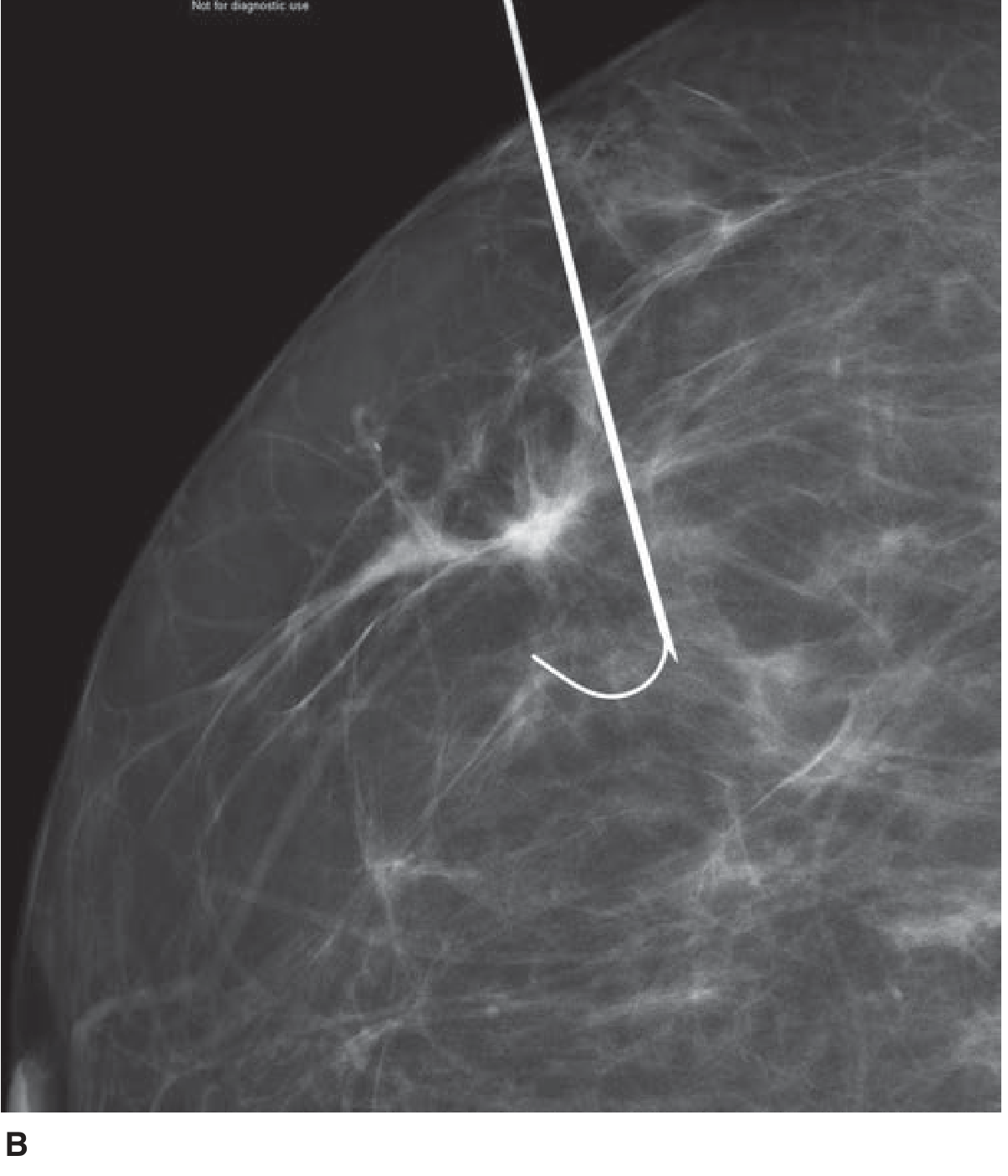
- Asymmetric density
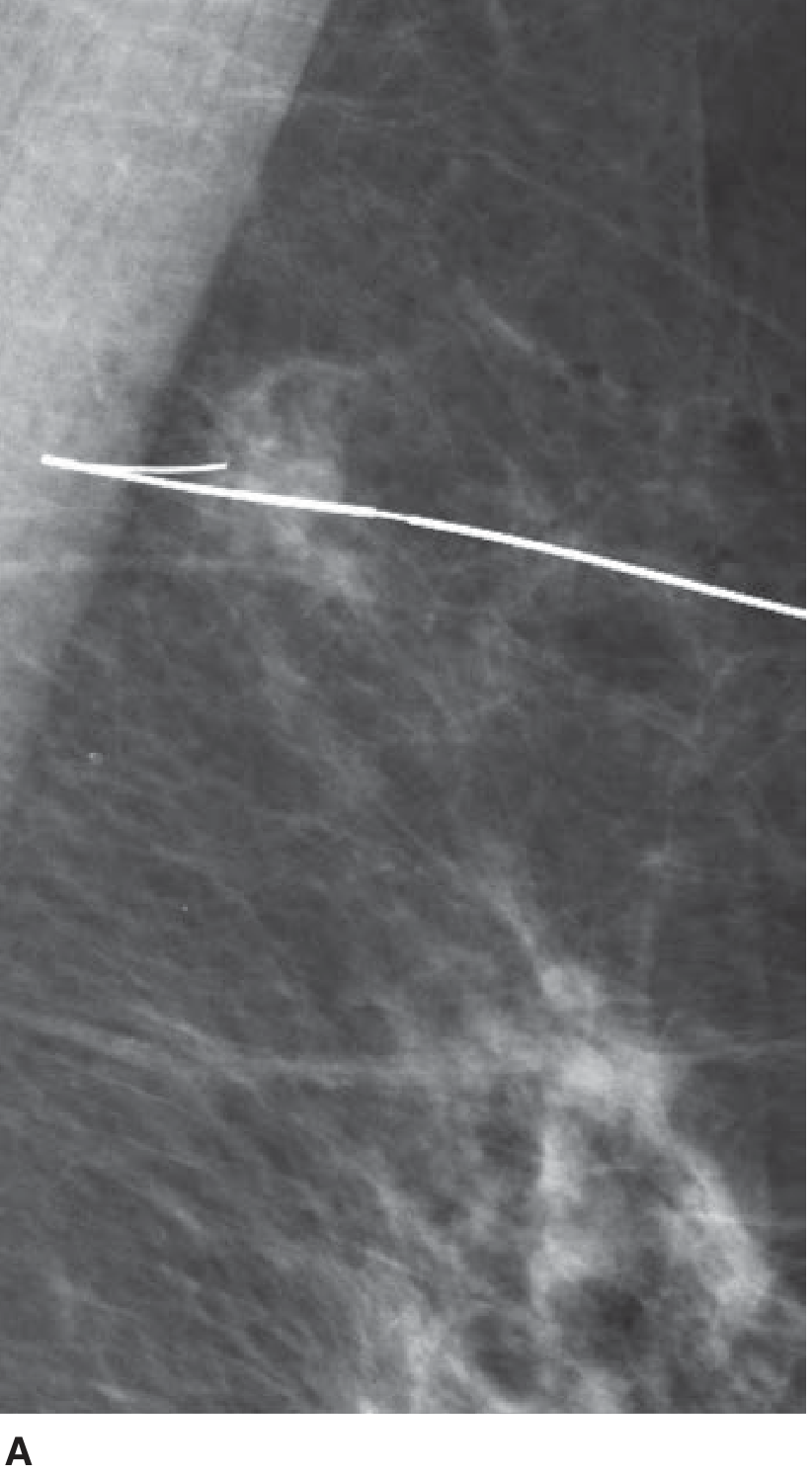
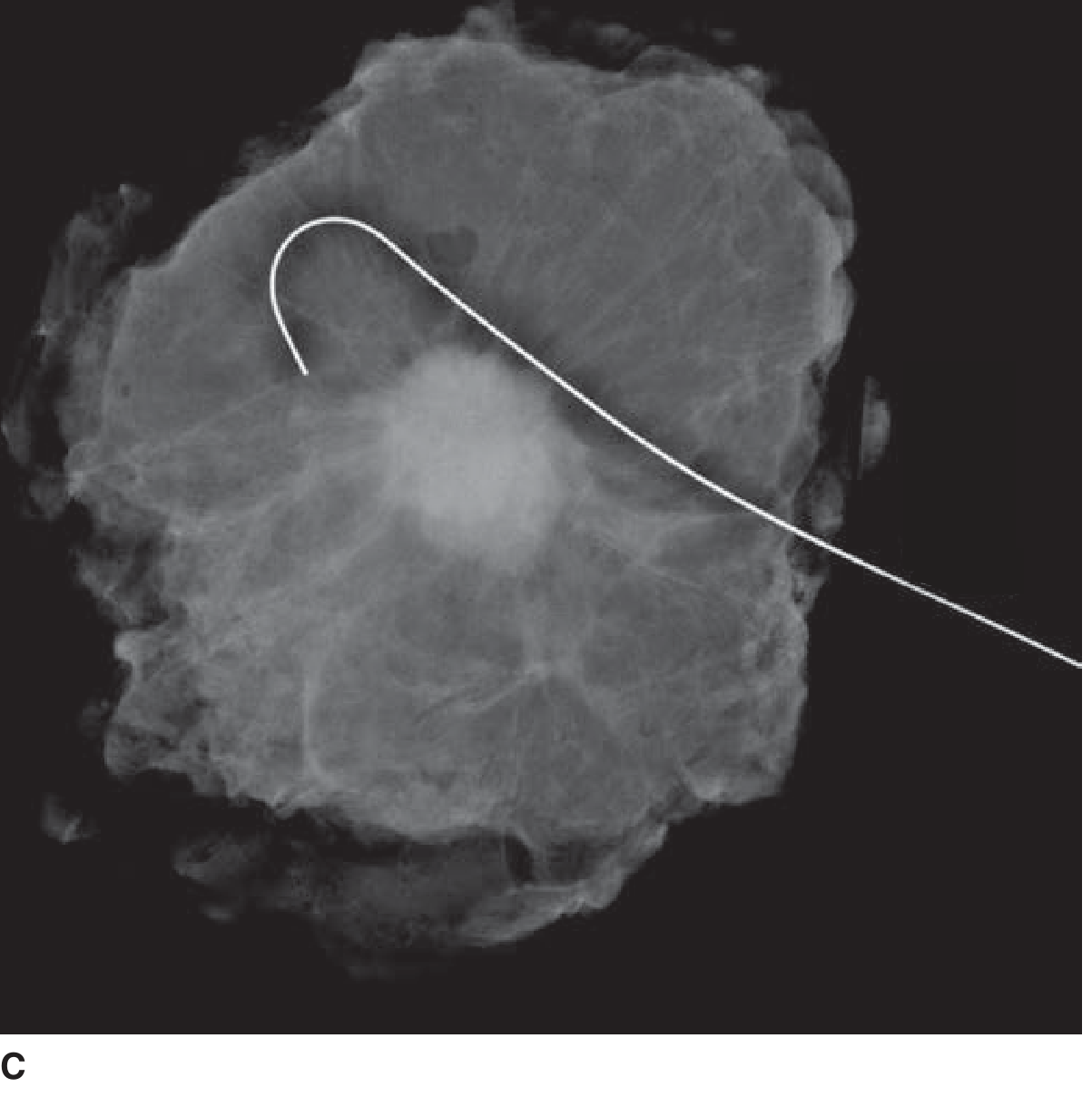
Wire localization procedure - mammographic image of hookwire in left breast. (Schwartz's Principles of Surgery, 11th Ed., Fig. 17-33)
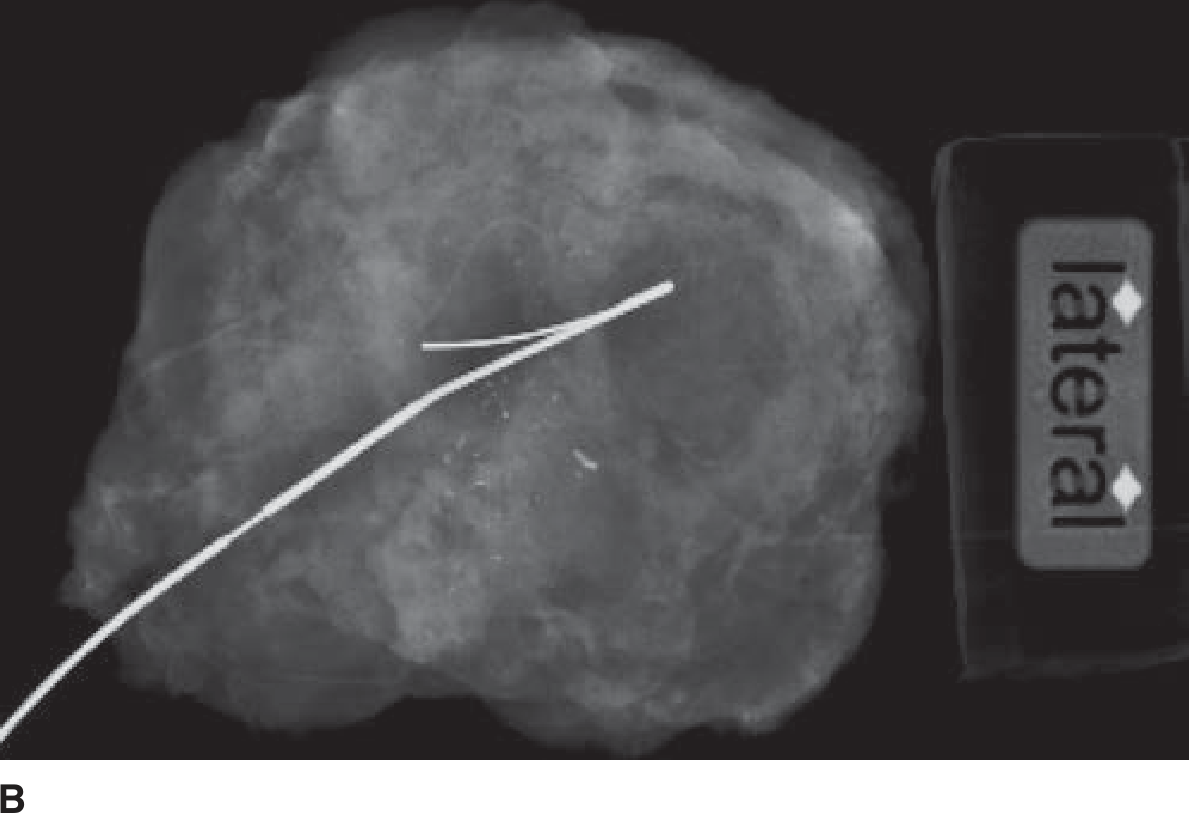
Specimen mammography (confirming excision of targeted lesion with hookwire):
Specimen mammogram demonstrating excision of targeted density. (Schwartz's Principles of Surgery, 11th Ed., Fig. 17-34)
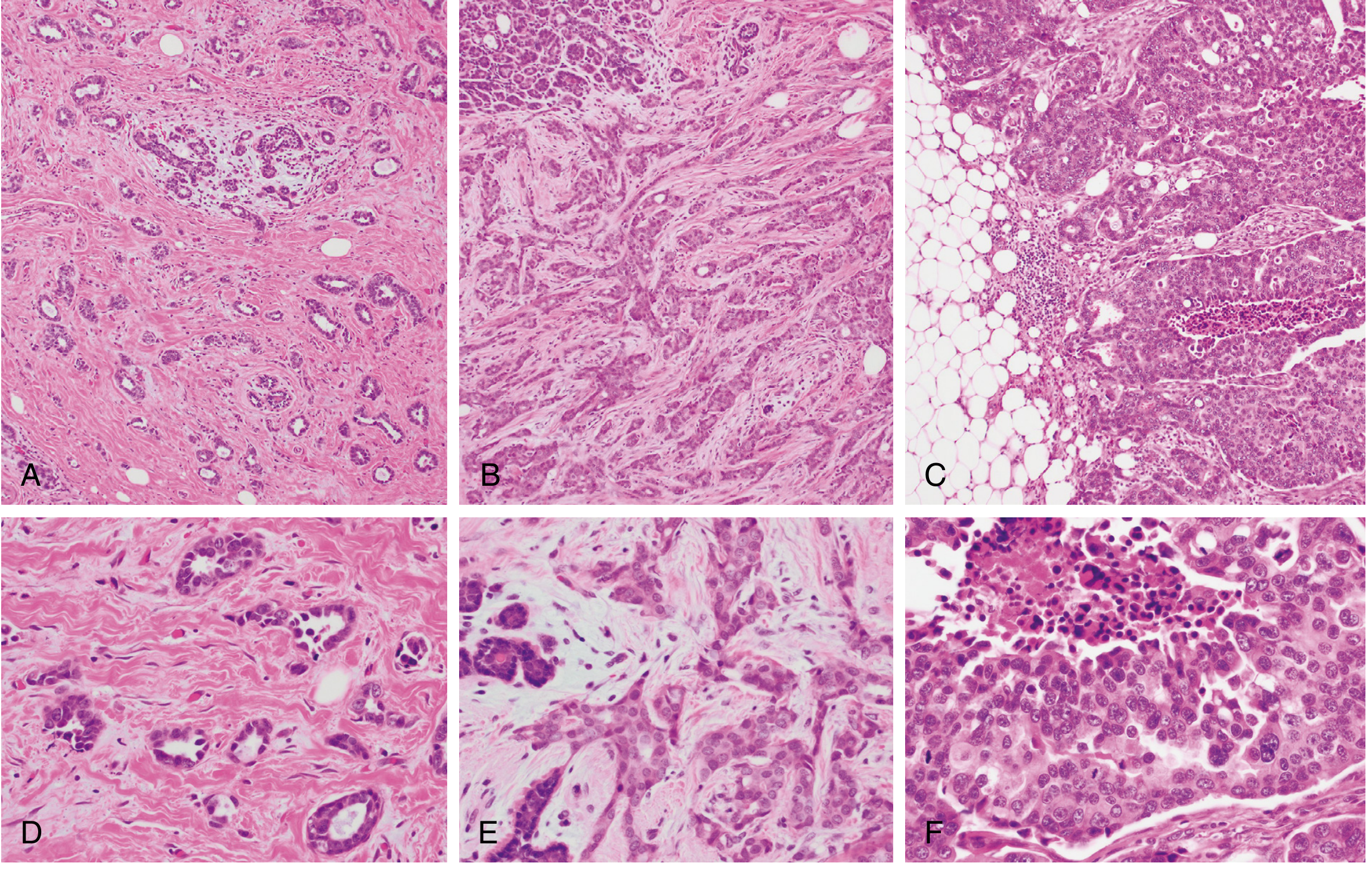
Gross and histopathology specimens to recognize:
