Pathological myopia and how is it treated
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pathological myopia" AND treatment
Reading File
Finding Sources
Searching PubMed
"myopia" AND "choroidal neovascularization" AND "anti-VEGF"
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full response:
Pathological Myopia
Definition and Epidemiology
Pathological (degenerative) myopia is characterized by progressive anteroposterior elongation of the scleral envelope accompanied by a range of secondary ocular changes, principally thought to result from mechanical stretching of involved tissues. A refractive error of more than -6 dioptres is the common threshold for high myopia, with axial length typically exceeding 26 mm.
- Affects >2% of adult Western European/American populations
- Up to ~10% prevalence in East Asian populations
- It is a significant cause of legal blindness, with maculopathy being the most common driver of visual loss
Pathological Features (Fundus Findings)
| Feature | Description |
|---|---|
| Tessellated (tigroid) fundus | Diffuse RPE attenuation exposing large choroidal vessels |
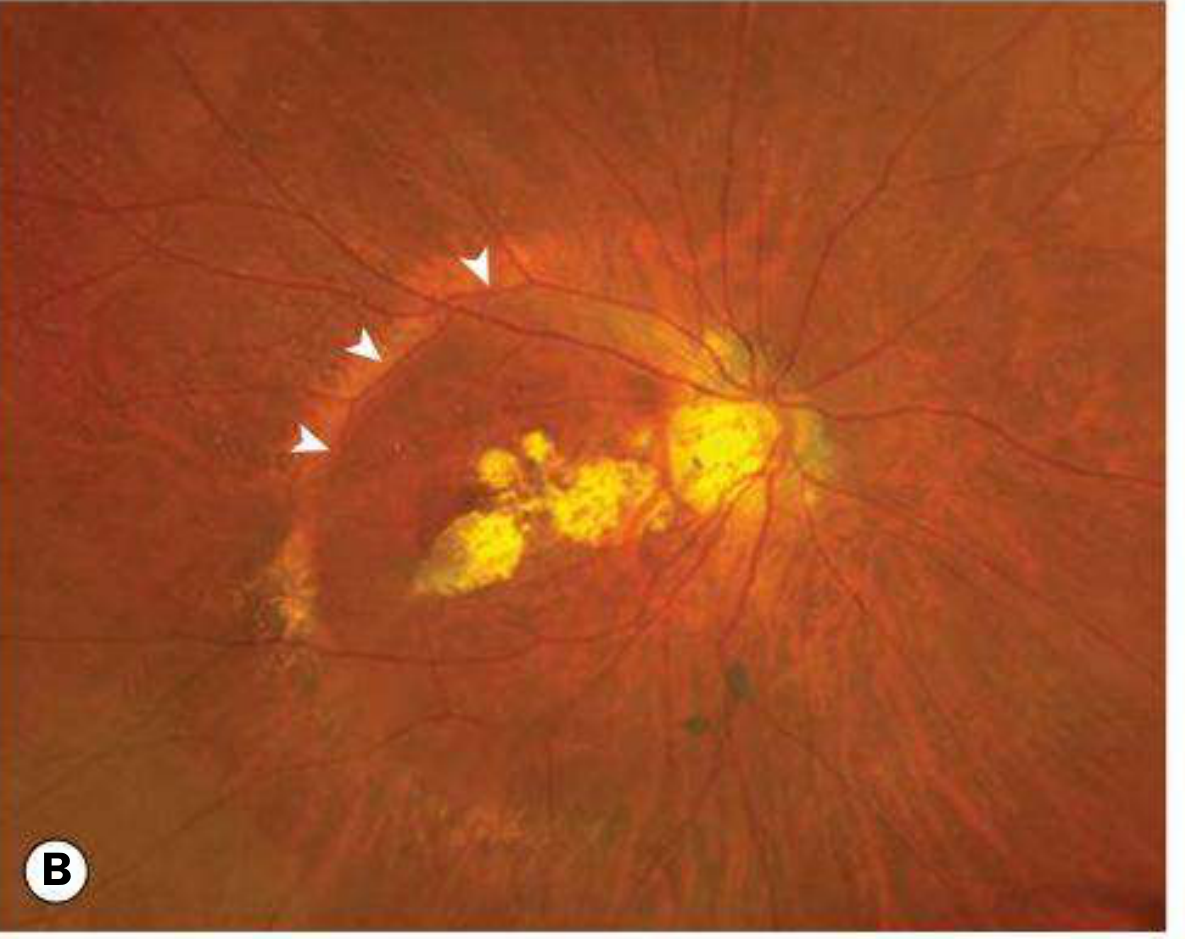
| Focal chorioretinal atrophy | Patchy visibility of choroidal vessels and often the sclera |
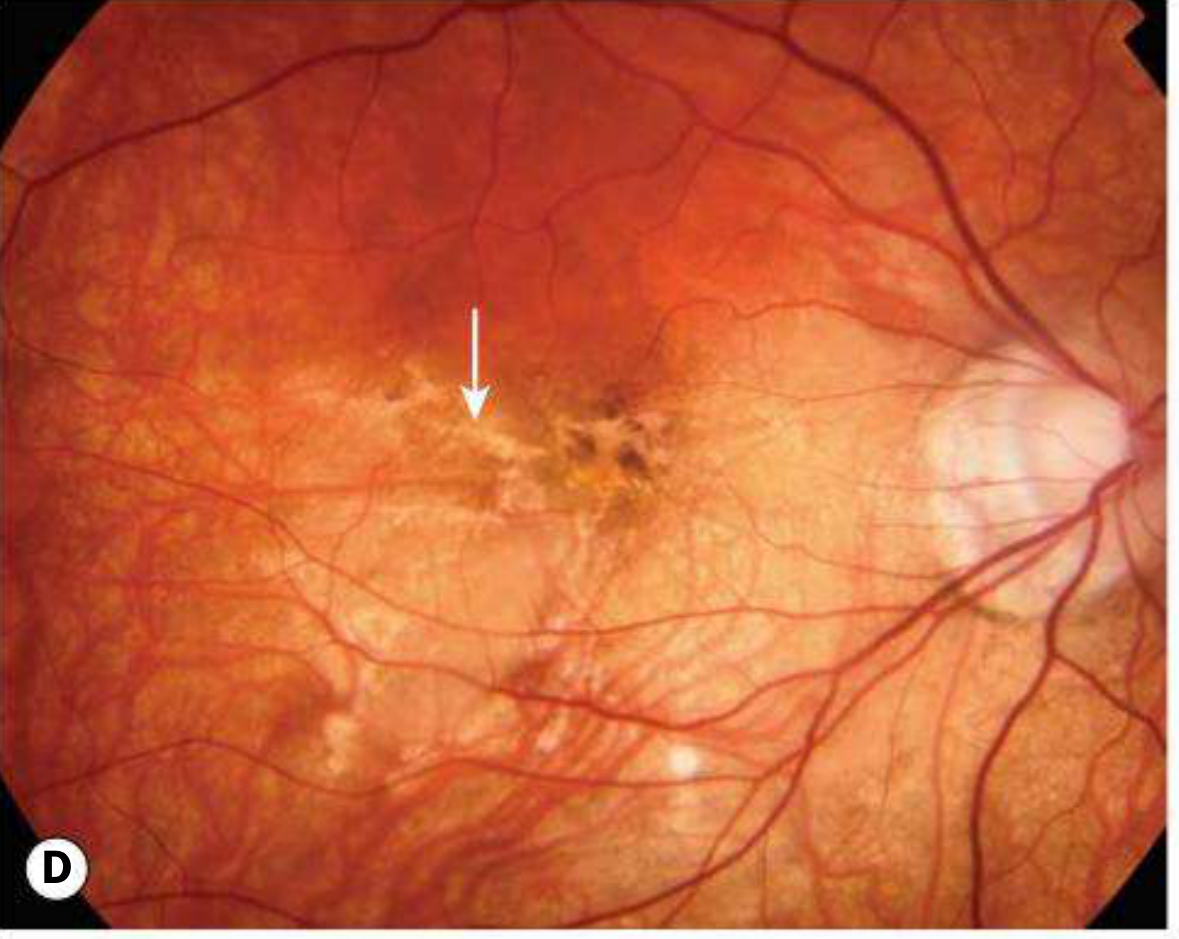
| Lacquer cracks | Ruptures in the RPE-Bruch membrane-choriocapillaris complex; fine irregular yellow lines at the posterior pole (~5% of high myopia); can be complicated by MNV |
| Subretinal "coin" haemorrhage | Arise from lacquer cracks in the absence of MNV |
| Fuchs spot | Raised circular pigmented macular lesion after haemorrhage absorption |
| Posterior staphyloma | Peripapillary or macular ectasia of the posterior sclera in ~1/3 of pathological myopia cases; associated with macular hole and dome-shaped macula |
| Anomalous optic nerve head | Tilted disc, peripapillary chorioretinal atrophy (temporal crescent), acquired optic disc pit |