- Scirrhous carcinoma - hard, gritty cut surface, stellate appearance
- Medullary carcinoma - soft, fleshy, pushing margins
- Mucinous carcinoma - gelatinous appearance
- DCIS with comedo necrosis - toothpaste-like material expressed from ducts
20. INSTRUMENTS
Key Instruments in Breast Surgery
| Instrument | Use |
|---|
| 14G Tru-cut/core biopsy needle | Core needle biopsy under USG guidance |
| 21G/23G fine needle | FNAC under USG guidance |
| Mammotome (vacuum-assisted biopsy) | Large volume excision biopsy for calcifications |
| Hookwire (Kopans wire) | Wire-guided localization for impalpable lesions |
| Hand-held gamma probe | SLNB - detection of Tc-99m hot nodes |
| Ligasure / Harmonic scalpel | Haemostatic dissection in axillary clearance |
| Self-retaining retractors | Mastectomy wound exposure |
| Skin stapler | Wound closure |
| Closed suction drain (Redivac/Jackson-Pratt) | Post-operative drainage (axilla + inferior flap) |
Examiner's instrument viva:
- Show a 14G core biopsy needle: "What is this? What gauge is used? What are its advantages over FNAC?"
- Show a Kopans hookwire: "How is this used preoperatively? What is the purpose?"
- Show a gamma probe: "What is the principle of SLNB? What radioisotope is used? How much radioactivity?"
21. SURGICAL PEARLS
Bailey & Love Pearls
- BCS = mastectomy in terms of overall survival (Bailey & Love, 28th Ed.)
- Peau d'orange = dermal lymphatic blockade (NOT inflammatory unless red + warm + ≥1/3 breast affected)
- LCIS = bilateral risk marker, not anatomic precursor
- Internal mammary nodes: important route for medial quadrant tumors; often overlooked
Schwartz Pearls
- In LCIS, up to 65% of subsequent invasive cancers are ductal, not lobular (Schwartz, 11th Ed.)