| Lattice degeneration | Peripheral predisposition to retinal tears |
| Rhegmatogenous RD | Much more common due to PVD, lattice, atrophic holes, myopic macular holes |
Complications
1. Myopic Macular Neovascularization (MNV)
- Occurs in ~10% of highly myopic eyes
- Prognosis is better in younger patients compared to age-related MNV/AMD
2. Macular Retinoschisis (Foveoschisis)
- Occurs in highly myopic eyes with posterior staphyloma, likely due to vitreous traction
- Can be mistaken clinically for cystoid macular oedema (CMO); better characterized by OCT
3. Myopic Macular Hole
- Can occur spontaneously or after mild trauma
- Associated with a much higher rate of rhegmatogenous RD than idiopathic macular hole
- May be part of the same pathological spectrum as macular retinoschisis
4. Associated Ocular Conditions
- Cataract: posterior subcapsular or early-onset nuclear sclerosis (can paradoxically increase myopic error)
- Glaucoma: increased prevalence of primary open-angle glaucoma, pigmentary glaucoma, and steroid responsiveness
- Lens dislocation: rare but recognized risk
- Amblyopia: if significant anisometropia is present
Treatment
Slowing Myopia Progression (Children)
| Intervention | Details |
|---|---|
| Low-dose atropine 0.01% | Instilled at bedtime; significantly slows progression. Offered to children aged 5-15 with >1 dioptre/year progression |
| High-add multifocal contact lens | +2.50D centre-distance soft multifocal lens in children aged 7-11 with <5D myopia; BLINK trial confirms dose-dependent slowing |
| Outdoor activity | Encouragement to spend more time outdoors in sunshine |
Myopic MNV
- Anti-VEGF intravitreal injections are the treatment of choice
- Agents include ranibizumab, bevacizumab, and aflibercept
- Injection frequency is generally less than required for AMD
- RD risk is higher than in AMD, requiring caution