- ACOSOG Z0011: ALND can be safely omitted in selected SLNB-positive patients
- MRI breast: mandatory for BRCA mutation carriers starting age 25 for annual screening
Operative Pearls (OT)
- Always orient the mastectomy specimen with sutures/clips for the pathologist (superior, medial, lateral, deep margins)
- Raise skin flaps at correct plane (subdermal, 5-8 mm thick) to preserve subdermal plexus and prevent necrosis
- Identify long thoracic nerve early - it lies on the surface of serratus anterior on the medial wall of the axilla
- Thoracodorsal nerve identified by following the thoracodorsal vessels on subscapularis
Emergency Pearls
- Inflammatory breast cancer = NACT first; NEVER take straight to mastectomy
- Spinal cord compression = ONCOLOGICAL EMERGENCY - dexamethasone immediately + urgent MRI
- Hypercalcemia = IV normal saline + furosemide + zoledronic acid
- Pathological fracture = orthopaedic stabilization + RT
Resident Tips
- Always do triple assessment - a single negative result does not exclude malignancy
- Core biopsy > FNAC for treatment planning (receptor status, grade, architecture)
- Always examine the contralateral breast and both axillae
- Ask about family history every single time
- For exam: know Haagensen's criteria of inoperability - frequently asked
22. RECENT GUIDELINES (2024-2025)
NCCN Guidelines Version 5.2025 (Key Updates)
| Topic | NCCN 2025 Recommendation |
|---|
| APBI/PBI | Endorsed for ER+ IDC ≤2 cm (pT1), Grade 1-2, node-negative, age ≥40, no BRCA mutation (ASTRO 2024 criteria) |
| Hypofractionation RT | Preferred over conventional fractionation for most patients (40 Gy/15# equivalent) |
| NACT for TNBC | Pembrolizumab + chemotherapy (AC-T) neoadjuvant → pembrolizumab adjuvant (KEYNOTE-522) |
| Residual disease TNBC | Capecitabine adjuvant (CREATE-X) or olaparib (BRCA-mutated, OlympiA) |
| Residual disease HER2+ | T-DM1 (trastuzumab emtansine) adjuvant (KATHERINE) |
| ER+/HER2- metastatic | CDK4/6 inhibitor (palbociclib/ribociclib/abemaciclib) + endocrine therapy = standard first-line |
| Trastuzumab deruxtecan (T-DXd) | Second-line HER2+ metastatic; also HER2-low (IHC 1+ or 2+/FISH-) |
| Olaparib | Adjuvant for BRCA-mutated, HER2-negative, high-risk early breast cancer |
| Elacestrant | ESR1-mutated ER+/HER2- metastatic (second-line) |
| Axillary management | Z0011 criteria still standard; ALND can be omitted in selected cN1-SLN+ with BCS + WBRT |
Recent PubMed Evidence Updates (2024-2025)
- PMID 39878175 (Int J Surg, 2025): Systematic review - SLNB after NACT in clinically node-positive breast cancer achieves adequate accuracy when ≥3 SLN removed; false-negative rate acceptable
- PMID 38808740 (Asia Pac J Clin Oncol, 2025): BCS vs. mastectomy for metaplastic breast cancer - no significant survival difference; BCS feasible when adequate margins achievable
- PMID 39370318 (Surgery, 2024): Systematic review of surgical treatment in older (≥70 yrs) breast cancer patients - surgery + RT equivalent survival to mastectomy; deescalation strategies valid
23. HIGH-YIELD EXAM SECTION
⭐ Frequently Asked MS/DNB Questions
- Enumerate risk factors for carcinoma breast
- Describe triple assessment of breast lump
- Classification of breast carcinoma
- Discuss management of early breast cancer
- What is modified radical mastectomy? Describe Patey's operation
- TNM staging of breast cancer with prognosis
- Management of axillary lymph nodes in breast cancer
- Sentinel lymph node biopsy - technique, indications, significance
- Indications and contraindications of BCS
- What is DCIS? How is it managed?
⭐ Viva Favourites (One-Liners)
- Most common carcinoma = IDC-NST (70-80%)
- Most common site = Upper outer quadrant (50%)
- Gold standard for diagnosis = Triple Assessment + Core biopsy
- Most important prognostic factor = Axillary lymph node status
- Most common early complication of ALND = Seroma
- Most common late complication = Lymphedema
- Nerve causing winged scapula = Long thoracic nerve of Bell
- BRCA1 site = 17q21; BRCA2 site = 13q12.3
- Inflammatory breast = T4d stage
- Paget's cells = large, pale cells with clear halo in epidermis
- Nottingham grade: tubules + nuclear pleomorphism + mitoses
- Halsted = pec major removed; Patey = pec major preserved
⭐ Examiner's Favourite Traps
- ❌ "Peau d'orange = inflammatory carcinoma" → WRONG. Peau d'orange = dermal lymphatic blockade (any invasive cancer). Inflammatory = erythema + warmth + ≥1/3 breast (T4d)
- ❌ "LCIS is a precursor lesion" → WRONG. LCIS is a RISK MARKER (bilateral, diffuse risk). DCIS is the true precursor
- ❌ "ALND is always needed for positive SLNB" → WRONG after Z0011 trial (1-2 SLN+ with BCS + WBRT can omit ALND)
- ❌ "Inflammatory breast cancer - do emergency mastectomy" → WRONG. NACT first; surgery later
- ❌ "Halsted = Patey" → Halsted removes pec major; Patey preserves pec major but removes pec minor
- ❌ "Fat necrosis is benign, no biopsy needed" → WRONG. Must biopsy to exclude carcinoma
⭐ OSCE Stations
Station 1 - Spot diagnosis: "What is peau d'orange? Describe its mechanism."