- Photodynamic therapy (PDT) with verteporfin is a historical option, still used in some predominantly classic MNV cases; verteporfin is given intravenously prior to laser activation (Goodman & Gilman's, p.1194-1197)
Myopic Macular Retinoschisis / Macular Hole
- Vitrectomy may be effective for both macular retinoschisis and myopic macular hole; however, the optimal surgical technique remains undefined
- Macular hole with associated RD requires prompt surgical intervention given the high detachment risk
Retinal Detachment
- Managed surgically (scleral buckle, vitrectomy, or pneumatic retinopexy depending on the configuration)
Refractive Correction
- Spectacles, contact lenses, or refractive surgery (LASIK, phakic IOLs) for correction of the underlying refractive error - these do not halt structural progression
Systemic Associations to Screen For
Down syndrome, Marfan syndrome, Stickler syndrome, Ehlers-Danlos syndrome, Noonan syndrome, Pierre-Robin syndrome, and prematurity.
Recent Evidence: A 2024 network meta-analysis (PMID 37950753) on myopic CNV treatment and a 2024 systematic review on differential diagnosis of mCNV (PMID 38060000) confirm anti-VEGF as the standard of care, with ranibizumab having the strongest evidence base for myopic CNV specifically.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach (10th ed.), Goodman & Gilman's The Pharmacological Basis of Therapeutics
For 15 marks with separate headings
Here is a structured 15-mark answer on pathological myopia:
Pathological Myopia
(Degenerative / High Myopia)
1. Definition
Pathological or degenerative myopia is a condition characterized by progressive anteroposterior elongation of the globe (axial length >26 mm) associated with a refractive error exceeding -6 dioptres, leading to secondary structural ocular changes due to mechanical stretching of ocular tissues. It is a significant cause of legal blindness worldwide.