Station 2 - Mammogram interpretation: "Describe this mammogram - spiculated mass with microcalcifications."
Station 3 - Instrument: "Identify this 14G needle. What is it used for? What are its advantages?"
Station 4 - Clinical examination: "Examine this breast lump and present your findings."
Station 5 - Management discussion: "A 48-year-old woman has a 3 cm IDC, ER+/HER2-, cN1. How do you manage?"
⭐ Mnemonics
Risk factors - "ABCDEF HHHHH RLNO":
- Age >40, Alcohol
- BRCA 1/2, Breast density, Breastfeeding (protective)
- Combined HRT, Contralateral breast cancer
- Dense breast tissue
- Early menarche, Evidence of radiation
- Family history, Fat (obesity)
- HRT use, High estrogen exposure, Hormone contraceptives
- Radiation, Race (Western)
- Late menopause, Late first pregnancy
- Nulliparity
- Ovarian cancer in family
Axillary node groups - "SCALPEL":
- Subscapular (posterior)
- Central
- Apical (Level III)
- Lateral (axillary vein)
- Pectoral (anterior, Level I)
- External mammary
- Level classification (I, II, III)
24. SUMMARY
One-Page Revision Sheet
| Category | Key Points |
|---|
| Definition | Malignant epithelial tumor from ductal/lobular epithelium |
| Incidence | #1 female cancer worldwide; 2.3 million/year (2020) |
| Most common type | IDC-NST (70-80%) |
| Most common site | UOQ (50%) |
| Risk factors | Age, BRCA, early menarche/late menopause, nulliparity, HRT, radiation, family history |
| Key genes | BRCA1 (17q21) - TNBC; BRCA2 (13q12.3) - multiple cancers |
| Diagnosis | Triple Assessment (Clinical + Imaging + Pathology) |
| Gold standard | Core needle biopsy + IHC for ER/PR/HER2/Ki67 |
| Staging | AJCC TNM 8th edition; Bone > Lung > Liver > Brain metastases |
| Surgery | BCS + WBRT (= mastectomy outcomes) OR MRM; SLNB (cN0) / ALND (cN+) |
| Halsted vs Patey | Halsted = pec major out; Patey = pec major in, pec minor out |
| Systemic | Chemo (AC-T); Hormonal (Tamox/AI); HER2 (Trastuzumab); PARP (Olaparib-BRCA) |
| Prognosis | Most important = Axillary LN status |
| Key nerve | Long thoracic nerve of Bell = winged scapula if injured |
| Key complication | Seroma (early); Lymphedema (late) |
| Guidelines | NCCN 2025; ASTRO 2024 (APBI); Z0011 (omit ALND); KATHERINE (T-DM1) |
50 Rapid-Fire Viva Q&A
- Most common female cancer worldwide? Breast cancer
- Most common histological type? IDC-NST
- Best initial investigation in <35 yrs? USG breast
- Best initial investigation in >35 yrs? Mammography
- Gold standard tissue diagnosis? Core needle biopsy
- BI-RADS 4 management? Tissue biopsy
- Most common site of breast cancer? UOQ (50%)
- Triple negative = which molecular type? Basal-like / TNBC
- BRCA1 location? 17q21
- BRCA2 associated malignancy (male)? Prostate cancer
- Nottingham grade components? Tubules + Nuclear pleomorphism + Mitoses
- Grade 1 score? 3-5
- Haagensen's inoperability - arm edema signifies? N3 axillary nodes
- T4d = ? Inflammatory breast cancer
- Inflammatory cancer - initial treatment? Neoadjuvant chemotherapy (NOT surgery)
- DCIS - true precursor or risk marker? True precursor
- LCIS - true precursor or risk marker? Risk marker
- Comedo DCIS - radiological feature? Clustered pleomorphic microcalcifications
- Peau d'orange mechanism? Dermal lymphatic blockade causing skin edema
- Paget's disease starts at? Nipple (not areola)
- Z0011 trial significance? ALND can be omitted in 1-2 positive SLN with BCS+WBRT
- Most important prognostic factor? Axillary lymph node status
- Batson's plexus significance? Haematogenous spread to spine without portal circulation
- Most common bone for breast metastasis? Vertebral column
- Most common early complication of ALND? Seroma
- Most common late complication? Lymphedema
- Nerve causing winged scapula? Long thoracic nerve of Bell
- Thoracodorsal nerve injury effect? Weak arm adduction/extension
- Intercostobrachial nerve injury effect? Numbness upper inner arm
- Halsted mastectomy preserves? Nothing; pec major removed
- Patey's mastectomy preserves? Pectoralis major
- Auchincloss-Madden preserves? Both pectoralis muscles
- Standard yield in ALND? ≥10 lymph nodes
- SLNB dye? Patent Blue/Methylene Blue + Tc-99m nanocolloid
- Sentinel node identification rate? 95-98%
- SLNB false negative rate? 5-10%
- Indication for MRI in breast? BRCA carriers, occult primary, preoperative planning, neoadjuvant monitoring
- OncotypeDx - what does it measure? 21-gene recurrence score; guides need for chemotherapy in ER+
- Trastuzumab target? HER2 extracellular domain
- Trastuzumab side effect? Cardiotoxicity (cardiomyopathy)
- PARP inhibitor used in breast cancer? Olaparib (for BRCA-mutated)
- pCR = ? Pathological complete response (no residual invasive cancer after NACT)
- Residual disease after NACT in HER2+? T-DM1 adjuvant (KATHERINE trial)
- Residual disease after NACT in TNBC? Capecitabine (CREATE-X) or Olaparib if BRCA+
- CDK4/6 inhibitors - example + use? Palbociclib/Ribociclib/Abemaciclib; metastatic ER+/HER2-
- Stewart-Treves syndrome? Lymphangiosarcoma in chronic post-mastectomy lymphedema
- Toilet mastectomy? Palliative mastectomy for fungating Stage IV tumor
- Prophylactic mastectomy reduces risk by? ~90%
- FAST-Forward trial? 5×5.4 Gy (1 week) equivalent to 40 Gy/15# (3 weeks)
- ASTRO 2024 APBI criteria (age)? ≥40 years, T1, ER+, node-negative, Grade 1-2, no BRCA
20 MCQs
- Most common carcinoma of breast: (a) ILC (b) IDC-NST (c) Medullary (d) Mucinous
- Most important prognostic factor: (a) Tumor size (b) Grade (c) Axillary node status (d) Receptor status
- BRCA1 chromosome location: (a) 13q12 (b) 17p13 (c) 17q21 (d) 22q12
- Berg's Level II nodes are: (a) Lateral to pec minor (b) Behind pec minor (c) Medial to pec minor (d) Along axillary vein
- Sentinel node is identified by: (a) CT scan (b) Bone scan (c) Blue dye + Tc99m probe (d) PET
- Winged scapula results from injury to: (a) Thoracodorsal (b) Intercostobrachial (c) Long thoracic nerve (d) Lateral pectoral
- Inflammatory breast cancer stage: (a) T3 (b) T4a (c) T4b (d) T4d
- ACOSOG Z0011 trial: ALND omission is safe with: (a) Any positive SLN (b) ≥3 positive SLN (c) 1-2 positive SLN + BCS + WBRT (d) All N1 disease
- Best imaging in a 28-year-old with breast lump: (a) Mammography (b) MRI (c) USG (d) PET-CT
- Nottingham Grade - best prognosis score: (a) 8-9 (b) 6-7 (c) 3-5 (d) All equal
- DCIS vs. LCIS - which is a true precursor: (a) DCIS (b) LCIS (c) Both (d) Neither
- HER2 3+ on IHC means: (a) Negative (b) Equivocal (c) Positive - trastuzumab eligible (d) Requires FISH
- Paget's disease starts at: (a) Areola (b) Nipple (c) Upper outer quadrant (d) Chest wall
- Protective factor for breast cancer: (a) Late menopause (b) HRT (c) Early first pregnancy + breastfeeding (d) Radiation
- Most common site of distant metastasis: (a) Lung (b) Liver (c) Brain (d) Bone
- Residual disease after NACT in HER2+: (a) Trastuzumab alone (b) Capecitabine (c) T-DM1 (trastuzumab emtansine) (d) Pertuzumab
- Comedo DCIS characterized by: (a) Low grade (b) High grade + necrosis + microcalcifications (c) Absent necrosis (d) All types equally
- Patey's operation removes: (a) Pec major only (b) Pec major + minor (c) Breast + axillary LN + pec minor (pec major preserved) (d) Breast only
- BRCA2 male breast cancer - most common associated malignancy: (a) Pancreatic (b) Prostate cancer (c) Colon (d) Gastric
- Peau d'orange mechanism: (a) Direct skin invasion (b) Cooper's ligament tethering (c) Dermal lymphatic blockade causing skin edema (d) Tumor ulceration
10 Clinical Scenarios
Scenario 1: A 45-year-old woman presents with a 3 cm hard, irregular, painless lump in the right upper outer quadrant with skin dimpling but no axillary nodes. What is your approach?
→ Triple assessment: Clinical exam, Mammogram ± USG, Core biopsy + IHC. If malignant: staging (CXR, LFTs, ALP), MDT, Stage IIA (T2N0) → BCS + SLNB + WBRT + adjuvant systemic therapy based on receptor status.
Scenario 2: 55-year-old postmenopausal woman, breast cancer 4 cm, ER+/PR+/HER2-, clinically cN0 on ultrasound. Is she eligible for BCS?
→ Yes, if breast size allows adequate margins. Stage IIB (T2N0→ wait for pathological staging). Plan: BCS + SLNB + WBRT + Aromatase inhibitor (Letrozole) for 5-10 years.
Scenario 3: 38-year-old woman, BRCA1 positive, no current cancer detected. What is management?
→ Annual MRI from age 25; annual mammogram from age 30; discuss risk-reducing bilateral mastectomy (reduces risk by 90%); bilateral salpingo-oophorectomy at 35-40 after completing family; chemoprevention with tamoxifen.
Scenario 4: 50-year-old woman, biopsy-proven IDC, HER2+++. Neoadjuvant chemotherapy planned. What regime?