2. Epidemiology
- Affects >2% of adult Western European/American populations
- Up to ~10% in East Asian populations
- Maculopathy is the most common cause of visual loss
- Strong hereditary component with environmental contribution (prolonged near work, limited outdoor activity)
3. Pathogenesis
The primary event is scleral remodelling and progressive axial elongation, which mechanically stretches the choroid, Bruch's membrane, RPE, and neurosensory retina. This leads to:
- Thinning and atrophy of the RPE and choriocapillaris
- Ruptures in Bruch's membrane (lacquer cracks)
- Mechanical traction at the vitreoretinal interface
- Formation of posterior staphyloma (focal scleral ectasia)
4. Systemic Associations
High myopia is associated with several systemic conditions:
- Marfan syndrome
- Stickler syndrome
- Down syndrome
- Ehlers-Danlos syndrome
- Noonan syndrome
- Pierre-Robin syndrome
- Prematurity
5. Fundus (Clinical) Features
| Finding | Description |
|---|---|
| Tessellated fundus | Diffuse RPE attenuation exposing large choroidal vessels |
| Focal chorioretinal atrophy | Patchy RPE/choriocapillaris loss; bare sclera visible |
| Lacquer cracks | Fine, irregular yellow lines at the posterior pole from Bruch's membrane rupture; seen in ~5% of high myopes |
| Subretinal "coin" haemorrhage | From lacquer cracks without MNV |
| Fuchs spot | Raised pigmented macular scar after haemorrhage resolves |
| Posterior staphyloma | Posterior scleral ectasia; present in ~1/3 of cases; associated with macular hole and dome-shaped macula |
| Tilted/anomalous optic disc | With peripapillary chorioretinal atrophy (temporal crescent) |
| Lattice degeneration | Peripheral retinal thinning predisposing to tears |
6. Complications
a) Myopic Macular Neovascularization (MNV)
- Occurs in ~10% of highly myopic eyes
- Subretinal neovascular membrane arising from Bruch's membrane rupture
- Presents with sudden decrease in vision, metamorphopsia
b) Macular Retinoschisis (Foveoschisis)
- Splitting within retinal layers due to vitreous traction in eyes with posterior staphyloma
- Mimics CMO clinically; best diagnosed with OCT
c) Myopic Macular Hole
- May occur spontaneously or after mild trauma
- Much higher risk of rhegmatogenous RD compared to idiopathic macular hole
- Shares a pathological spectrum with macular retinoschisis
d) Rhegmatogenous Retinal Detachment
- Increased risk due to PVD, lattice degeneration, atrophic holes, and macular holes
e) Cataract
- Posterior subcapsular or early-onset nuclear sclerosis
- Nuclear sclerosis can paradoxically increase the myopic refractive error
f) Glaucoma
- Increased prevalence of primary open-angle glaucoma, pigmentary glaucoma, and steroid responsiveness
g) Lens dislocation - rare but recognized complication
7. Investigations
- OCT: gold standard for macular retinoschisis, foveoschisis, macular hole, dome-shaped macula, and MNV
- Fundus fluorescein angiography (FFA): identifies active MNV
- OCT-Angiography (OCTA): non-invasive detection of MNV
- B-scan ultrasonography / MRI: demonstrates posterior staphyloma
- Visual fields: to assess for associated glaucomatous damage
8. Treatment
A. Slowing Myopia Progression (Children)
| Intervention | Details |
|---|---|
| Low-dose atropine 0.01% | Nightly instillation; offered to children aged 5-15 with progression >1 D/year; significantly slows axial elongation |
| High-add multifocal contact lens | +2.50D centre-distance soft lens in children aged 7-11 with <5D myopia; BLINK trial confirms dose-dependent slowing |
| Outdoor activity | Increased time in sunlight reduces progression risk |
| Orthokeratology | Overnight rigid lenses that flatten the cornea; shown to reduce axial elongation |
B. Myopic MNV
- Anti-VEGF intravitreal injections are the first-line treatment of choice
- Ranibizumab, bevacizumab, or aflibercept
- Injection frequency is generally less than in AMD
- Prognosis is better in younger patients than in AMD-related MNV
- RD risk is higher than in AMD - monitor closely
- Photodynamic therapy (PDT) with verteporfin - historical option; still used for predominantly classic MNV where anti-VEGF is unavailable or contraindicated; verteporfin is given IV then activated by laser
C. Macular Retinoschisis / Macular Hole
- Pars plana vitrectomy (PPV) with or without internal limiting membrane (ILM) peeling
- Effective for both macular retinoschisis and myopic macular hole
- Optimal surgical technique (gas tamponade, ILM peeling extent) remains debated
- Macular hole with RD requires urgent surgery
D. Retinal Detachment
- Surgical repair: scleral buckle, PPV, or pneumatic retinopexy depending on configuration
- High myopes tend to have more complex detachments requiring PPV
E. Cataract
- Phacoemulsification with IOL implantation; choice of IOL power requires careful biometry in abnormally long eyes
F. Glaucoma
- Managed with topical IOP-lowering agents; screen regularly given increased risk
G. Refractive Correction
- Spectacles or contact lenses for symptom correction
- Refractive surgery (LASIK, phakic IOL implantation) corrects the refractive error but does not halt progressive axial elongation or structural damage
9. Prognosis
- Progressive condition with no cure for the underlying scleral elongation
- Visual prognosis depends on the severity of macular involvement
- MNV in younger patients responds well to anti-VEGF with relatively fewer injections needed compared to AMD
- Posterior staphyloma and geographic atrophy carry a guarded long-term prognosis
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach (10th ed.) | Goodman & Gilman's Pharmacological Basis of Therapeutics | PMID 37950753 (Network meta-analysis, mCNV treatment, 2024)
This is a shared conversation. Sign in to Orris to start your own chat.