→ Pertuzumab + Trastuzumab + Docetaxel + Carboplatin (TCHP - Taxere, Carboplatin, Herceptin, Perjeta). If pCR achieved → trastuzumab alone adjuvant. If residual disease → T-DM1 adjuvant (KATHERINE trial).
Scenario 5: Post-mastectomy day 3 - patient has 200 mL drain output. What is the management?
→ Seroma/hematoma. If drain output >30 mL/day → keep drain. Compression bandage. If hematoma: re-explore. Drain removed only when <30 mL/day for 2 consecutive days.
Scenario 6: Patient develops arm swelling 6 months after MRM + ALND. How do you manage?
→ Lymphedema. Measure limb circumference. Exclude recurrence (lymph node biopsy if hard/new nodes). Management: Complete Decongestive Therapy (CDT), compression garments, Manual Lymphatic Drainage, physiotherapy, elevate arm.
Scenario 7: 42-year-old with diffuse erythema, warmth, pitting edema of entire right breast. Core biopsy shows IDC with dermal lymphatics packed with tumor cells. What is management?
→ Inflammatory breast cancer (T4d, Stage IIIB). NACT first (anthracycline + taxane + HER2-directed if HER2+). After response: modified radical mastectomy + PMRT. NOT amenable to BCS.
Scenario 8: A 62-year-old woman, known breast cancer (ER+), presents with severe back pain. X-ray shows vertebral collapse L2. What is emergency management?
→ Rule out spinal cord compression: urgent MRI spine. If cord compression: IV dexamethasone 8-16 mg immediately + urgent radiotherapy ± surgical decompression. Start bisphosphonate (Zoledronic acid 4 mg IV).
Scenario 9: FNAC of breast lump shows C3 (atypical). What is the next step?
→ C3 = uncertain/atypical. Proceed to core needle biopsy (cannot exclude malignancy on FNAC alone). If core biopsy also equivocal → excision biopsy.
Scenario 10: 70-year-old woman with 2 cm ER+ IDC, unfit for general anesthesia. What are options?
→ Consider primary endocrine therapy (tamoxifen or letrozole) for hormone-sensitive tumor. For surgery: local anesthesia ± sedation for BCS. Discuss risks/benefits of different approaches with MDT. Recent evidence supports deescalation of surgery in elderly (PMID 39370318).
5 OSCE Stations
OSCE Station 1 - Clinical Examination
Task: "Examine the breast of this patient and present your findings"
Expected: Inspection (4 positions) → Palpation of all quadrants + axillary tail → Axillary examination → Supraclavicular → Contralateral breast → Present findings in structured format
OSCE Station 2 - Radiology
Task: "Describe this mammogram" (shows spiculated mass with microcalcifications)
Expected: Identify spiculated mass, architectural distortion, microcalcifications. Classify as BI-RADS 5. State need for core biopsy.
OSCE Station 3 - Instrument
Task: "Identify this instrument and describe its use"
Expected: Identify core biopsy needle (14G Tru-cut). Describe USG-guided technique, advantages over FNAC, what information it provides (histology, grade, receptor status).
OSCE Station 4 - History Taking
Task: "Take a focused history from this patient with breast lump"
Expected: Duration, progression, pain, discharge, skin changes. Menstrual/obstetric history. Family history. Metastatic symptoms. Risk factor assessment.
OSCE Station 5 - Counselling
Task: "Counsel this patient who has been diagnosed with Stage IIA breast cancer about surgical options"
Expected: Explain BCS vs. mastectomy, equivalence in survival, need for radiotherapy after BCS, lymph node assessment (SLNB), reconstruction options, multidisciplinary care.
Top 10 Examiner Take-Home Messages
- Triple assessment is the cornerstone of breast diagnosis - never rely on clinical examination alone
- Core biopsy > FNAC - provides histology, grade, receptor status needed for treatment planning
- BCS = mastectomy in survival outcomes when followed by radiotherapy (Level 1 evidence - NSABP B-06, Milan trials)
- Axillary lymph node status = most important single prognostic factor
- LCIS = risk marker (bilateral, 1-2%/year); DCIS = true precursor (must treat)
- Inflammatory breast cancer - NACT first, mastectomy later; never take to OT initially
- Z0011 trial changed axillary surgery - 1-2 positive SLN + BCS + WBRT = ALND can be omitted
- BRCA1 (17q21) = TNBC type; BRCA2 (13q12.3) = multiple organ cancers; prophylactic mastectomy reduces risk by 90%
- Know your nerve anatomy - long thoracic nerve = winged scapula; thoracodorsal nerve = latissimus dorsi; protect both in ALND
- Modern breast cancer management is molecular and individualized - receptor status drives every treatment decision; the era of one-size-fits-all surgery is over
Sources: Bailey & Love's Short Practice of Surgery (28th Ed.), Schwartz's Principles of Surgery (11th Ed.), Robbins Cotran Pathologic Basis of Disease (10th Ed.), Fischer's Mastery of Surgery (8th Ed.), NCCN Guidelines Version 5.2025, ASTRO 2024 Consensus, ACOSOG Z0011, KATHERINE Trial, KEYNOTE-522, OlympiA Trial, CREATE-X Trial, PubMed recent evidence (2024-2026)